prevention and control measures of trichomoniasis
"trichomoniasis" AND "prevention" AND "control"
trichomoniasis prevention control measures CDC 2025 guidelines
https://www.cdc.gov/trichomoniasis/about/index.html
Prevention and Control of Trichomoniasis
Overview
1. Primary Prevention (Avoiding Infection)
A. Sexual Behavior Modification
- Abstinence from vaginal, anal, and oral sex is the only guaranteed way to prevent all STIs, including trichomoniasis.
- Reduce the number of sexual partners - having multiple partners significantly increases acquisition risk. - Textbook of Family Medicine 9e, p. 621
- Mutual monogamy - being in a mutually monogamous relationship with an uninfected partner eliminates sexual transmission risk.
B. Consistent Condom Use
- Correct and consistent use of male or female (internal) condoms is the single most important preventive measure for sexually active individuals.
- Condoms reduce the risk of acquiring trichomoniasis by creating a physical barrier to parasite transmission. - Goldman-Cecil Medicine, p. 3453; CDC STI Treatment Guidelines 2021
- Male circumcision may offer some (though not definitive) risk reduction for female partners of circumcised men.
C. Avoid Douching
- Douching is not recommended as it disrupts normal vaginal flora, reduces vaginal acidity (pH), and may increase susceptibility to trichomoniasis and other vaginal infections. - CDC STI Treatment Guidelines, 2021
D. Personal Hygiene and Avoiding Fomite Transmission
- Although trichomoniasis is transmitted almost exclusively by sexual contact, the parasite can survive briefly in moist environments.
- Avoid sharing towels, bathing suits, washcloths, and toilet articles - particularly relevant in communal settings. - Medical Microbiology 9e, p. (section: Treatment, Prevention, and Control)
- Practice good personal hygiene.
E. Open Communication with Partners
- Discuss STI status and testing history with new sexual partners before sex.
- Normalizing frank, honest communication reduces unknowing transmission.
2. Screening (Secondary Prevention)
| Population | Recommendation |
|---|---|
| High-risk women (sex workers, multiple partners) | Routine screening |
| Women evaluated for any STI | Include T. vaginalis testing |
| HIV-positive women | Screen at least annually (trichomoniasis increases risk of pelvic inflammatory disease and HIV transmission) |
| Pregnant women | Test symptomatic women; benefit of routine asymptomatic screening not established |
| Men | Wet prep has poor sensitivity; culture of urethral/urine/semen or NAAT preferred |
- Goldman-Cecil Medicine, p. 3452; Textbook of Family Medicine 9e, p. 621
Diagnostic Methods
- Wet mount microscopy - motile trichomonads; sensitivity ~60% in women, ~50% in men; first-line due to cost and speed.
- NAATs (nucleic acid amplification tests) - most sensitive; preferred for men and when wet prep is inconclusive.
- Rapid point-of-care tests (OSOM Trichomonas Rapid Test, AFFIRM VP III) - FDA-approved; higher sensitivity than wet mount but more false positives.
- Culture - gold standard for sensitivity but results take 3-7 days.
- Pap smear is not recommended as a diagnostic tool (sensitivity only 58%).
3. Treatment as Prevention (Tertiary Control)
First-Line Regimens (CDC 2021)
| Drug | Dose | Notes |
|---|---|---|
| Metronidazole | 500 mg orally twice daily for 7 days (preferred) OR 2 g single dose | 7-day course preferred over single dose for better cure rates |
| Tinidazole | 2 g single oral dose | Better tolerated, more effective as single-dose; drug of choice per Goldman-Cecil |
- Both drugs have a disulfiram-like reaction with alcohol - patients must avoid alcohol for 24 hours after metronidazole and 72 hours after tinidazole. - Goldman-Cecil Medicine, p. 3452
- Metronidazole gel (intravaginal) is less effective (≤50% cure rate) and is not recommended as sole therapy. - Textbook of Family Medicine 9e, p. 622
Special Populations
- Symptomatic pregnant women at any stage should be treated. Treatment relieves symptoms and prevents neonatal respiratory or genital infection.
- Metronidazole is safe in pregnancy (no teratogenicity reported); tinidazole is not recommended in pregnancy.
- Clotrimazole 100 mg intravaginally nightly for 2 weeks may relieve symptoms but does not eradicate the infection.
- Andrews' Diseases of the Skin, p. 493; Goldman-Cecil Medicine, p. 3452
- Treat with metronidazole 500 mg twice daily for 7 days (not single-dose) due to higher recrudescence rates with single-dose therapy. - Goldman-Cecil Medicine, p. 3453
- Acquired during passage through an infected birth canal; treat only if symptomatic or if colonization persists more than 4 weeks. - Andrews' Diseases of the Skin, p. 492
4. Partner Management (Critical for Control)
- Concurrent (simultaneous) treatment of all current sex partners is mandatory - nearly 20% of male partners are coinfected, and most are asymptomatic. - Goldman-Cecil Medicine, p. 3453
- Partners should abstain from sex until both have completed treatment and symptoms have resolved.
- Expedited Partner Therapy (EPT) - prescribing treatment for partners without a prior clinical evaluation - is legally permissible in many jurisdictions and can be used to reduce barriers to partner treatment. - CDC STI Guidelines 2021
- A test of cure is not necessary if symptoms resolve after treatment. However, the CDC recommends re-testing 3 months after treatment due to high reinfection rates (~1 in 5 people within 3 months). - CDC
5. Recurrent / Resistant Trichomoniasis
- Repeat course: Tinidazole or metronidazole 2 g once daily for 5-7 days.
