Thyroid gland anatomy and physiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks along with excellent diagrams. Let me compile the full answer.
Thyroid Gland: Anatomy and Physiology
1. Overview and Gross Anatomy
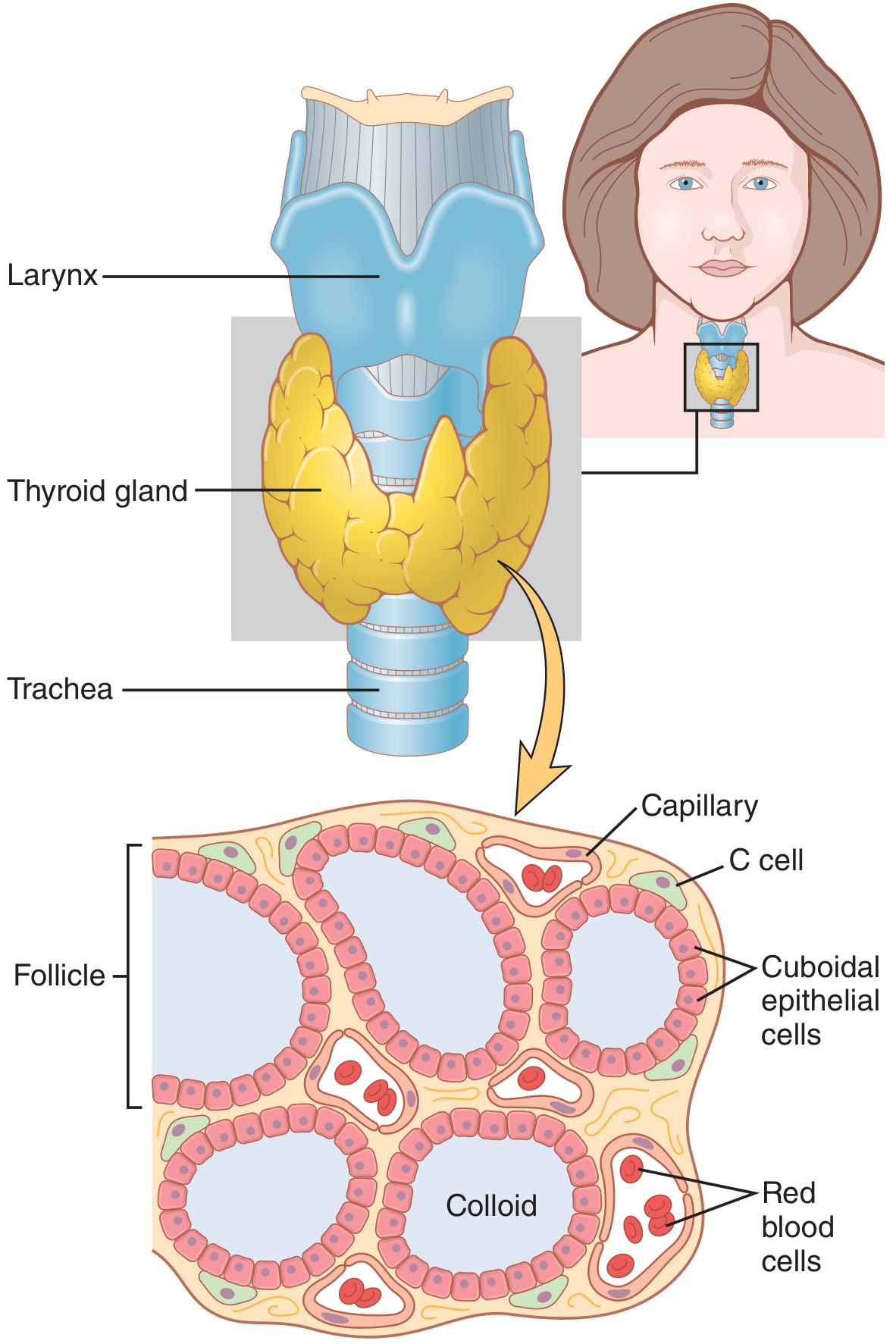
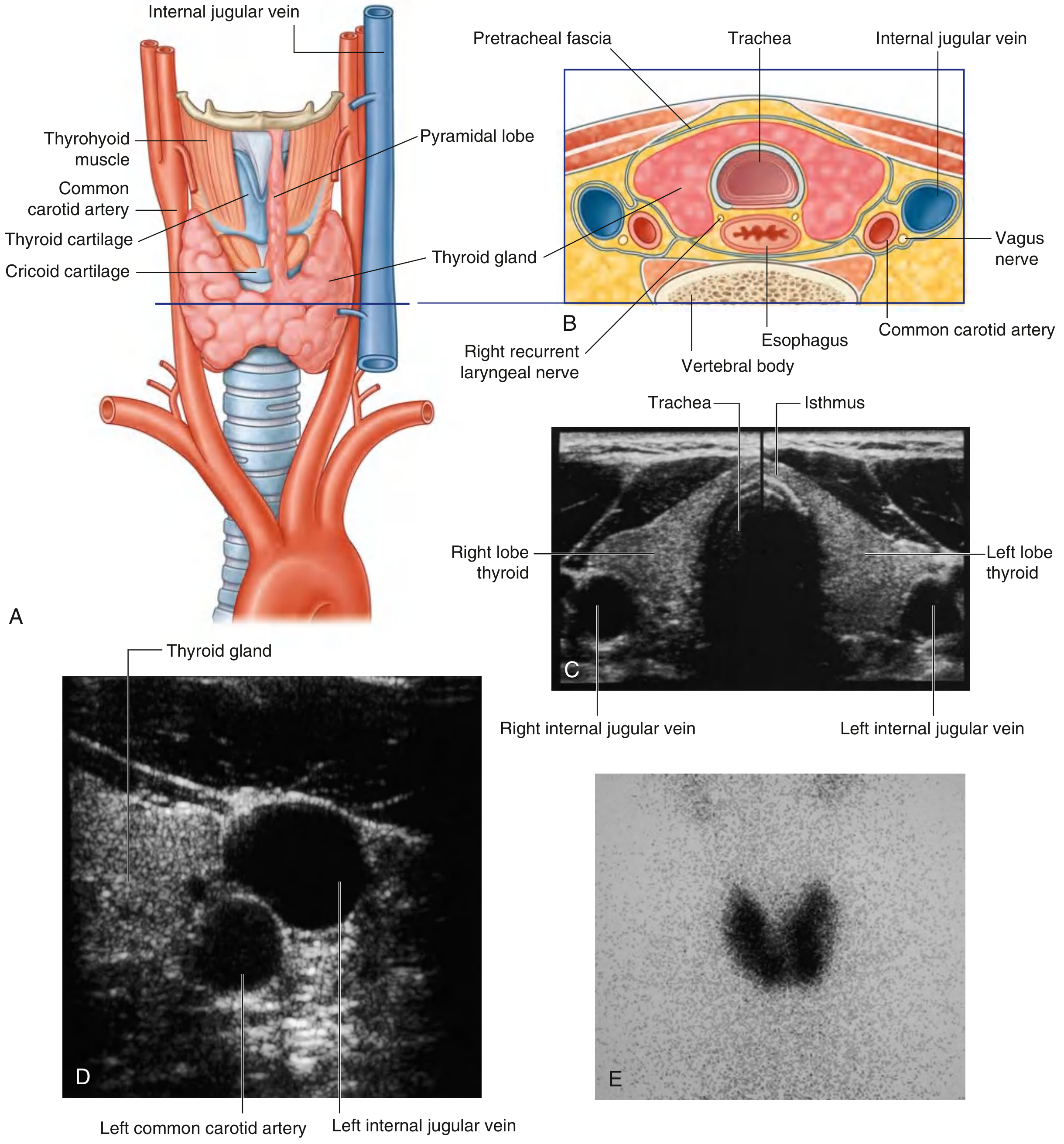
The thyroid is a butterfly-shaped, highly vascular endocrine gland located in the anterior neck, just below the larynx and anterior to the trachea. It consists of two lateral lobes connected by a midline isthmus, which crosses the anterior surface of the 2nd and 3rd tracheal cartilages. A pyramidal lobe may extend superiorly from the isthmus in approximately 50% of individuals - a remnant of the thyroglossal duct.
- Weight: ~20-30 g in adults
- Relations: Lies deep to the sternohyoid, sternothyroid, and omohyoid muscles (infrahyoid "strap" muscles), within the pretracheal fascia of the visceral compartment of the neck
- Gray's Anatomy for Students, p. 1157
2. Embryology
The thyroid originates from median and lateral thyroid anlagenes - embryologic precursor tissues from the foregut endoderm near the base of the tongue. The site of origin is marked by the foramen cecum at the posterior tongue. The gland descends through the neck along the thyroglossal duct, which normally disappears early in development.
