Heart failure mbbs neet pg full explanation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full NEET PG / MBBS explanation.
❤️ Heart Failure - Complete NEET PG / MBBS Explanation
Sources: Goldman-Cecil Medicine, Robbins & Kumar Basic Pathology, Braunwald's Heart Disease, Lippincott Pharmacology, Goodman & Gilman's
1. DEFINITION
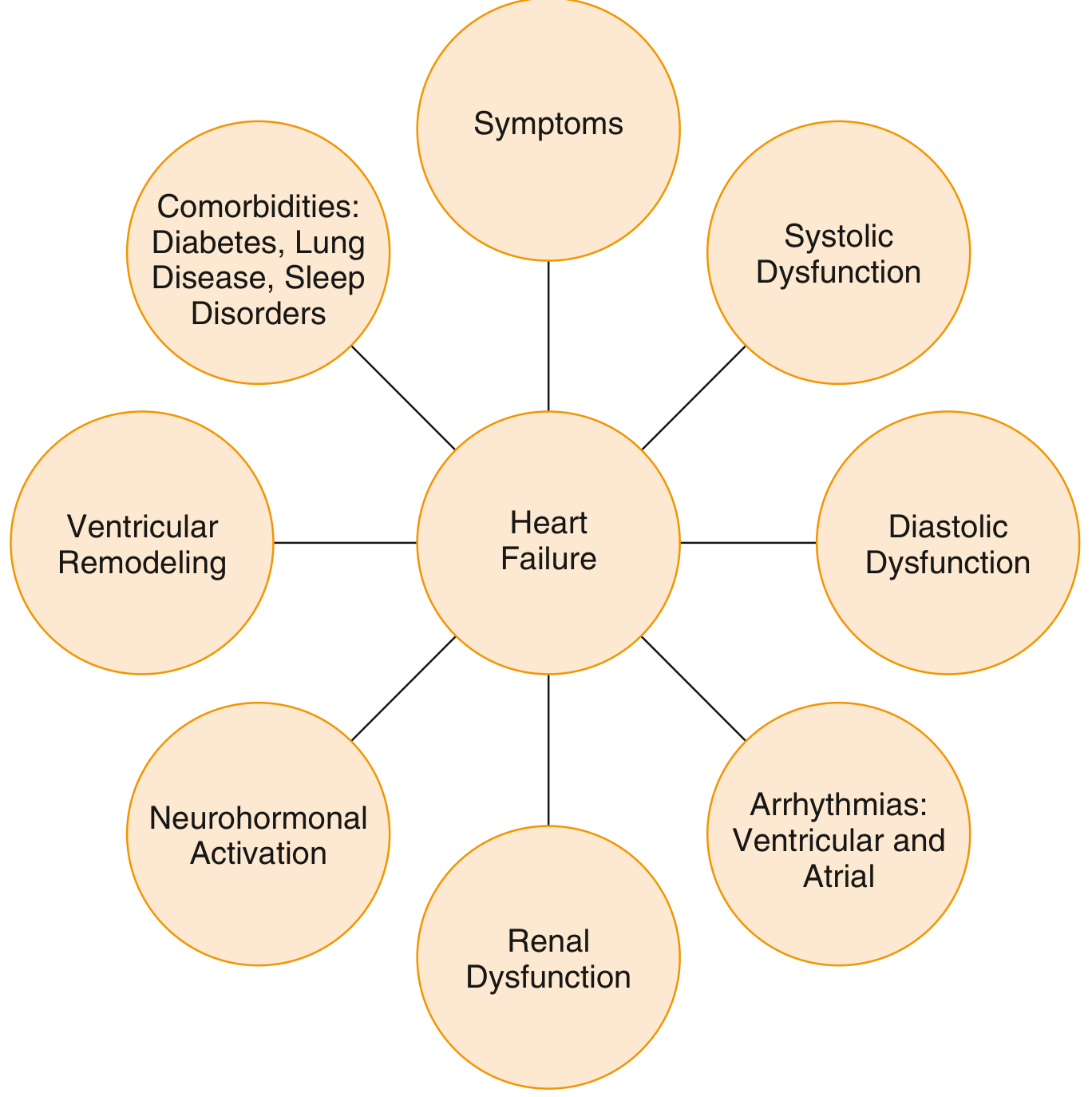
Heart failure (HF) is a clinical syndrome in which the heart is unable to pump sufficient blood to meet the body's metabolic demands, or can do so only at the cost of elevated filling pressures. It is NOT a single disease but the end result of many cardiac conditions.