- High-dose regimen: Oral tinidazole 2 g/day plus intravaginal tinidazole 500 mg twice daily for 14 days.
- Salvage regimen: Oral tinidazole 1 g three times/day plus intravaginal paromomycin cream (4 g of 6.25%) nightly for 14 days.
- Drug-resistance testing: CDC provides a kit for cases refractory to treatment. - CDC Resistance Testing
- Intravaginal boric acid (600 mg twice daily for 1 month) has documented clinical improvement in some refractory cases. - Goldman-Cecil Medicine, p. 3453
6. Public Health and Surveillance Measures
- STI surveillance and reporting to track trichomoniasis trends, particularly in high-burden communities.
- Addressing health disparities - trichomoniasis rates are 7 times higher in Black women than non-Hispanic White women in the US, calling for targeted outreach and accessible testing. - Goldman-Cecil Medicine, p. 3452
- Screening programs in STI clinics, family planning centers, HIV care settings.
- Health education in schools and communities about safe sex practices, STI awareness, and partner communication.
- No vaccine is currently available for human trichomoniasis; vaccine research is ongoing.
Summary Table
| Category | Key Measures |
|---|---|
| Primary prevention | Abstinence, condom use, reduce partners, avoid douching, personal hygiene |
| Screening | High-risk women, HIV+ women (annually), all STI evaluations |
| Treatment | Metronidazole 500mg BID x7d or tinidazole 2g single dose |
| Partner management | Concurrent treatment, abstinence until cured, EPT where legal |
| Re-testing | 3 months post-treatment |
| Resistance | Escalating regimens; CDC drug-resistance testing available |
| Public health | Surveillance, education, health equity interventions |
Note (PubMed 2025): A recent systematic review and meta-analysis (PMID 40864904) on global prevalence and risk factors for T. vaginalis (published 2025) confirms that multiple sexual partners and lower socioeconomic status remain dominant modifiable risk factors - reinforcing the behavioral prevention strategies outlined above.
explain about EWARS
EWARS Early Warning Alert and Response System WHO explained components
https://www.paho.org/en/health-emergencies/health-emergency-…
EWARS "in a box" components diseases monitored alert thresholds WHO implementation
EWARS - Early Warning, Alert and Response System
1. Definition and Background
The overall aim of EWARS is to reduce excess morbidity and mortality due to epidemic-prone diseases and other public health hazards in emergency-affected populations.
2. What is EWAR vs EWARS vs EWARN?
| Term | Full Form | Meaning |
|---|---|---|
| EWAR | Early Warning, Alert and Response | The general concept/process of detecting and responding to health signals |
| EWARS | Early Warning, Alert and Response System | WHO's specific software and technology platform that operationalizes EWAR |
| EWARN | Early Warning, Alert and Response Network | A network of health partners that collectively implements EWAR in a region (used in WHO EMRO countries like Syria, Iraq, Afghanistan) |
3. Core Objective
"To support the early detection and rapid response to acute public health events of any origin." - PAHO/WHO
- Detect outbreaks before they spread and claim lives
- Provide a simple, cost-effective surveillance infrastructure where none exists
- Work in settings with no reliable internet or electricity
- Connect field health workers to decision-makers in real time
- Generate automated epidemiological reports to inform response
4. Three Core Components of EWAR
A. Early Warning (Signal Detection)
- The rapid detection of signals that may indicate a potential acute public health event.
- Uses two complementary surveillance approaches:
| Type | Description |
|---|---|
| IBS (Indicator-Based Surveillance) | Structured, routine reporting from health facilities using standardized case definitions and counts (e.g., weekly disease tallies) |
| EBS (Event-Based Surveillance) | Unstructured reports from any source - community members, rumors, media, health workers - that something unusual is happening. Can be implemented faster than IBS at emergency onset |
- Alert thresholds are pre-set for each disease. When a threshold is crossed, the system automatically flags the event for urgent investigation.
B. Alert (Verification and Triage)
- Upon receiving a signal, the system activates an immediate investigation to verify whether the event represents a true outbreak threat.
- Verification typically occurs within 24 hours of alert generation.
- Alerts are triaged as: Discarded (false alarm), Monitored (watch and see), or Requires Response (confirmed outbreak).
