Phases of cardiac cycle
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
I now have a thorough, multi-textbook picture of the cardiac cycle. Let me compose the complete answer.
Phases of the Cardiac Cycle
The cardiac cycle encompasses all mechanical and electrical events from the beginning of one heartbeat to the beginning of the next. At a heart rate of 72 beats/min the cycle lasts ~0.833 s; at 75 beats/min it lasts ~0.800 s. Each cycle is triggered by an action potential from the sinoatrial node, which spreads through both atria, traverses the AV node (adding >0.1 s delay), and then activates the ventricles. Systole occupies ~300 ms and diastole ~500 ms at rest.
The Four Fundamental Phases (valve-based view)
From the perspective of ventricular valve positions, there are 4 core phases (Medical Physiology, p. 745):
| Phase | AV Valve | Semilunar Valve | Volume |
|---|---|---|---|
| 1. Inflow (ventricular filling) | Open | Closed | Increasing |
| 2. Isovolumetric contraction | Closed | Closed | Constant |
| 3. Outflow (ventricular ejection) | Closed | Open | Decreasing |
| 4. Isovolumetric relaxation | Closed | Closed | Constant |
Systole = phases 2 + 3; Diastole = phases 4 + 1.
Expanded Seven-Phase Description
Costanzo Physiology describes 7 phases (A-G) that give finer temporal resolution:
Phase A - Atrial Systole
- ECG: P wave -> PR interval
- The atria depolarize and contract, raising left atrial pressure. This is reflected in the venous pulse as the a wave.
- The mitral valve is already open; atrial contraction adds the final ~20-30% of ventricular filling ("atrial kick"), raising LV end-diastolic volume.
- Heart sound: S4 (not audible in healthy adults; heard in ventricular hypertrophy with reduced compliance).
Phase B - Isovolumetric Ventricular Contraction
- ECG: QRS complex
- Ventricles depolarize and begin contracting. LV pressure rises sharply.
- When LV pressure exceeds left atrial pressure, the mitral valve closes - producing S1 (mitral closes slightly before tricuspid, hence possible splitting of S1).
- Both AV and semilunar valves are now closed: volume is constant (isovolumetric), but pressure climbs steeply.
- This is an energy-consuming phase with no ejection.
Phase C - Rapid Ventricular Ejection
- ECG: ST segment
- When LV pressure exceeds aortic diastolic pressure (~80 mmHg), the aortic valve opens.
- Blood is rapidly ejected into the aorta - most of the stroke volume (~70%) is ejected here.
- LV pressure rises to its peak (~120 mmHg). Aortic pressure rises simultaneously.
- LV volume falls sharply.
- Atrial filling begins quietly in the background as venous return continues.
Phase D - Reduced Ventricular Ejection
- ECG: T wave begins (ventricular repolarization starts)
- Ventricles begin relaxing; pressure falls.
- The aortic valve is still open, so ejection continues but at a slower rate.
- Blood "runs off" into the peripheral arterial tree faster than the ventricle ejects it, so aortic pressure begins to fall.
- LV volume reaches its minimum (end-systolic volume, ~50 mL).
Phase E - Isovolumetric Ventricular Relaxation
- ECG: End of T wave
- Ventricles are fully relaxed; LV pressure falls precipitously.
- When LV pressure drops below aortic pressure, the aortic valve closes - producing S2 (aortic component A2 closes just before pulmonic P2).
- The dicrotic notch (incisura) appears on the aortic pressure waveform at valve closure.
- All valves again closed: volume constant, pressure falling.
- Inspiratory splitting of S2 occurs because decreased intrathoracic pressure increases RV venous return, prolonging RV ejection and delaying P2.
Phase F - Rapid Ventricular Filling
- ECG: Isoelectric (between T and next P wave)
- When LV pressure falls below left atrial pressure, the mitral valve opens.
- Blood rushes passively from atrium to ventricle down a pressure gradient; LV volume increases rapidly.
- LV pressure stays low due to ventricular compliance.
- Rapid filling produces S3 (normal in children; indicates volume overload/heart failure in adults >40 years).
Phase G - Reduced Ventricular Filling (Diastasis)
- The longest phase of the cardiac cycle.
- Ventricular filling slows as the pressure gradient equalizes.
- Atrial and ventricular pressures equilibrate at low levels.
- At the end of diastasis, ventricular volume = end-diastolic volume (~120-130 mL).
- Clinically important: Tachycardia disproportionately shortens diastasis, reducing filling and stroke volume (Frank-Starling mechanism).