- Systolic HF (HFrEF): Reduced ejection fraction (EF <40%) - impaired contractility
- Diastolic HF (HFpEF): Preserved EF (>50%) - impaired relaxation/filling
- HFmrEF: Mid-range EF (40-50%)
Nearly half of all HF patients have preserved EF. Mortality is similar in both HFrEF and HFpEF (~50% within 5 years of diagnosis). - Goldman-Cecil Medicine
2. ETIOLOGY / CAUSES
| Category | Examples |
|---|---|
| Most common (70%) | Coronary artery disease / prior MI |
| Hypertension | Pressure overload causing LVH |
| Valvular disease | Aortic stenosis, mitral regurgitation |
| Cardiomyopathy | Dilated, hypertrophic, restrictive |
| Metabolic | Diabetes, obesity, metabolic syndrome |
| Toxins | Alcohol, chemotherapy (anthracyclines) |
| Infections | Myocarditis (Coxsackie B), Chagas disease |
| Infiltrative | Amyloidosis, sarcoidosis, hemochromatosis |
| Volume overload | AV fistulae, severe anemia, thyrotoxicosis |
Mnemonic for causes: HIDE CAT - Hypertension, IHD, Dilated cardiomyopathy, Endocarditis/valvular, Cardiomyopathy (restrictive), Arrhythmias, Thyrotoxicosis
3. PATHOPHYSIOLOGY
Sequence of Events
Myocardial injury → ↓ Cardiac Output → Compensatory mechanisms → Decompensation
Compensatory Mechanisms (Initially Helpful, Eventually Harmful)
A. Frank-Starling Mechanism
- ↓ CO → ↑ venous return → ↑ preload → ↑ sarcomere stretch → ↑ contractility
- Helps short term; long term causes ventricular dilation
B. Neurohormonal Activation (KEY for NEET PG)
| System | Effect | Long-term consequence |
|---|---|---|
| Sympathetic NS | ↑ HR, ↑ contractility, vasoconstriction | Norepinephrine toxic to myocytes; ↓ β-receptor density |
| RAAS | ↑ Angiotensin II → vasoconstriction; Aldosterone → Na+/H2O retention | Maladaptive remodeling, fibrosis |
| ADH/Vasopressin | V1: vasoconstriction; V2: free water retention | Hyponatremia, volume overload |
| Endothelin | Prolonged vasoconstriction, ↓ GFR, pulmonary arteriolar constriction | Worsening HF |
| BNP/ANP (counterregulatory) | Vasodilation, natriuresis, diuresis | Marker of severity; elevated BNP = poor prognosis |
"The sympathetic nervous system and RAAS are co-regulated, such that increased activity of each pathway stimulates a simultaneous increase in the other." - Goldman-Cecil Medicine
C. Ventricular Remodeling
- Pathological hypertrophy + chamber dilation
- Eccentric hypertrophy (volume overload - sarcomeres in series)
- Concentric hypertrophy (pressure overload - sarcomeres in parallel)
- Progressive → further LV dysfunction → spiral of worsening
D. Calcium Cycling Abnormality
- Abnormal ryanodine receptors → diastolic Ca²⁺ leak from sarcoplasmic reticulum
- Loss of SERCA2a function → impaired Ca²⁺ reuptake → diastolic dysfunction
- Reduced Ca²⁺ stores → impaired systolic contraction
E. Cardiorenal Interaction
- ↓ cardiac output → ↓ renal perfusion + passive venous congestion → ↓ GFR
- Worsening renal function → further Na+ and water retention → vicious cycle
4. CLASSIFICATION
A. ACC/AHA Staging (Progression-Based - NEET HIGH YIELD)
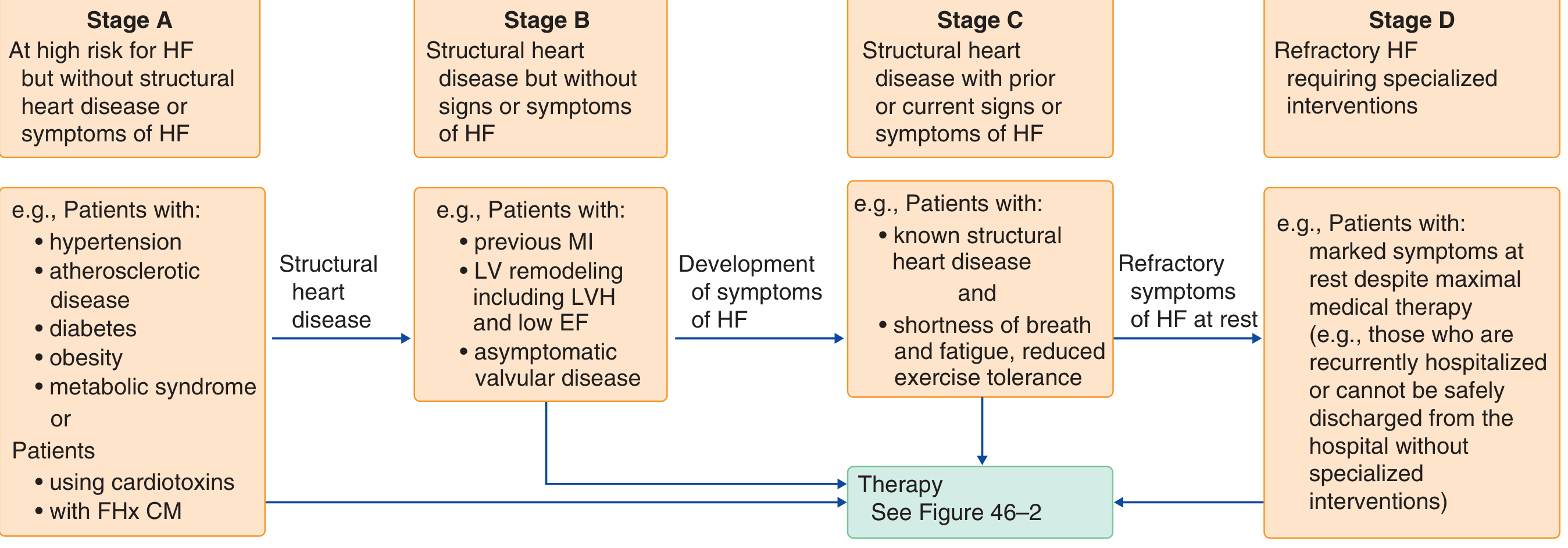
| Stage | Description | Example |
|---|---|---|
| A | At risk, NO structural disease | HTN, DM, obesity, family history |