C. Response (Action)
- Once an alert is verified as a real event, EWARS supports rapid public health response including:
- Outbreak investigation (case-based line listing with GPS coordinates)
- Generic immediate control measures
- Agent-specific control measures (e.g., vaccination, case isolation, water chlorination)
- Real-time epidemic curves, maps, and dashboards
- Automated daily outbreak bulletins shared with partners
5. EWARS Technology Platform
i. EWARS Mobile (Data Collection)
- A mobile app installed on smartphones distributed to health workers at reporting sites (clinics, health posts)
- Workers submit weekly aggregate reports and immediate case alerts using pre-configured digital forms
- Works offline - data queues and submits when network is available
- Provides SMS feedback to facilities: report receipt confirmations, overdue reminders, and instant alert notifications
ii. EWARS DataHub (Server/Analysis)
- A local server that receives, stores, and processes all incoming data
- Generates automated epidemiological bulletins, epidemic curves, and maps
- Works fully offline - no internet required
- Allows customized analysis, line-list export, and anonymization of data for partner sharing
- Hosts alert threshold logic and sends alert notifications
iii. EWARS Exchange (Online Dashboard)
- An online platform for when internet connectivity is available
- Allows broader data sharing with national authorities, WHO, and partner organizations
- Supports integration with national surveillance systems
6. EWARS "in a Box"
Contents of the Box:
- 60 mobile phones (for data collection at health facilities)
- Laptops (for data management and analysis)
- A local server (DataHub - works offline)
- Solar generator and solar chargers (for areas without electricity)
- Network equipment and accessories
- Pre-loaded surveillance software
Key Specifications:
| Feature | Detail |
|---|---|
| Cost | ~US$ 15,000 per kit |
| Coverage | 50 fixed or mobile clinics; ~500,000 people |
| Deployment time | Can be configured within 48 hours of emergency declaration |
| Electricity | Not required (solar powered) |
| Internet | Not required (offline-capable) |
| Mobile network | Required (for SMS alerts) |
7. Diseases and Conditions Monitored
| Category | Examples |
|---|---|
| Vaccine-preventable | Measles, yellow fever, acute flaccid paralysis (polio indicator) |
| Diarrheal diseases | Acute watery diarrhea (cholera indicator), bloody diarrhea |
| Vector-borne | Malaria, dengue |
| Respiratory | Acute respiratory infections, meningitis |
| Hemorrhagic fevers | Viral hemorrhagic fever |
| Others | Severe acute malnutrition, neonatal tetanus, relapsing fever |
8. EWARS Alert Threshold System
- The system automatically generates an alert
- Alert is sent via SMS to surveillance officers
- A 24-hour verification is initiated
- If confirmed, a public health response is activated
9. EWARS Implementation Process
EMERGENCY DECLARED
↓
Rapid needs assessment (existing surveillance capacity?)
↓
Configure EWARS (diseases, thresholds, reporting sites, case definitions)
↓
Deploy EWARS in a Box → Train health workers
↓
Weekly aggregate reporting + Immediate case alerts
↓
Automated alert generation → 24h verification
↓
Response activation (investigation, control measures)
↓
Weekly epidemiological bulletins → Feedback to facilities
↓
Post-emergency: Re-integrate into national surveillance system
10. Governance and Partners
- EWARS is led and managed by WHO in coordination with:
- Ministries of Health (national ownership)
- UNHCR (refugee settings)
- UNICEF, MSF, NGOs (health facility network)
- US CDC (technical support and evaluation)
- ECDC (European contexts)
11. EWARS vs Routine Surveillance Systems
| Feature | EWARS | Routine National Surveillance |
|---|---|---|
| Setting | Emergencies, conflicts, disasters | Stable, peacetime settings |
| Deployment | Within 48 hours | Years to develop |
| Electricity needed | No (solar) | Yes |
| Internet needed | No (offline) | Usually yes |
| Case definitions | Syndromic (clinical) | Often lab-confirmed |
| Purpose | Outbreak detection + response | Trend monitoring + policy |
| Data flow | Mobile → DataHub → Exchange | Facility → District → National |
12. Where EWARS Has Been Used
Summary

EXPLAIN IN UNDERSTANDABLE WAY
Understanding the EWARS Diagram - Simply Explained
The Players in This System
| Box Color | Meaning | Who |
|---|---|---|
| 🟩 Green boxes | Directly part of EWARS | EDCD, Sentinel Sites, VBDRTC |
| 🟧 Orange boxes | Support the system (indirectly) | Health Directorate, Health Office (RRT), Local health facilities, Local municipalities |
Meet the Key Players (Simply)
🟩 EDCD - Epidemiology and Disease Control Division
Think of this as the "brain" or headquarters" at the top.
- It is the national authority that receives all disease reports.
- It gives feedback back down to the system.
- It coordinates with everyone for a big-picture response.
🟩 Sentinel Sites
These are selected hospitals or clinics chosen strategically to act as "watchdogs" for disease.
- They are the main reporters - they send data weekly (routine updates) AND immediately (when something urgent happens).
- They report upward to EDCD AND sideways to VBDRTC.
- They also receive feedback from EDCD so they know what is happening nationally.
🟩 VBDRTC - Vector Borne Disease Response and Training Centre
Think of this as a specialist expert center - focused specifically on diseases spread by mosquitoes, flies, etc. (malaria, dengue, etc.)
- It receives weekly and immediate reports from Sentinel Sites.
- It has two-way coordination with EDCD - meaning they talk back and forth to plan responses together.
🟧 Health Office (RRT) - Rapid Response Team
This is the local action team - the people who physically go out to investigate and respond when an alert is raised.
- RRT = Rapid Response Team - they move fast when an outbreak is suspected.
- They coordinate with the Health Directorate above them and the local facilities below them.
- They receive referrals of suspected cases from local facilities.
🟧 Health Directorate
The district/regional administrative body - a middle manager between the Health Office and the Sentinel Sites.
- Has two-way coordination with the Health Office (RRT) for verification and response.
🟧 Local Health Facilities
The ground-level clinics and health posts where patients actually show up.
- These are the first to notice something unusual (a spike in fever cases, diarrhea, rash, etc.)
- They send informal outbreak notifications upward to the Health Office (RRT).
- They refer suspected cases to higher facilities for investigation.
🟧 Local Level (Urban/Rural Municipalities)
The community and local government level - villages, towns.
- Communities can also notice and informally report unusual health events.
