Diplopia in details
Reading File
Finding Sources
Finding Sources
Searching PubMed
diplopia etiology evaluation management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive material from multiple authoritative textbooks. Let me compile the detailed answer:
Diplopia (Double Vision) - A Comprehensive Overview
Definition
Diplopia is the perception of two images from a single object. It is classified primarily as monocular or binocular, a distinction that immediately narrows the differential diagnosis and guides the workup.
- Monocular diplopia: Persists when the fellow eye is closed. Caused by local ocular pathology.
- Binocular diplopia: Resolves when either eye is covered. Caused by misalignment of the visual axes. This is the clinically significant, potentially dangerous type.
Pathophysiology
Normal binocular vision depends on perfect coordination of six extraocular muscles in each eye, controlled by cranial nerves III, IV, and VI, orchestrated via the medial longitudinal fasciculus (MLF) in the brainstem. Any disruption - from muscle, neuromuscular junction, nerve, nucleus, or supranuclear pathway - can cause the visual axes to diverge, projecting the image of an object onto non-corresponding retinal points, resulting in two perceived images.
Classification
1. Monocular Diplopia
- Persists with the other eye closed
- Causes:
- Uncorrected refractive error (most common; resolves with pinhole)
- Cataract
- Corneal aberration (keratoconus, pterygium)
- Lens subluxation (does NOT resolve with pinhole)
- Retinal abnormality / epiretinal membrane (does NOT resolve with pinhole)
- Foveal traction
- Occasionally: malingering or psychiatric disease