Remnants may persist as:
-
Thyroglossal duct cyst (midline neck mass, most common anomaly)
-
Thyroglossal duct fistula (connection to foramen cecum)
-
Lingual thyroid (ectopic thyroid at the tongue base)
-
Ectopic thyroid tissue anywhere along the path of migration
-
Sabiston Textbook of Surgery, p. 1488; Gray's Anatomy for Students, p. 1157
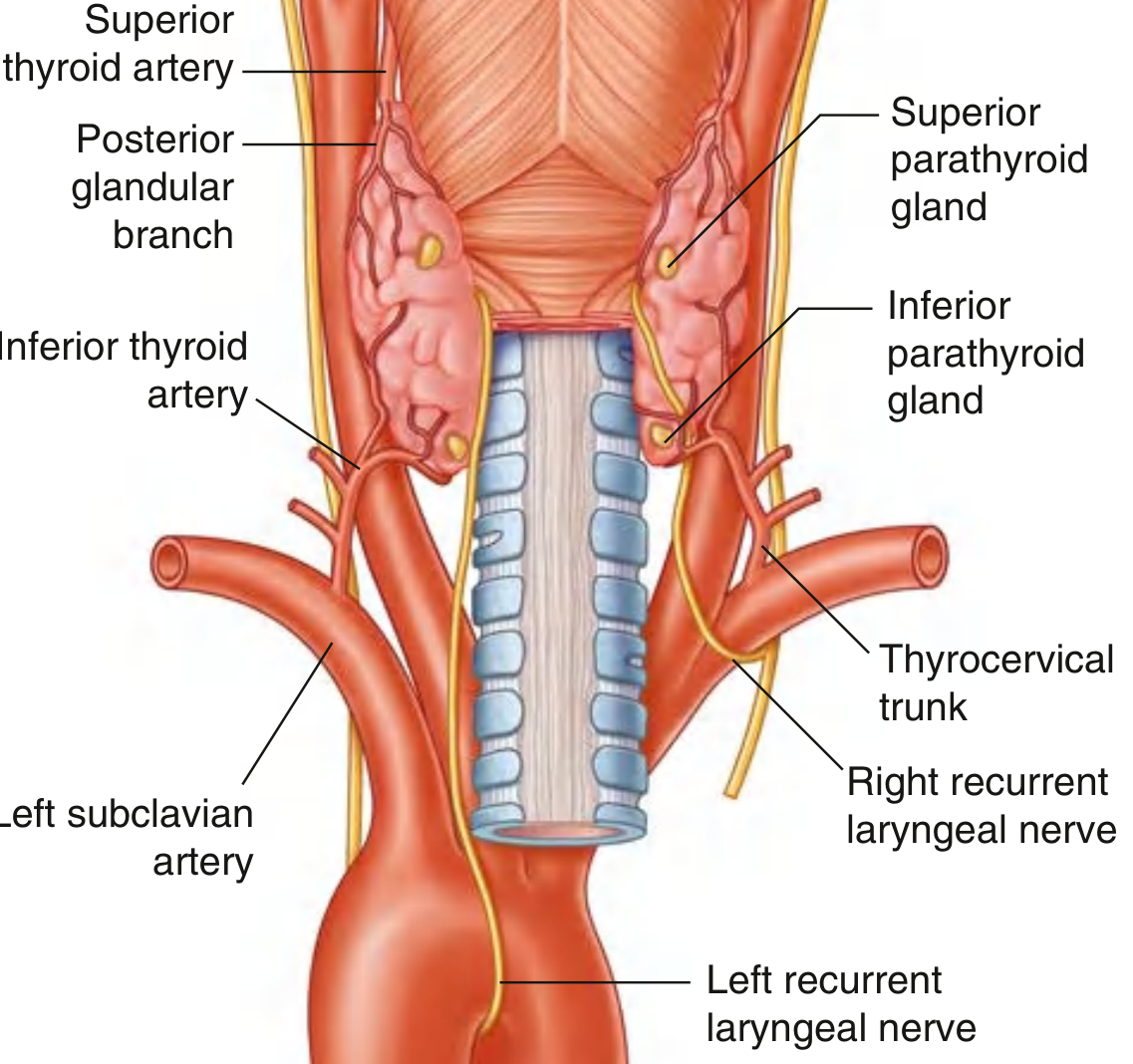
3. Arterial Supply
Two major paired arteries supply the thyroid:
| Artery | Origin | Supplies |
|---|---|---|
| Superior thyroid artery | First branch of the external carotid artery | Superior pole of each lateral lobe; branches into anterior and posterior glandular branches |
| Inferior thyroid artery | Thyrocervical trunk (from 1st part of subclavian artery) | Lower thyroid, parathyroid glands via ascending branch |
- Occasionally a thyroid ima artery arises from the brachiocephalic trunk or aortic arch and ascends on the trachea's anterior surface to supply the gland.