- They too send informal outbreak notifications to the Health Office.
How the System Works - Step by Step
STEP 1 - DETECTION (Bottom of diagram)
A local health facility or a village notices unusual cases.
↓
STEP 2 - INFORMAL NOTIFICATION (Dashed arrows going up)
The local facility sends an informal notification to the
Health Office (RRT) saying "something unusual is happening here."
↓
STEP 3 - VERIFICATION (Two-way coordination arrows)
The Health Office (RRT) coordinates back and forth with the
Health Directorate to verify: Is this a real outbreak?
How many cases? Where?
↓
STEP 4 - FORMAL REPORTING (Solid arrows going up)
Sentinel Sites send official weekly reports AND immediate
alerts to EDCD and VBDRTC at the top.
↓
STEP 5 - RESPONSE COORDINATION
EDCD and VBDRTC coordinate with each other (two-way).
They send back feedback and directives downward (dotted arrows).
The RRT is activated and goes to the field.
↓
STEP 6 - REFERRAL OF CASES (Double solid arrows on left)
Suspected serious cases are referred upward from local
facilities to higher-level sentinel sites for proper diagnosis.
Understanding the Arrows
| Arrow Type | Meaning | Example |
|---|---|---|
| → Solid arrow | Formal reporting | Sentinel site reports to EDCD |
| ····→ Dotted arrow | Feedback | EDCD sends feedback back down |
| - - - → (thin dashes) | Informal outbreak notification | Village reports rumor to Health Office |
| ◄══► Bold dashes | Two-way coordination | EDCD and VBDRTC planning response together |
| ⟹ Double solid | Referral of suspected cases | Sending a sick patient to a bigger hospital |
The Big Picture - In One Paragraph
Local clinics and communities at the bottom notice unusual illness and informally alert the local Health Office (Rapid Response Team). The RRT investigates and coordinates with health directorates. Meanwhile, Sentinel Sites - the system's official eyes - formally report data weekly and immediately to two national bodies: EDCD (the overall brain) and VBDRTC (the specialist vector disease center). These top-level bodies coordinate with each other, give feedback down the chain, and activate a response. Suspected cases are physically referred upward through the system for proper testing and management.
Why This Structure Works
- Speed - informal community notifications reach the RRT quickly without waiting for paperwork.
- Two-way flow - information does not just go up; feedback, guidance, and supplies come back down.
- Multiple entry points - outbreaks can be spotted at the local facility level OR the community level OR through sentinel surveillance - reducing the chance of missing something.
- Specialist involvement - VBDRTC ensures that vector-borne disease outbreaks get expert attention immediately.
- Accountability - each arrow represents a defined responsibility, so no one can say "we didn't know."
sailent feature of HMIS
salient features of HMIS health management information system public health
https://nhsrcindia.org/sites/default/files/2021-04/Session%2…
HMIS salient features India NRHM data flow reporting levels components objectives uses
Salient Features of HMIS (Health Management Information System)
What is HMIS?
Think of HMIS as the nervous system of a country's healthcare - it collects signals (data) from every health facility, processes them, and helps the "brain" (health administrators) make informed decisions.
- Source: NHSRC India / WHO
Salient Features of HMIS
1. Comprehensive Data Collection
- HMIS captures data across all levels of the health system - sub-centers, PHCs (Primary Health Centres), CHCs (Community Health Centres), district hospitals, and tertiary institutions.
- In India, HMIS captures 300+ data items under Service Delivery and 400+ data items under Infrastructure and Human Resources on a monthly basis.
- Data categories include:
- Reproductive, Maternal, Neonatal, Child and Adolescent Health (RMNCH+A)
- Immunization, Family Planning
- Vector-borne diseases (malaria, dengue)
- Tuberculosis
- Morbidity and Mortality
- OPD/IPD services, Surgeries
- Infrastructure: buildings, equipment, drugs, staff
- Source: HMIS India 2020
2. Multi-Level Hierarchical Data Flow
Sub-Centre (SC)
↓
Primary Health Centre (PHC) ←→ Block Level
↓
Community Health Centre (CHC)
↓
District Headquarters (DPMU - District Programme Management Unit)
↓
State Headquarters
↓
National Level (Web Portal)
↑
Feedback flows back down at each level
- Each level aggregates data from below and reports upward.
- Facility-level reporting allows identification of underperforming facilities, coverage gaps, and data quality issues - which is not possible with consolidated district-level reporting alone.
- Source: NHSRC India
3. Standardized Reporting Formats
- HMIS uses uniform, pre-defined reporting formats across all facilities and states.
- This ensures data from different geographic areas and administrative levels can be compared, aggregated, and analyzed meaningfully.
- Standardization prevents inconsistency and allows national benchmarking.
- In India, every sub-center and health facility compiles service delivery details as aggregate numbers that are entered into standardized formats.
4. Regular and Timely Reporting (Periodicity)
- Reporting occurs at fixed intervals:
- Monthly - routine service delivery data (OPD, ANC, deliveries, immunization)
- Quarterly - specific indicators (PNC rates, anaemia detection, etc.)
- Annual/Semi-annual - infrastructure, human resources, outcome indicators
- Timeliness is a core principle - delayed data means delayed decisions.
Example: If 5 out of 10 sub-centres fail to submit monthly reports on time, the Medical Officer cannot assess PHC performance or plan effectively.