- Key test: Pinhole - if diplopia resolves, the cause is refractive; if it persists, consider lens or retinal pathology
2. Binocular Diplopia
Resolves when either eye is closed. Has an extensive differential. Further classified by direction:
- Horizontal diplopia: Impaired abduction or adduction (CN VI or medial rectus dysfunction)
- Vertical or oblique diplopia: Superior/inferior rectus or oblique dysfunction (CN III or IV)
- Torsional diplopia: Oblique muscle dysfunction (especially CN IV)
Extraocular Muscle Actions (Key Reference)
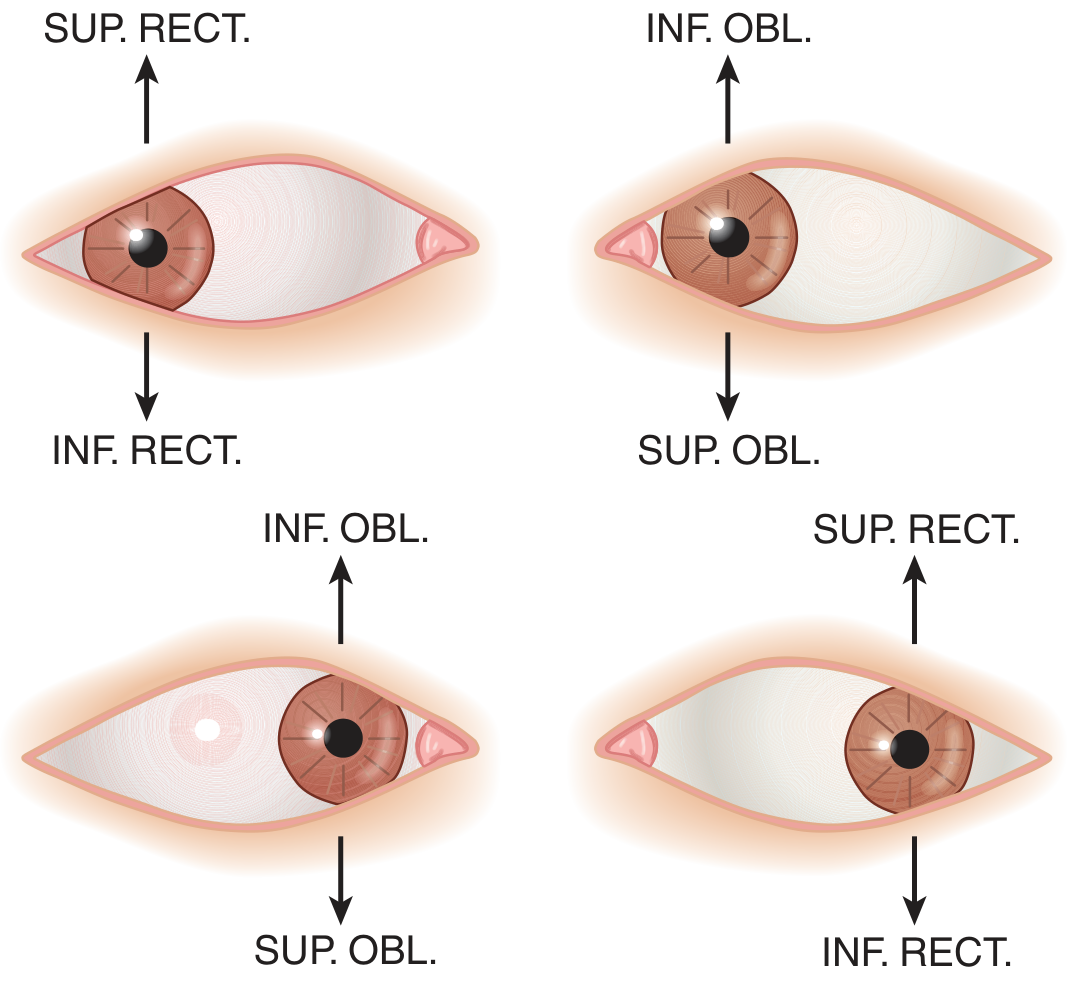
When the eye is abducted: main elevator = Superior Rectus, main depressor = Inferior Rectus. When the eye is adducted: main elevator = Inferior Oblique, main depressor = Superior Oblique.
Causes of Binocular Diplopia - Systematic Approach
Level 1: Orbit / Extraocular Muscles (Restrictive/Mechanical)
| Cause | Key Features |
|---|---|
| Thyroid eye disease (Graves) | Most commonly affects inferior and medial recti - restricts elevation and abduction. Proptosis, lid retraction, chemosis |
| Orbital blowout fracture | Inferior rectus entrapment - restricted upgaze with enophthalmos after trauma |
| Orbital myositis / pseudotumor | Pain, proptosis, restricted motility; may be idiopathic or due to giant cell arteritis (older patient + headache + jaw claudication) |
| Orbital cellulitis / abscess | Fever, periorbital swelling, pain |
| Orbital tumors / metastases | Progressive, painless, associated mass effect |
Restrictive orbitopathy causes mechanical diplopia - worse when looking into the restricted direction. Signs: proptosis, periorbital swelling, conjunctival hyperemia.