- Gray's Anatomy for Students, p. 1158-1159
4. Venous Drainage
Three veins drain the thyroid:
- Superior thyroid vein - drains area of superior thyroid artery supply → internal jugular vein
- Middle thyroid vein - drains lateral lobes → internal jugular vein
- Inferior thyroid veins (paired) - drain inferior pole → right and left brachiocephalic veins respectively
5. Lymphatic Drainage
Lymphatics drain to:
- Paratracheal nodes (alongside the trachea)
- Deep cervical nodes inferior to the omohyoid, along the internal jugular vein
This drainage pattern is important in understanding the spread of thyroid cancers.
6. Nerve Supply and Key Surgical Relationships
The thyroid gland has two clinically important nerve relationships:
-
Recurrent laryngeal nerves (RLN): Branch from vagus [CN X]; right RLN loops around the right subclavian artery, left RLN loops around the aortic arch. Both ascend in the tracheo-esophageal groove and pass deep to the posteromedial surface of the thyroid lobes. They enter the larynx deep to the inferior pharyngeal constrictor. Injury during thyroidectomy causes hoarseness or voice loss.
-
External branch of the superior laryngeal nerve (EBSLN): Runs close to the superior thyroid vessels at the superior pole. Injury causes loss of high-pitched voice.
-
Gray's Anatomy for Students, p. 1159; Sabiston Textbook of Surgery
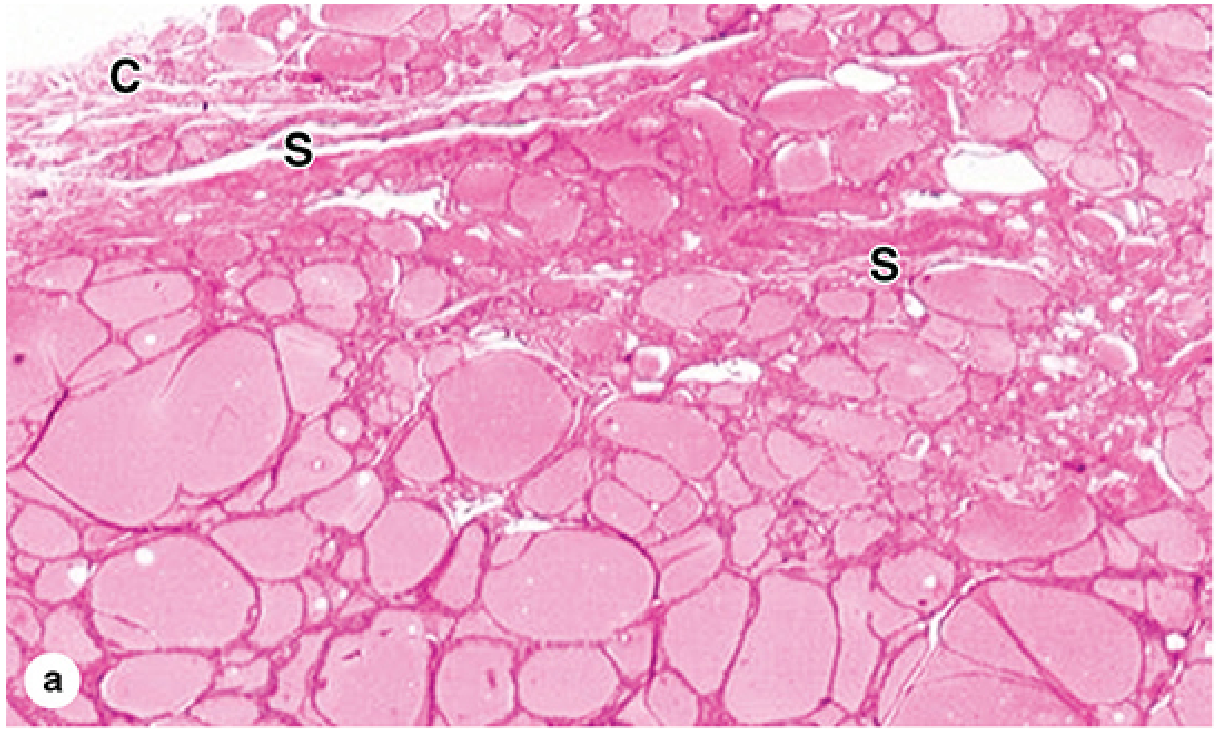
7. Histology
The thyroid is unique in storing its secretory product outside the cells, in the colloid of follicle lumens.