| B | Structural disease, NO symptoms | Previous MI, LVH, asymptomatic LV dysfunction |
| C | Structural disease WITH current or prior symptoms | Breathlessness, fatigue, reduced exercise tolerance |
| D | Refractory HF requiring specialized interventions | Recurrently hospitalized, symptoms at rest |
KEY: Stage A and B = prevent progression. Stage C and D = treat symptoms and improve survival.
B. NYHA Functional Classification (Symptom-Based - HIGH YIELD)
| Class | Description |
|---|---|
| I | No symptoms with ordinary activity |
| II | Slight limitation; symptoms with moderate exertion |
| III | Marked limitation; symptoms with minimal exertion |
| IV | Symptoms at rest; unable to carry out any activity |
Remember: ACC/AHA stages are unidirectional (can't go back from C to B). NYHA classes are dynamic (can improve with treatment).
C. By Ejection Fraction
| Type | EF | Key Feature |
|---|---|---|
| HFrEF | <40% | Systolic dysfunction; responds to most drugs |
| HFmrEF | 40-50% | Intermediate; heterogeneous |
| HFpEF | >50% | Diastolic dysfunction; older, female, HTN |
5. MORPHOLOGY / PATHOLOGY (Robbins - HIGH YIELD)
Left-Sided Heart Failure
Heart:
- LV usually hypertrophied and dilated
- LV dilation → functional mitral regurgitation → left atrial enlargement → atrial fibrillation
- Microscopy: myocyte hypertrophy + interstitial fibrosis
Lungs (MOST IMPORTANT):
- Acute: pulmonary edema - heavy, wet lungs; perivascular/interstitial transudates
- Chronic: "Heart failure cells" = hemosiderin-laden alveolar macrophages (RBCs extravasate → phagocytosed → hemosiderin deposition)
- Pleural effusion (from increased hydrostatic pressure in visceral pleural venules)
Right-Sided Heart Failure
Liver:
- Congestive hepatomegaly
- "Nutmeg liver" - congested centrilobular areas + paler peripheral parenchyma on cut section
- Severe chronic: Cardiac cirrhosis (centrilobular fibrosis)
Spleen: Congestive splenomegaly
Other: Peripheral pitting edema (dependent), ascites, pleural effusion, pericardial effusion
6. CLINICAL FEATURES
Left Heart Failure (Pulmonary Congestion + Low Output)
| Symptom | Mechanism |
|---|---|
| Dyspnea on exertion (earliest) | ↑ pulmonary venous pressure → pulmonary edema |
| Orthopnea | Recumbent position → ↑ venous return → ↑ pulmonary congestion; relieved by sitting up |
| PND (paroxysmal nocturnal dyspnea) | Awakens from sleep; dramatic breathlessness/suffocation |
| Cardiac asthma | Wheeze from bronchospasm due to edema |
| Pink frothy sputum | Acute pulmonary edema |
| Fatigue/exercise intolerance | Low cardiac output |
| Nocturia | Fluid redistribution when recumbent at night |
| Cheyne-Stokes respiration | Reduced cerebral perfusion |
Signs:
- Elevated JVP (when biventricular)
- 3rd heart sound (S3) - gallop = PATHOGNOMONIC of HF (ventricular overload)
- 4th heart sound (S4) - non-compliant, stiff ventricle
- Displaced/laterally displaced apex
- Bilateral basal crepitations (crackles)
- Pulsus alternans (alternating strong/weak pulse in severe LV failure)
Right Heart Failure (Systemic Congestion)
- Raised JVP (jugular venous pressure) - most important sign
- Hepatomegaly (tender, pulsatile)
- Peripheral pitting edema (ankle → thigh → sacral in bedridden)
- Ascites
- Pleural effusion (more right-sided)