Level 2: Neuromuscular Junction
Myasthenia Gravis
- Major cause of painless binocular diplopia
- Ptosis + diplopia that worsens with fatigue, improves with rest or ice
- Pupils always normal (key distinguishing feature)
- Intermittent and variable - does not conform to any single CN distribution
- Purely ocular form common (no systemic weakness)
- Confirm with: anti-AChR or anti-MuSK antibodies, ice test, repetitive nerve stimulation, single-fiber EMG
- Botulism (food/wound poisoning) can mimic ocular myasthenia
Level 3: Cranial Nerve Palsies
CN III (Oculomotor) Palsy
- Innervates: medial rectus, superior rectus, inferior rectus, inferior oblique, levator palpebrae superioris, pupillary constrictor
- Classic findings: Eye deviated "down and out" (unopposed lateral rectus + superior oblique), ptosis, dilated pupil
- Diplopia in all directions EXCEPT lateral gaze to the affected side
- Pupil involvement = compressive lesion until proven otherwise (aneurysm - posterior communicating artery, tumor, herniation)
- Pupil sparing = microvascular ischemia (diabetes, hypertension) - rule of thumb, not absolute
- Urgent neuroimaging + CTA/MRA if pupil involved, especially if painful
Midbrain syndromes causing CN III palsy:
| Syndrome | Lesion Site | Signs |
|---|---|---|
| Weber's | Cerebral peduncle | Ipsilateral CN III + contralateral hemiparesis |
| Benedikt's | Red nucleus | Ipsilateral CN III + contralateral tremor/chorea |
| Nothnagel's | Superior cerebellar peduncle | Ipsilateral CN III + contralateral cerebellar ataxia |
| Claude's | Red nucleus + SCP | Combines Benedikt + Nothnagel |
Nuclear CN III palsy: Bilateral ptosis (central subnucleus) + contralateral superior rectus weakness
CN IV (Trochlear) Palsy
- Supplies: superior oblique only
- Longest intracranial course; only nerve to exit from dorsal brainstem
- Vertical or torsional diplopia, worse looking down and nasally (e.g., reading, descending stairs)
- Patient tilts head away from affected side (Bielschowsky head tilt)
- Most commonly caused by trauma (contrecoup injury to the nerve at the dorsal midbrain)
- Also: congenital, microvascular, idiopathic
- Park's three-step test used for diagnosis
CN VI (Abducens) Palsy
- Supplies: lateral rectus only
- Horizontal diplopia, worse on gaze toward the affected side
- Affected eye deviates medially (esotropia)
- Most common isolated ocular motor palsy
- Long intracranial course = "false localizing sign" - raised ICP can stretch the nerve
- Causes: microvascular (DM, HTN), elevated ICP, tumor (pontine glioma), trauma, Wernicke encephalopathy, basilar meningitis