Two cell types:
Follicular Cells (Thyrocytes)
- The predominant cell type (~99%)
- Arranged into spherical follicles (100-300 µm diameter) filled with gelatinous, acidophilic colloid
- Cell shape varies with activity: squamous/flat = hypoactive; low columnar = active
- Activity controlled by TSH
- Function: synthesis and secretion of T3 and T4
Parafollicular C Cells
- Located in the interfollicular stroma, mainly in the lateral mid/upper thyroid lobes
- Secrete calcitonin
- Do not contact the follicle lumen
Structural organization:
- Covered by a fibrous capsule with septa that extend inward to form lobules
- Septa carry blood vessels, nerves, and lymphatics
- Follicles separated by sparse reticular connective tissue with richly fenestrated capillaries
The thyroid is the only endocrine gland that stores a large quantity of its secretory product - enough hormone in follicles to supply the body for up to 3 months without additional synthesis.
- Junqueira's Basic Histology, p. 1034-1035; Sabiston Textbook of Surgery, p. 1489
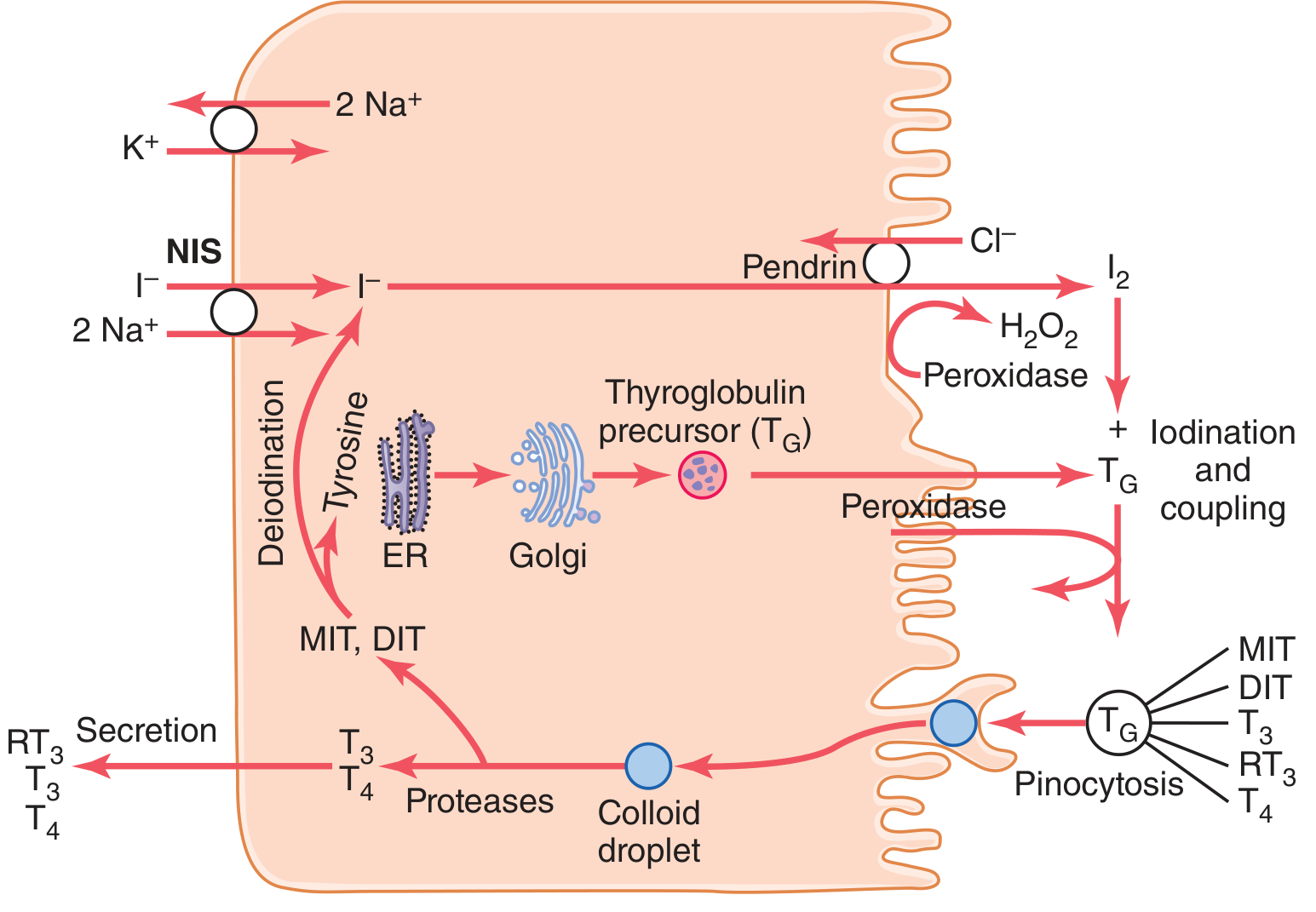
8. Thyroid Hormone Synthesis
The synthesis process occurs within the follicle unit and requires iodine.
Step-by-Step Synthesis:
Step 1 - Iodide Trapping (NIS pump)
Follicular cells actively transport iodide from blood into the cytoplasm via the Na⁺/I⁻ symporter (NIS) at the basolateral membrane. Energy comes from Na⁺-K⁺-ATPase. The thyroid normally concentrates iodide ~30x blood concentration (up to 250x when maximally stimulated by TSH).
Step 2 - Iodide Transport into Colloid
Iodide moves across the apical membrane into the follicle via the Cl⁻/I⁻ counter-transporter pendrin.
Step 3 - Oxidation of Iodide
Iodide is oxidized to molecular iodine (I₂) by thyroid peroxidase (TPO) using H₂O₂ at the apical membrane.