5. Indicator-Based Monitoring System
| Indicator Type | What it Measures | Example |
|---|---|---|
| Input indicators | Resources available | Number of ANMs posted |
| Process indicators | Activities done | % ANC registered in 1st trimester |
| Output indicators | Services delivered | Institutional delivery rate |
| Outcome indicators | Health results | Maternal Mortality Ratio (MMR) |
| Impact indicators | Long-term change | Reduction in infant mortality |
- Indicators alert managers to problems, but must be compared over time and across facilities to reveal trends - a single isolated number means little.
- Source: NHSRC India
6. Dashboard and Score Card System
- HMIS powers a Health Management Dashboard for real-time visual monitoring of key indicators at national, state, and district levels.
- In India (NRHM/NHM), a Score Card system based on HMIS data rates states/districts:
- Indicators based on a life-cycle approach (newborn → child → adolescent → pregnant woman)
- States scored +1 to +4 (above national average) or -1 to -4 (below average)
- States classified into four performance categories
- This creates accountability and motivates performance improvement. - Park's Textbook of Preventive and Social Medicine
7. Data Quality Assurance
- Validation rules - logical checks prevent impossible entries
e.g., "ANC registrations in 1st trimester cannot exceed total ANC registrations"
- Completeness checks - tracking how many facilities submitted reports out of total facilities
- Timeliness monitoring - checking whether reports were submitted on time
- Random field verification - periodic cross-checks of HMIS data against physical registers at facility level
- Data Quality Review (DQR) Toolkit - WHO-supported tool for comprehensive HMIS data quality audits
- Source: NHSRC India / Global Health Data Methods
8. Web-Based National Portal
- In India, HMIS operates through a centralized national web portal where district-level aggregated data is uploaded monthly.
- This creates a central repository of health information from all public health facilities across the country.
- Accessible to planners, programme managers, and researchers.
- Enables real-time monitoring from any location.
- Data is updated monthly without interruption - a key achievement since the NRHM reform.
9. Programme-Specific Integration
| Programme | Data Captured |
|---|---|
| Reproductive Health | ANC, delivery, PNC rates |
| Child Health | Immunization, nutrition, SNCU admissions |
| Family Planning | Contraceptive use, sterilizations |
| Communicable Diseases | Malaria, TB, dengue cases |
| Non-Communicable Diseases | Hypertension, diabetes screening |
| HIV/PMTCT | ART uptake, PMTCT coverage |
10. Supports Evidence-Based Decision Making at All Levels
| Level | Who Uses It | How They Use It |
|---|---|---|
| Facility | Medical Officer, ANM | Monitor own performance, identify gaps |
| Block/District | DPMU, CMO | Compare facilities, allocate resources, plan |
| State | State Health Department | Policy decisions, budget allocation |
| National | MoHFW, NHM | Programme evaluation, goal setting |
| Research | Academics, WHO | Evidence generation, studies |
11. Feedback Mechanism
- HMIS is not just a one-way upward reporting chain.
- Feedback flows downward from national → state → district → facility.
- Feedback includes: performance analysis, benchmarks, problem areas identified, corrective actions suggested.
- This makes HMIS a two-way communication tool, not just a data submission system.
12. Facilitates Planning and Resource Allocation
- HMIS data is used for:
- District Health Action Plans (DHAP) - planning based on local data
- Budget allocation - directing funds to underperforming areas
- Human resource deployment - posting staff where gaps exist
- Procurement planning - medicines, equipment based on caseload data
- Identifying underserved populations - through facility-wise coverage data
13. Interoperability and Scalability
- Modern HMIS (like DHIS2 used globally) is interoperable with other systems:
- EWARS (outbreak surveillance)
- Laboratory information systems
- Community health worker tracking systems
- Telemedicine platforms
- Fully customizable to align with national reporting structures, disease priorities, and local administrative units.
- Can scale from small districts to entire nations.
Summary Table of Salient Features
| # | Feature | In Simple Words |
|---|---|---|
| 1 | Comprehensive data collection | Covers all health services at all levels |
| 2 | Multi-level hierarchical flow | Data goes from village clinic → national HQ |
| 3 | Standardized formats | Same forms everywhere = comparable data |
| 4 | Regular timely reporting | Monthly, quarterly, annual cycles |
| 5 | Indicator-based monitoring | Measurable targets to track progress |
| 6 | Dashboard and score cards | Visual performance tracking |
| 7 | Data quality assurance | Checks to catch errors and gaps |
| 8 | Web-based national portal | Centralized, accessible data repository |
| 9 | Programme integration | All health programmes in one system |
| 10 | Evidence-based decision making | Data drives planning, not guesswork |
| 11 | Feedback mechanism | Results shared back down the chain |
| 12 | Resource planning | Tells you where to send money, staff, medicines |
| 13 | Interoperability | Connects with other health systems |
One-Line Definition to Remember
HMIS = The system that turns raw health data from every clinic in the country into actionable information for managers to improve healthcare delivery.
sailent feature of hmis in nepal
salient features HMIS Nepal health management information system DoHS MoHP
Nepal HMIS system components data flow reporting health facilities annual report
https://www.slideshare.net/slideshow/health-management-infor…
Nepal HMIS established 1993 DHIS2 recording reporting forms features Management Division DoHS
Salient Features of HMIS in Nepal
Background: Why Was HMIS Established in Nepal?