- Kussmaul's sign (JVP rises on inspiration) in constrictive pericarditis/RV infarct
7. INVESTIGATIONS
Biomarkers (HIGH YIELD)
- BNP (B-type Natriuretic Peptide) and NT-proBNP: Released from ventricular myocytes in response to wall stretch
- BNP >100 pg/mL = HF likely
- BNP <35 pg/mL = HF unlikely
- Used for diagnosis AND prognosis; ↑ BNP = worse outcome
- Elevated in ALL types of HF
Imaging
- CXR: Cardiomegaly, pulmonary venous congestion, Kerley B lines, bat-wing perihilar edema, pleural effusion
- Echo (2D Echo + Doppler): Gold standard - assesses EF, wall motion, valves, filling pressures
- EF <40% = HFrEF
- Tissue Doppler for diastolic function
ECG
- May show LVH, Q waves (prior MI), LBBB, AF (common comorbidity)
- LBBB with EF <35% = candidate for CRT (cardiac resynchronization therapy)
Others
- Serum electrolytes, creatinine (renal function monitoring)
- Thyroid function (rule out thyrotoxicosis)
- CBC (anemia can worsen HF)
- Coronary angiography (if ischemic etiology suspected)
8. TREATMENT
Non-Pharmacological
- Salt restriction (<2g/day sodium)
- Fluid restriction in advanced HF
- Daily weight monitoring (if weight ↑ >1.5-2 kg over 2 days → adjust diuretic)
- Regular aerobic exercise (once stable)
- Vaccination (influenza, pneumococcal)
- Avoid NSAIDs, verapamil/diltiazem (negative inotropes)
Pharmacological Treatment of HFrEF (EF <40%) - NEET MEGA HIGH YIELD
The "Fantastic Four" / GDMT (Guideline-Directed Medical Therapy):
| Drug Class | Examples | Mechanism | Benefit |
|---|---|---|---|
| ARNI (first-line over ACEi) | Sacubitril/valsartan (Entresto) | Neprilysin inhibitor + ARB → ↑ BNP → vasodilation, natriuresis | Reduces mortality >ACEi |
| ACE Inhibitor | Ramipril, Enalapril, Lisinopril | Blocks angiotensin II, ↓ aldosterone | Reduces mortality, prevents remodeling |
| ARB | Valsartan, Candesartan | If ACEi intolerant (cough) | Similar to ACEi |
| β-Blocker | Carvedilol, Bisoprolol, Metoprolol succinate | Blocks SNS activation | Reduces mortality, ↑ EF |
| MRA (Aldosterone antagonist) | Spironolactone, Eplerenone | Block aldosterone → ↓ Na+ retention, ↓ fibrosis | Reduces mortality; watch K+ |
| SGLT2 inhibitor | Dapagliflozin, Empagliflozin | Glucosuria → ↓ preload, cardioprotective | Newest pillar; reduces HF hospitalizations |
Diuretics (symptom relief - do NOT improve mortality):
- Loop diuretics: Furosemide - first-line for volume overload
- Thiazides: Added in resistant cases
- Combination (loop + thiazide) in stage D
Other drugs:
- Ivabradine: If HR >70 bpm in sinus rhythm despite max β-blocker; inhibits If (funny current) in SA node
- Digoxin: Rate control in AF with HF; modest symptom benefit (no mortality benefit); narrow therapeutic index - watch toxicity
- Hydralazine + Isosorbide dinitrate: For patients who cannot tolerate ACEi/ARB/ARNI (especially in renal failure or African Americans)
Device Therapy
- ICD (Implantable Cardioverter Defibrillator): EF ≤35%, NYHA II-III, on optimal medical therapy - prevents sudden cardiac death
- CRT (Cardiac Resynchronization Therapy/Biventricular pacemaker): EF ≤35% + LBBB + QRS ≥150ms - resynchronizes LV contraction
- CRT-D: Combined CRT + ICD
Advanced/Stage D HF