Step 4 - Iodination of Thyroglobulin
TPO also catalyzes the iodination of tyrosine residues on thyroglobulin (Tg), a large glycoprotein (~660 kDa, ~70 tyrosine residues) synthesized in the ER/Golgi and secreted into the colloid:
- 1 iodine + tyrosine → Monoiodotyrosine (MIT)
- 2 iodines + tyrosine → Diiodotyrosine (DIT)
Step 5 - Coupling (Oxidative Coupling)
TPO couples the iodotyrosines:
- DIT + DIT → Thyroxine (T4) - contains 4 iodine atoms
- DIT + MIT → Triiodothyronine (T3) - contains 3 iodine atoms
T3 and T4 remain stored within the Tg molecule in the colloid.
Step 6 - Secretion
When stimulated (by TSH), follicular cells engulf colloid by pinocytosis/endocytosis. Lysosomes fuse with the colloid droplet, and proteases cleave T3 and T4 from Tg. Free T3 and T4 are then secreted into the bloodstream. MIT and DIT are deiodinated intracellularly, and the iodide is recycled.
- Guyton and Hall Medical Physiology, p. 930-932; Sabiston Textbook of Surgery, p. 1489
Iodine Requirements
~50 mg iodide/year (1 mg/week) is required for normal T4 production. Common table salt is iodized (1 part NaI per 100,000 parts NaCl) to prevent deficiency.
9. Plasma Transport
Upon entering the blood, >99% of T4 and T3 binds plasma proteins synthesized by the liver:
- Thyroxine-binding globulin (TBG) - main carrier
- Thyroxine-binding prealbumin (transthyretin)
- Albumin
| Hormone | Half-life in blood | Notes |
|---|---|---|
| T4 (thyroxine) | ~6-7 days | Higher protein binding affinity; "prohormone" |
| T3 | ~1 day | Lower protein binding; 4x more potent than T4 |
Most T4 is converted to T3 in peripheral tissues (liver, kidney, muscle) by 5'-deiodinase. More than 90% of thyroid hormone binding intracellular receptors is T3.