- Lack of uniformity and standardization
- Duplication of effort and data
- Need for more resources
- Collection of unnecessary information
- Inability to compare or combine data across programs
Definition of HMIS in Nepal
Nepal's HMIS is an organized system of collecting, storing, processing, recording, reporting, and providing feedback of health information from grassroots service delivery points up to the central level - to assist monitoring, evaluation, and policy formulation.
Administrative Structure
| Body | Role |
|---|---|
| Ministry of Health and Population (MoHP) | Overall policy, strategy, oversight |
| Department of Health Services (DoHS) | Programme implementation, annual reports |
| Management Division (MD), DoHS | Directly responsible for HMIS - information management, planning, coordination, supervision, monitoring and evaluation |
| Regional Health Directorates (5 RHDs) | Regional coordination and supervision |
| District Health Offices / DPHO | District data aggregation, quality checks |
| Palika (Local Government - 753) | Local data collection and coordination since federalization |
| Health Facilities | Primary data recording and reporting |
Salient Features of Nepal's HMIS
1. Integration of Vertical Programs (Core Feature)
- Nepal's HMIS replaced fragmented, program-specific reporting with a single unified system.
- All major health programs report through the same platform:
- Reproductive, Maternal, Neonatal, Child and Adolescent Health (RMNCH+A)
- Immunization and Family Planning
- Vector-borne diseases (malaria, dengue, kala-azar)
- Tuberculosis, Leprosy, HIV/AIDS
- Non-communicable diseases (hypertension, diabetes)
- Emergency obstetric care (Aama Programme, CB-NCP)
- OPD/IPD, surgery, and inpatient services
- Key reform feature: Integration of vertical reporting systems such as EOC, Aama, CB-NCP, TB, HIV into one reporting format.
2. Hierarchical Multi-Level Data Flow
Health Post / Sub-Health Post / PHCC / Hospital
(Primary recording into registers)
↓ Monthly
Palika (Local Government - Ward / Municipality)
↓
District Health Office / DPHO (Data entry, aggregation)
↓
Province Health Directorate (7 Provinces)
↓
Department of Health Services (DoHS) - National Level
↓
MoHP → Annual Report (Published)
↑
Feedback flows back down at each level
- Palika-level data management is a key feature added after Nepal's federalization in 2017 - local governments now play a central role in data collection and use.
- The district office maintains copies of all facility reports (at least 10 months out of 12).
3. Standardized Recording and Reporting Forms
- HMIS uses standardized recording registers and reporting formats across all public health facilities in Nepal.
- Forms are designed and distributed by the Management Division, DoHS.
- Key standardized forms include:
- Outpatient register (OPD)
- Inpatient register (IPD)
- Antenatal care (ANC) register
- Delivery register
- Immunization register
- Family planning register
- Disease surveillance register
- Monthly reporting forms (aggregated and sent upward)
- These forms use ICD-10 codes for inpatient diagnoses at hospital level.
4. DHIS2 as the Electronic Platform (Since 2016)
- Nepal introduced DHIS2 (District Health Information Software 2) nationally in 2016 as the electronic platform for HMIS data management.
- DHIS2 is a free, open-source software used in 100+ countries worldwide, maintained by the University of Oslo.
- Key capabilities of DHIS2 in Nepal:
- Web-based data entry accessible from any location
- Offline data entry with synchronization when internet is available
- Automated data validation rules
- Real-time dashboards, charts, maps (GIS), pivot tables
- Data disaggregation by caste/ethnicity, age, sex
- API-based interoperability with other systems (TB, HIV, EWARS, LMIS)
- Accessible to federal, provincial, and local level managers
- Source: MoHP Nepal / PLOS ONE study
5. Disaggregation by Caste/Ethnicity and Geography
- A landmark feature of Nepal's revised HMIS is that selected indicators can be disaggregated by caste/ethnicity - enabling monitoring of health equity and identifying marginalized groups.
- Data is also disaggregated by:
- Sex (male/female)
- Age groups
- Geographic area (urban/rural, province, district, Palika)
- Facility type (health post, PHCC, district hospital, zonal hospital)
- This supports Nepal's constitutional commitment to equitable health service delivery.
6. Facility-Level Reporting
- Unlike older systems that only captured district-level consolidated data, Nepal's reformed HMIS enables facility-wise data reporting.
- Benefits of facility-level reporting:
- Identifies which specific facility has low or high coverage
- Pinpoints underserved populations geographically
- Monitors which facilities report on time (timeliness tracking)
- Allows data quality probing at the facility level
- Enables performance comparison between facilities
7. Regular and Periodic Reporting Cycle
| Frequency | What is Reported |
|---|---|
| Monthly | Service delivery data - OPD/IPD, ANC, deliveries, immunization, family planning |
| Quarterly | Programme-specific indicators (e.g., PNC coverage, anaemia detection) |
| Annual | Infrastructure, human resources, outcome indicators; Annual Report published |
| Weekly (EWARS) | Disease surveillance / outbreak alerts (separate but linked system) |
- The DoHS publishes the Annual Report of the Department of Health Services - Nepal's most important health data publication - entirely based on HMIS data.