- LVAD (Left Ventricular Assist Device): Bridge to transplant or destination therapy
- Heart Transplantation: Gold standard for eligible patients
HFpEF Treatment
- Currently no therapy proven to reduce mortality in HFpEF
- Treat underlying cause (HTN, AF, obesity)
- Diuretics for symptom relief
- SGLT2 inhibitors (empagliflozin, dapagliflozin) - now shown to reduce HF hospitalization even in HFpEF
9. ACUTE DECOMPENSATED HEART FAILURE (ADHF)
Precipitants (Mnemonic: FAILURE)
- Forgetting medications
- Arrhythmia / Anemia
- Ischemia / Infection
- Life style (dietary indiscretion, excess salt/fluid)
- Up in heart rate (uncontrolled AF)
- Renal failure
- Embolism (pulmonary)
Acute Management:
- Position: Sit upright
- Oxygen + BiPAP/CPAP for pulmonary edema
- IV Furosemide (40-80 mg) - rapid diuresis
- IV Nitrates (nitroglycerine/isosorbide dinitrate) - vasodilation, ↓ preload
- Morphine (controversial - causes vasodilation, reduces anxiety; now less preferred)
- Inotropes if cardiogenic shock: Dobutamine (positive inotrope), Dopamine
- Vasopressors if refractory shock: Norepinephrine
10. PROGNOSIS - KEY FACTS
- ~50% mortality within 5 years of diagnosis
- Annual sudden cardiac death risk 5-10x higher than general population
- Poor prognostic markers: ↑ BNP, low Na+, low EF, NYHA class IV, renal dysfunction, QRS widening
11. HIGH-YIELD ONE-LINERS FOR NEET PG MCQs
| Question type | Answer |
|---|---|
| Most common cause of HF | Ischemic heart disease (CAD/MI) |
| Most common cause of RHF | Left heart failure |
| Cor pulmonale = | RHF due to lung disease |
| Earliest symptom of LHF | Dyspnea on exertion |
| Gold standard investigation | 2D Echocardiography |
| Best single biomarker | BNP / NT-proBNP |
| "Heart failure cells" | Hemosiderin-laden alveolar macrophages |
| "Nutmeg liver" seen in | Right heart failure (chronic congestive hepatomegaly) |
| S3 gallop heard in | Volume-overloaded/dilated ventricle (significant) |
| S4 gallop heard in | Stiff/non-compliant ventricle (HTN, HCM) |
| Drug that reduces mortality in HFrEF | ACEi, ARBs, β-blockers, ARNI, MRA, SGLT2i |
| Drug with NO mortality benefit | Diuretics, Digoxin |
| Drug contraindicated in HF | Verapamil, diltiazem, NSAIDs, thiazolidinediones |
| ARNI preferred over | ACE inhibitor (for HFrEF NYHA II-III) |
| β-blockers approved for HF | Carvedilol, Bisoprolol, Metoprolol succinate ONLY |
| ICD indication in HF | EF ≤35%, NYHA II-III, on GDMT |
| CRT indication | EF ≤35% + LBBB + QRS ≥150ms |
| Ivabradine used when | Sinus rhythm, HR >70, intolerant/max β-blocker dose |
| Spironolactone side effect to monitor | Hyperkalemia (stop if K+ >6 mmol/L) |
| Spironolactone male side effect | Gynecomastia (less with eplerenone) |
Sources cited:
- Goldman-Cecil Medicine, 26e - Chapter 45 (Heart Failure Epidemiology, Classification) and Chapter 46 (Management)
- Robbins & Kumar Basic Pathology - Chapter 9 (Cardiac morphology and clinical features)
- Braunwald's Heart Disease, 12e - Heart Failure Definition and Epidemiology
- Lippincott Illustrated Reviews: Pharmacology - HF pharmacotherapy
- Goodman & Gilman's Pharmacological Basis of Therapeutics - HF staging and drug mechanisms
This is a shared conversation. Sign in to Orris to start your own chat.