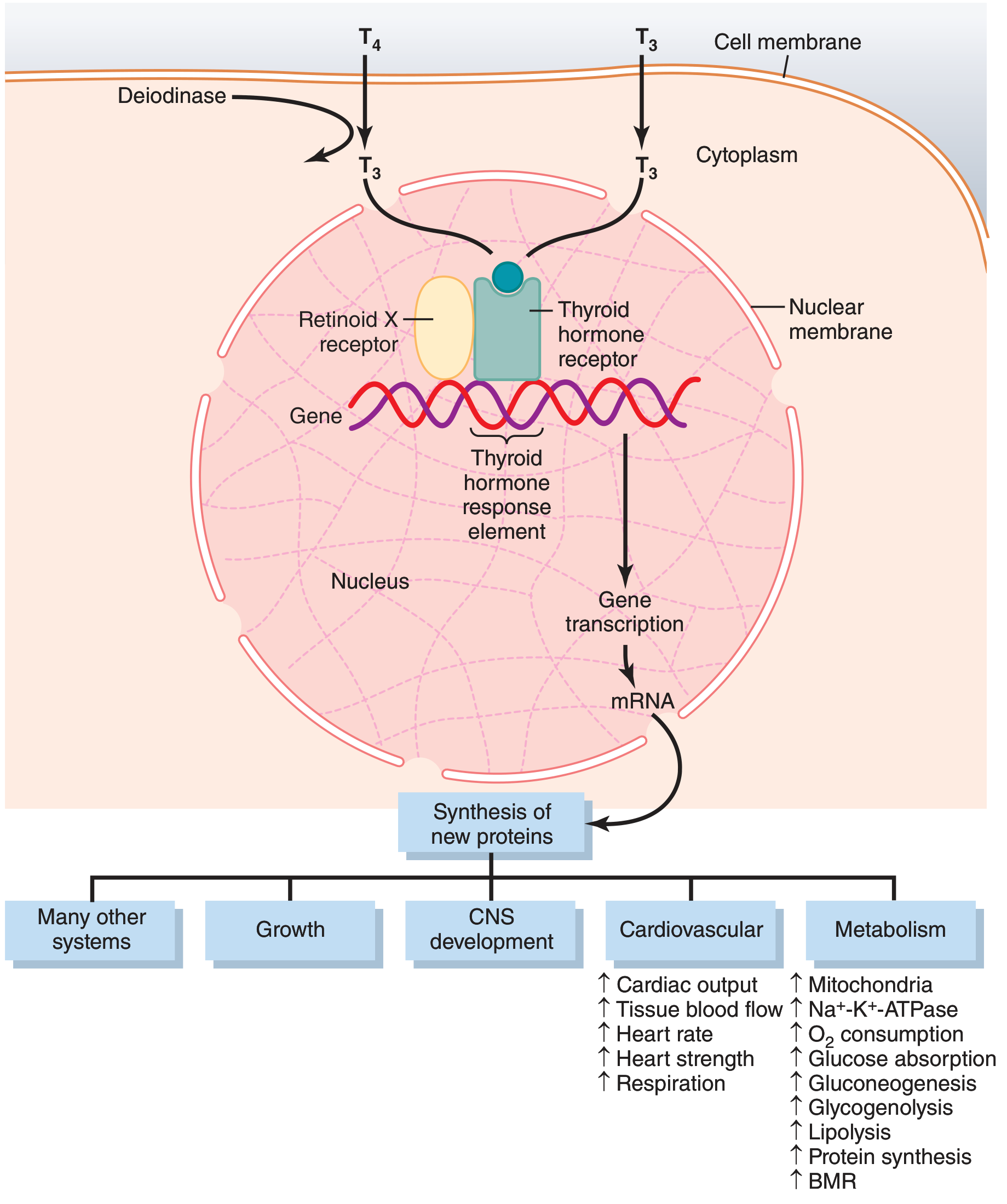
10. Mechanism of Action
T3 is the active form. It enters target cells by carrier-mediated transport and:
- Binds nuclear thyroid hormone receptors (TR)
- TR forms a heterodimer with Retinoid X Receptor (RXR)
- This complex binds the thyroid hormone response element (TRE) on DNA
- Activates or represses gene transcription
- Produces new mRNAs and hundreds of new proteins
- Net effect: generalized increase in functional activity throughout the body
There are also nongenomic (rapid) effects occurring within minutes via membrane receptors and second messengers (cAMP, kinase cascades) - too fast to be explained by changes in protein synthesis.