- Reporting from the public sector is over 95%; however, only about 49% of the private sector is captured in the annual health report. - KUMJ Study
8. Coverage of Health Facilities
| Facility Type | Number |
|---|---|
| Health Posts (public) | 3,808 |
| Community Health Units | 314 |
| Urban Health Centres | 288 |
| Primary Health Care Centres | 288 |
| District Hospitals | 52 |
| General Hospitals (public + NGO) | 407 |
| Zonal/Regional/Central Hospitals | 10+ |
| Teaching Hospitals | 26 |
| Ayurveda Aushadhalaya | 309 |
- Source: WHO HIS Evaluation Nepal
9. Nine Routine Information Systems (HMIS is One of Nine)
- HMIS (Health Management Information System) - service statistics
- LMIS (Logistics Management Information System) - medicines and supplies
- HURIS (Human Resources Management Information System) - staff data
- HIIS (Health Infrastructure Information System) - buildings and equipment
- IMIS (Insurance Management Information System) - health insurance
- Vital Registration / CRVS (Civil Registration and Vital Statistics)
- Disease Surveillance Systems (EDCD / EWARS)
- Hospital Management Information Systems (individual hospitals)
- Community-level health worker tracking systems (e.g., FCHV data)
10. Indicator-Based Performance Monitoring
| Indicator Type | Nepal Example |
|---|---|
| Input | Number of skilled health personnel per facility |
| Process | % of ANC registrations in 1st trimester |
| Output | Institutional delivery rate; Immunization coverage |
| Outcome | Maternal Mortality Ratio; Under-5 mortality rate |
| Impact | Reduction in poverty-related disease burden |
- ANC 4+ visit rate, institutional delivery rate, PNC coverage
- Full immunization coverage, BCG/MR1 dropout rates
- Contraceptive prevalence rate
- ORS/Zinc use in diarrhea, IMCI coverage
- Bed occupancy rate, average length of stay
- TB treatment success rate, PMTCT coverage
11. Data Quality Assurance Mechanisms
- Validation rules in DHIS2 - logical error checks (e.g., ANC 4+ visits cannot exceed ANC 1st visit registrations)
- Routine Data Quality Assessment (RDQA) system at facility and Palika level
- Annual sample surveys - recorded data vs. reported data cross-checked at each level
- Field verification - random checks of HMIS data against physical registers
- Reporting completeness monitoring - tracking % of facilities that submitted reports
- Timeliness monitoring - tracking submission deadlines
- Data Quality Sweeps - daily monitoring introduced during COVID-19 response
12. Feedback Mechanism
- Feedback is provided from the central/district level back down to health facilities - a two-way information flow.
- Feedback includes: performance analysis, benchmarks, problem identification, and corrective action guidance.
- SMS and digital notifications alert facilities about missing or overdue reports.
- Monthly review meetings at PHC and district level use HMIS data for performance review and planning.
13. Annual Report Publication
- Nepal's DoHS Annual Report is the flagship publication produced from HMIS data.
- Published every year covering:
- Service delivery statistics by programme
- Coverage indicators by province and district
- Disease-wise morbidity and mortality data
- Infrastructure and human resource data
- Progress toward national health targets (NHSS, SDGs)
- It is the primary reference for Nepal's health policymakers, planners, researchers, and development partners.
14. Federal Structure Adaptation (Post-2017)
- HMIS was restructured to align with the new governance structure
- Palikas now collect reports from health facilities within their jurisdiction, keep a copy, and forward to DHO/DPHO
- Provincial Health Directorates manage province-level data
- Data management responsibilities were clarified across three levels
- A web-based Master Health Facility Registry with unique IDs for each facility was developed to support local government registration
15. Integration with Other Systems
| System | Integration |
|---|---|
| EWARS | DHIS2-based weekly disease alert data feeds into HMIS dashboard |
| LMIS | Logistics data integrated for supply chain management |
| TB/HIV programs | Data modules interface directly with HMIS via APIs |
| eHealth/EMR | Bahmni EMR at select hospitals (Bayalpata, Trishuli) interfaces with DHIS2 |
| IMIS | Health insurance data being made compatible with DHIS2-HMIS |
Summary of Salient Features at a Glance
| # | Feature | Key Point |
|---|---|---|
| 1 | Integrated system | Replaced fragmented vertical program reporting (since 1993/94) |
| 2 | Multi-level data flow | Health post → Palika → District → Province → National |
| 3 | Standardized forms | Uniform recording/reporting formats across all facilities |
| 4 | DHIS2 platform | Electronic, web-based, offline-capable since 2016 |
| 5 | Caste/ethnicity disaggregation | Equity-focused health monitoring |
| 6 | Facility-level reporting | Individual facility performance trackable |
| 7 | Regular reporting cycles | Monthly, quarterly, annual |
| 8 | Wide facility coverage | 5,500+ public health facilities |
| 9 | One of 9 routine IS | Works alongside LMIS, HURIS, HIIS, IMIS, etc. |
| 10 | Indicator-based monitoring | Input → process → output → outcome → impact |
| 11 | Data quality assurance | Validation rules, RDQA, field verification |
| 12 | Feedback mechanism | Two-way information flow |
| 13 | Annual Report | DoHS Annual Report is key national health publication |
| 14 | Federalized structure | Aligned with Nepal's 3-tier governance (post-2017) |
| 15 | System integration | Linked with EWARS, LMIS, TB, HIV, insurance systems |
In one sentence: Nepal's HMIS is a federally structured, DHIS2-powered, integrated health data system managed by the Management Division of DoHS that collects routine health service data from over 5,500 facilities, flows it through Palika → District → Province → National levels, and produces the Annual DoHS Report used for evidence-based health planning and policymaking.
what are soil transmitted helminth
"soil-transmitted helminths"[MeSH Terms] AND prevention
Soil-Transmitted Helminths (STH)
Definition
STHs are transmitted via soil - hence the name. They cannot spread directly person to person because eggs passed in feces need approximately 3 weeks to mature in soil before becoming infective.