Level 4: Brainstem / Supranuclear
Internuclear Ophthalmoplegia (INO)
- Lesion in the Medial Longitudinal Fasciculus (MLF) in the pons
- Failure of adduction in the ipsilateral eye during horizontal gaze to the contralateral side, with nystagmus in the abducting eye
- Convergence is often preserved (differentiates from CN III palsy)
- Most common cause in young patients: Multiple sclerosis (often bilateral)
- Most common cause in older patients: Brainstem infarction
- "WEBINO" = Wall-Eyed Bilateral INO (bilateral adduction failure)
- "ONE and a HALF syndrome" = ipsilateral gaze palsy + ipsilateral INO (lesion in ipsilateral PPRF + MLF)
Other Brainstem Causes
- Basilar artery thrombosis (vertical gaze palsy, coma - critical emergency)
- Pontine glioma
- Wernicke encephalopathy (CN VI palsy + INO + altered consciousness + ataxia)
- Miller Fisher syndrome (ophthalmoplegia + areflexia + ataxia; anti-GQ1b antibodies)
- Ophthalmoplegic migraine
Level 5: Cavernous Sinus / Orbital Apex
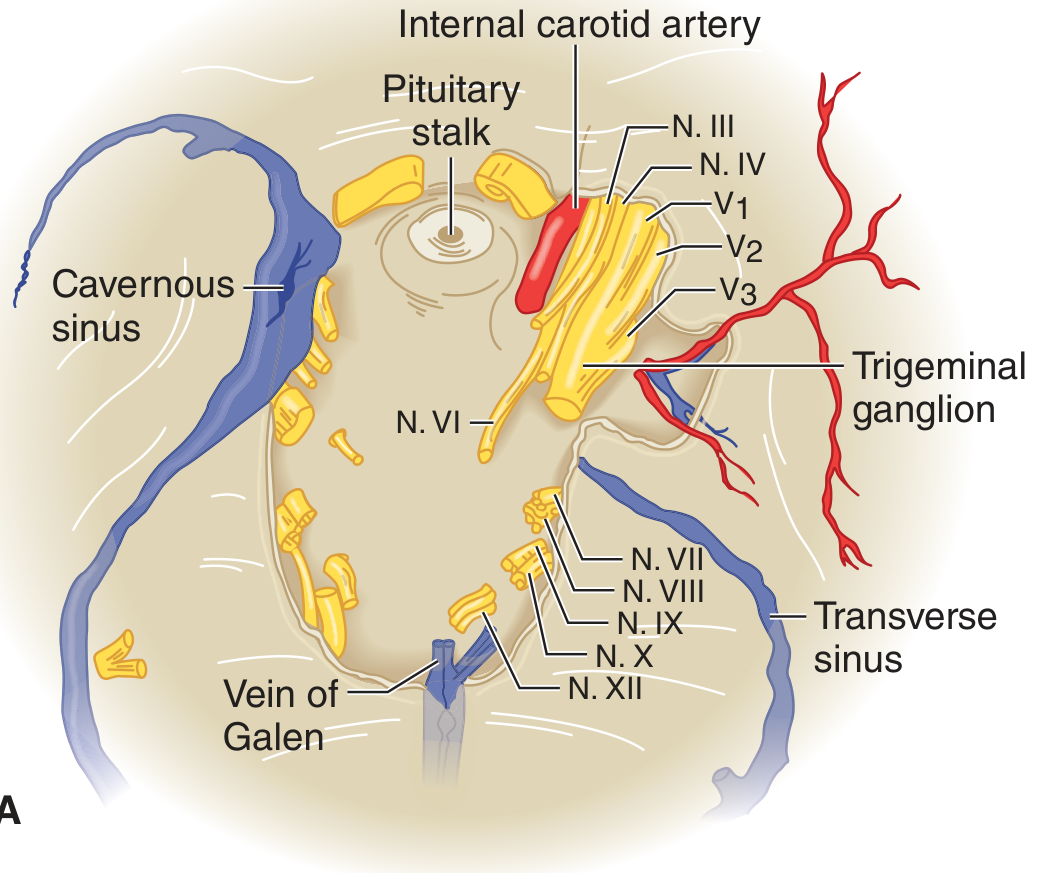
Any process in the cavernous sinus can affect CN III, IV, VI (and V1, V2) simultaneously:
- Cavernous sinus thrombosis: Fever, proptosis, chemosis, periorbital pain
- Carotid-cavernous fistula: Pulsating proptosis, chemosis, bruit
- Tolosa-Hunt syndrome: Painful ophthalmoplegia, steroid-responsive
- Pituitary adenoma or meningioma: Painless, progressive
- Herpes zoster: Vesicular eruption in V1 distribution + ophthalmoplegia
Priority Diagnoses (Urgency Tiers)
Tier 1 - Critical (Life-Threatening)
| Diagnosis | Key Feature | Action |
|---|---|---|
| Basilar artery thrombosis | Vertigo, dysarthria, other CN signs, coma | Emergency CTA + thrombectomy |
| Posterior communicating artery aneurysm | CN III palsy with pupil dilation + pain | Urgent CTA/MRA |
| Botulism | Descending paralysis, dysarthria, dysphagia, autonomic dysfunction | ICU, antitoxin |
| Basilar meningitis | Headache, meningismus, fever | LP, antibiotics |
Tier 2 - Emergent
- Vertebral artery dissection (neck pain + vertigo)
- Myasthenia gravis crisis (respiratory compromise)
- Cavernous sinus thrombosis
- Wernicke encephalopathy (thiamine deficiency)
Tier 3 - Urgent
- CN III/IV/VI palsies (microvascular)
- Multiple sclerosis
- Thyroid eye disease
- Stroke / TIA
Diagnostic Approach
History
- Monocular or binocular? (Ask patient to cover each eye)
- Direction of diplopia: horizontal, vertical, oblique, torsional?
- Onset: sudden (vascular) vs. gradual (neoplastic, inflammatory)?
- Constant or intermittent? Fatiguable (myasthenia)?