- Guyton and Hall Medical Physiology, p. 933-934
11. Physiological Actions of Thyroid Hormones
| System | Effect |
|---|---|
| Metabolism | ↑ BMR (60-100% above normal with excess T3/T4); ↑ Na⁺-K⁺-ATPase; ↑ mitochondria size/number; ↑ O₂ consumption |
| Carbohydrates | ↑ glucose absorption from gut; ↑ glycogenolysis; ↑ gluconeogenesis |
| Lipids | ↑ lipolysis; ↑ fatty acid oxidation; ↓ cholesterol, phospholipids, and triglycerides in blood |
| Proteins | ↑ protein synthesis AND catabolism; in excess: net catabolism |
| Cardiovascular | ↑ cardiac output; ↑ heart rate and strength; ↑ tissue blood flow; ↑ respiration rate |
| CNS | ↑ rapidity of cerebration; excitability, anxiety (excess); sluggishness, somnolence (deficiency); essential for normal brain development in fetus |
| Growth | Accelerates growth in young people; promotes bone maturation |
| GI tract | ↑ motility; ↑ digestive juice secretion; diarrhea (excess) vs. constipation (deficiency) |
| Muscle | Mild excess → vigor; severe excess → weakness (protein catabolism); deficiency → sluggish contraction/relaxation |
| Reproductive | Required for normal gonadal function; hypothyroidism → menorrhagia, infertility; hyperthyroidism → oligomenorrhea |
| Other endocrine glands | ↑ insulin need; ↑ PTH need; ↑ glucocorticoid degradation → ↑ ACTH/cortisol |
- Guyton and Hall Medical Physiology, p. 934-937
12. Hypothalamic-Pituitary-Thyroid (HPT) Axis - Regulation
Feedback loop:
Hypothalamus (PVN)
↓ TRH (thyrotropin-releasing hormone)
Anterior Pituitary
↓ TSH (thyrotropin, glycoprotein ~28 kDa)
Thyroid Gland
↓ T3 + T4
Peripheral tissues
↑ T3/T4 → NEGATIVE FEEDBACK to hypothalamus and pituitary
TSH Actions on the Thyroid (via TSH receptor → G protein → adenylyl cyclase → cAMP → protein kinase):
- ↑ Proteolysis of stored thyroglobulin → immediate hormone release (within 30 min)
- ↑ NIS activity (iodide trapping - up to 8x normal)
- ↑ Iodination of tyrosine
- ↑ Cell size and secretory activity
- ↑ Cell number (cuboidal → columnar → infolding of epithelium)
TRH is a tripeptide secreted from the paraventricular nucleus of the hypothalamus into the portal circulation → anterior pituitary → binds thyrotroph receptors → TSH release.
Negative feedback: Rising T3/T4 suppresses both TRH release from hypothalamus and TSH release from pituitary. This is the basis of TSH testing in clinical practice - a low TSH indicates excess circulating thyroid hormone.
- Guyton and Hall Medical Physiology, p. 937-938
13. Calcitonin
Secreted by parafollicular C cells, calcitonin is a 32-amino acid polypeptide regulated by serum calcium (not TSH).
Actions (lowering blood calcium):
- Bone: ↑ osteoblast activity; ↓ osteoclast activity
- Kidney: ↑ urinary calcium excretion
- Gut: ↓ calcium absorption
Its physiological significance is minor (absence does not noticeably alter calcium homeostasis), but it is clinically important as a tumor marker for medullary thyroid carcinoma.
- Sabiston Textbook of Surgery, p. 1490
14. Parathyroid Glands (Closely Related Structures)
Two pairs of parathyroid glands lie on the posterior surface of each thyroid lobe:
- Superior parathyroids (from 4th pharyngeal pouch)
- Inferior parathyroids (from 3rd pharyngeal pouch - travel farther, more variable position)
Their blood supply comes primarily from the inferior thyroid artery. Their position is variable (anywhere from carotid bifurcation to mediastinum) - a critical consideration during thyroidectomy.
Sources
- Guyton and Hall Textbook of Medical Physiology (p. 930-938)
- Gray's Anatomy for Students (p. 1157-1160)
- Sabiston Textbook of Surgery (p. 1488-1491)
- Junqueira's Basic Histology (p. 1034-1035)
- Schwartz's Principles of Surgery, 11th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.