Key Pressure Values (Left Heart, at Rest)
| Parameter | Value |
|---|---|
| LV peak systolic pressure | ~120 mmHg |
| LV end-diastolic pressure | ~8-12 mmHg |
| Aortic systolic / diastolic | ~120 / 80 mmHg |
| Left atrial mean pressure | ~5-10 mmHg |
| End-diastolic volume (EDV) | ~120-130 mL |
| End-systolic volume (ESV) | ~50 mL |
| Stroke volume (SV = EDV - ESV) | ~70-80 mL |
| Ejection fraction (EF) | ~55-70% |
Heart Sounds Summary
| Sound | Cause | Phase |
|---|---|---|
| S1 ("lub") | Closure of mitral (+ tricuspid) valve | End of Phase B (start of systole) |
| S2 ("dub") | Closure of aortic (+ pulmonic) valve | End of Phase E (start of diastole) |
| S3 | Rapid ventricular filling (turbulence) | Phase F |
| S4 | Atrial contraction against stiff ventricle | Phase A |
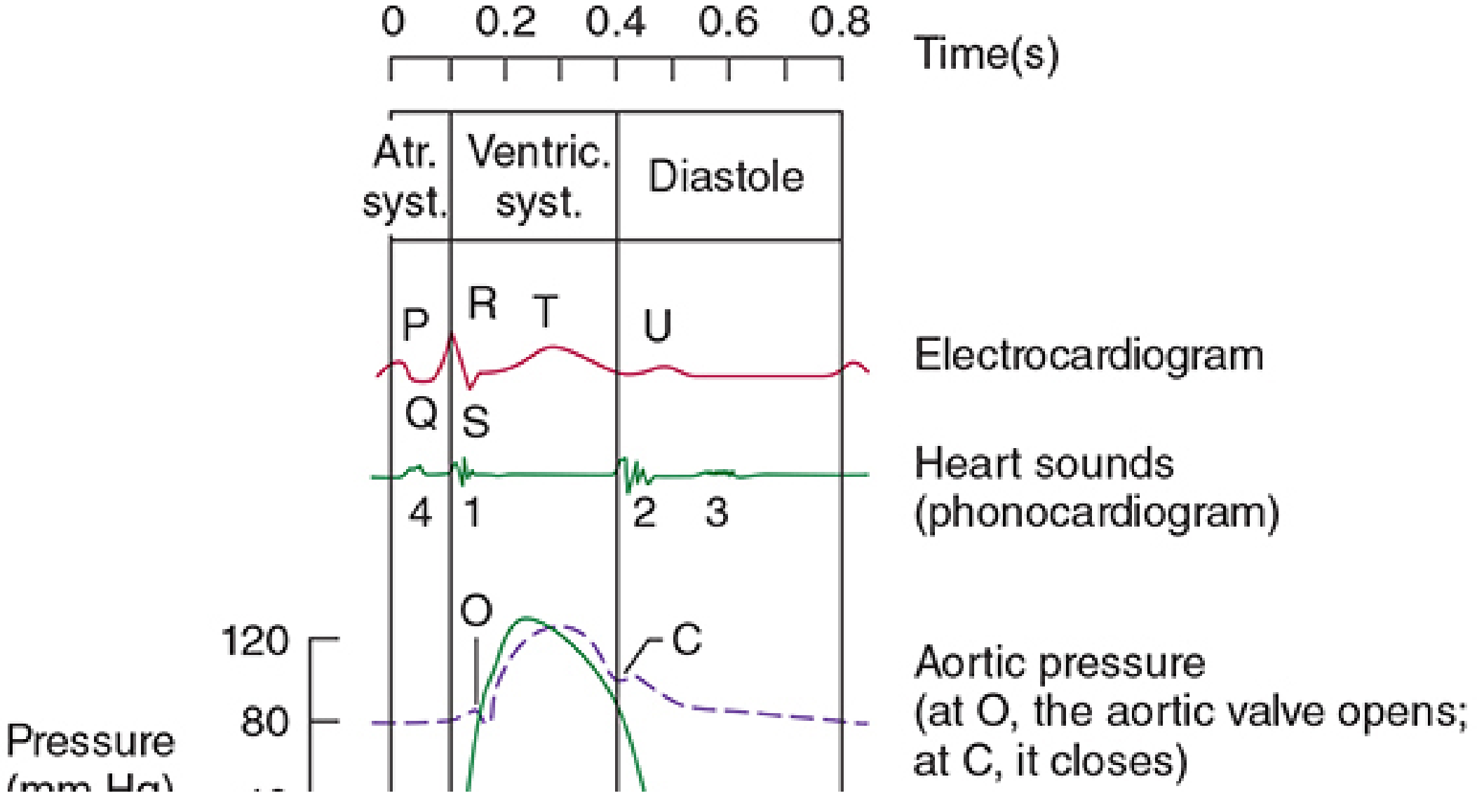
ECG Correlation
| ECG Event | Cardiac Event |
|---|---|
| P wave | Atrial depolarization -> atrial systole |
| PR interval | AV node conduction delay |
| QRS complex | Ventricular depolarization -> isovolumetric contraction begins |
| ST segment | Ventricular plateau (plateau of action potential) -> rapid ejection |
| T wave | Ventricular repolarization -> reduced ejection -> isovolumetric relaxation |
Effect of Heart Rate
At higher heart rates, cycle duration shortens. Diastole is disproportionately reduced compared to systole. At 72 beats/min, systole is ~40% of the cycle; at ~220 beats/min, systole can be ~65% of the cycle. This is why very fast heart rates can impair ventricular filling and reduce cardiac output.
Sources: Costanzo Physiology 7th Ed., pp. 160-163 | Guyton & Hall Medical Physiology | Medical Physiology (Boron & Boulpaep), pp. 745-746 | Ganong's Review of Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.