- Pain? (Compressive CN III, Tolosa-Hunt, giant cell arteritis, cavernous sinus thrombosis)
- Associated symptoms: ptosis, pupil change, headache, vertigo, weakness, neck pain?
- Diurnal variation? (worse in evening = myasthenia)
- Risk factors: DM, HTN, smoking (microvascular), trauma, cancer history, autoimmune disease
Examination
- Cover test - establishes monocular vs. binocular; reveals deviation in primary gaze
- Extraocular movements - identify the weak muscle/nerve
- Pupils - dilation = compressive CN III; sparing = microvascular
- Ptosis - CN III, myasthenia, Horner syndrome
- Proptosis/chemosis - orbital disease
- Fatigability test - sustained upgaze ptosis = myasthenia
- Ice test - ice pack over eye for 2 minutes; improvement in ptosis/diplopia = myasthenia
- Head tilt test (Bielschowsky) - for CN IV palsy
- Pinhole test - for monocular diplopia
Investigation
- All binocular diplopia: MRI brain (with brainstem sequences) ± gadolinium
- Pupil-involved CN III: Urgent CTA/MRA to exclude posterior communicating artery aneurysm
- Suspected myasthenia: Anti-AChR/MuSK antibodies, repetitive nerve stimulation, chest CT (thymoma)
- Orbital disease: Dedicated orbital MRI with fat saturation + gadolinium
- Thyroid eye disease: TFTs, TSH receptor antibodies
- Giant cell arteritis: ESR, CRP, temporal artery biopsy
- Wernicke: Thiamine levels, empiric thiamine infusion
- Miller Fisher: Anti-GQ1b antibodies
Treatment
Treatment is directed at the underlying cause. Symptomatic options include:
| Modality | Use |
|---|---|
| Occlusion (patching) | Acute phase - eliminates one image; alternate eyes in children <6 years to prevent amblyopia |
| Fresnel prisms | If deviation is not too large; useful for stable, comitant deviations |
| Botulinum toxin injection | Into antagonist muscle; helpful in acute abducens palsy (especially bilateral/traumatic); effects last 3-4 months; complications: ptosis, worsening diplopia, dry eye |
| Strabismus surgery | After at least 6 months of stable alignment; for long-standing deviation |
| Orthoptic exercises | Convergence insufficiency |
| Treat etiology | Thiamine for Wernicke; steroids for Tolosa-Hunt/GCA; immunotherapy for myasthenia; surgical clipping/coiling for aneurysm; decompression for thyroid eye disease |
Special Patterns to Recognize
| Pattern | Think of |
|---|---|
| Painless, fatigable ptosis + diplopia, variable | Myasthenia gravis |
| CN III palsy + dilated pupil + pain | Posterior communicating artery aneurysm |
| CN III palsy + pupil sparing | Microvascular ischemia (DM/HTN) |
| Bilateral INO | Multiple sclerosis |
| CN VI palsy + raised ICP signs | False localizing sign |
| Ophthalmoplegia + areflexia + ataxia | Miller Fisher syndrome |
| Ophthalmoplegia + jaw claudication + elderly patient | Giant cell arteritis |
| Descending ophthalmoplegia + autonomic signs | Botulism |
| Ophthalmoplegia + encephalopathy + ataxia | Wernicke encephalopathy |
| Proptosis + chemosis + pain + fever | Cavernous sinus thrombosis |
Sources
- Rosen's Emergency Medicine, 10th Ed. - Chapter 17: Diplopia
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025) - Chapter 34: Double Vision
- Adams and Victor's Principles of Neurology, 12th Ed. - Chapter 13: Diplopia and Strabismus
- Bradley and Daroff's Neurology in Clinical Practice - Chapter 18: Diplopia and Treatment
- Neuroanatomy through Clinical Cases, 3rd Ed. - Section 13.1
This is a shared conversation. Sign in to Orris to start your own chat.