- Park's Textbook of Preventive and Social Medicine
The Main Species
| Common Name | Scientific Name | Disease |
|---|---|---|
| Giant roundworm | Ascaris lumbricoides | Ascariasis |
| Whipworm | Trichuris trichiura | Trichuriasis |
| Hookworm (New World) | Necator americanus | Hookworm disease |
| Hookworm (Old World) | Ancylostoma duodenale | Hookworm disease |
| Threadworm | Strongyloides stercoralis | Strongyloidiasis (sometimes classified separately) |
- Sherris & Ryan's Medical Microbiology 8e; Jawetz Medical Microbiology 28e
Global Burden
- More than 1.5 billion people (about 24% of the world's population) are infected.
- Greatest burden in sub-Saharan Africa, the Americas, China, and East Asia.
- Over 267 million pre-school children and 568 million school-age children live in areas of intense transmission.
- Hookworm alone affects ~460 million people globally.
- STHs collectively infect more than 25% of all humans.
- Park's Textbook; Sherris & Ryan's Medical Microbiology 8e
Mode of Transmission
For Ascaris and Whipworm (via ingestion of eggs):
- Contaminated vegetables/salads not carefully washed, peeled, or cooked
- Contaminated water sources
- Children playing in contaminated soil and putting unwashed hands in their mouth
For Hookworm (via skin penetration - unique!):
- Eggs hatch in warm, moist soil → larvae develop into infective filariform larvae in 5-10 days
- These larvae actively penetrate human skin, most commonly through bare feet
- Ancylostoma duodenale larvae can also infect by mouth
- They move upward on blades of grass, lying in wait for a host
Key principle: There is NO direct person-to-person transmission. Reinfection only occurs through renewed contact with contaminated environment.
Life Cycles and Body Migration
1. Ascaris lumbricoides (Roundworm)
Embryonated egg ingested
↓
Hatches in small intestine → larvae penetrate gut wall
↓
Travel via blood to LIVER → LUNGS (Loeffler's syndrome phase)
↓
Break through alveoli → bronchioles → trachea → coughed up → swallowed
↓
Reach small intestine → mature into adults in 60-80 days
↓
Adults live in intestine (6-12 months lifespan)
↓
Females produce ~240,000 eggs/day → passed in feces → soil
2. Trichuris trichiura (Whipworm)
Embryonated egg ingested
↓
Larvae hatch in small intestine
↓
Migrate to large intestine (caecum, colon) → burrow into mucosa
↓
Adults live in colon (anterior end buried in mucosa)
↓
Eggs passed in feces → embryonate in soil (3-4 weeks)
- No pulmonary migration phase
- Route of infection: mouth only
3. Hookworm (Necator americanus / Ancylostoma duodenale)
Infective filariform larva penetrates skin (bare feet)
↓
Travel via blood to LUNGS
↓
Break into alveoli → trachea → swallowed
↓
Reach small intestine (jejunum) → attach to villi with "hooks"
↓
Suck blood actively → cause iron deficiency anemia
↓
Eggs passed in feces → hatch in soil → rhabditiform → filariform larvae
| Feature | A. duodenale | N. americanus |
|---|---|---|
| Size | 10-13mm (F), 8-11mm (M) | Slightly smaller |
| Eggs/day per female | 10,000-30,000 | 5,000-10,000 |
| Adult lifespan | ~1 year | ~4 years |
| Distribution | Mediterranean, South Asia | Tropical Africa, Americas |
1. Ascariasis - Clinical Features
| Worm Load | Symptoms |
|---|---|
| Light (WHO: <50 worms) | Usually asymptomatic |
| Heavy (WHO: ≥50 worms) | Intestinal manifestations |
- Pulmonary phase (larval migration): cough, wheezing, eosinophilia, fever - Loeffler's syndrome
- Intestinal phase: abdominal pain, nausea, vomiting, diarrhea, malnutrition, growth retardation
- Complications: intestinal obstruction (worm mass), volvulus, intussusception, biliary obstruction (worm migrating into bile duct), bowel perforation
- Contributes significantly to malnutrition and Vitamin A deficiency in children
2. Trichuriasis - Clinical Features
- Light infections: usually asymptomatic
- Moderate/Heavy infections: abdominal pain, chronic diarrhea, dysentery (bloody mucous diarrhea)
- Massive infection in children: rectal prolapse (characteristic complication), Trichuris dysentery syndrome, growth retardation, anemia
- Heavy infection: WHO definition ≥10,000 eggs/gram of feces
3. Hookworm Infection - Clinical Features
| Stage | Manifestation |
|---|---|
| Entry (skin) | "Ground itch" - local itching, rash at entry site (feet) |
| Pulmonary (migration) | Cough, wheeze, eosinophilia |
| Intestinal (adult worms) | Abdominal pain, diarrhea, nausea |
| Chronic (blood loss) | Iron deficiency anemia (main impact), hypoalbuminemia, edema |
- Each adult hookworm sucks 0.03-0.15 mL blood/day from intestinal mucosa
- Iron deficiency anemia is the most important consequence, especially in pregnant women and children
- Hypoproteinemia and edema in heavy infections
- Impaired physical and cognitive development in children
Shared Effects of STH on Children
| Effect | Mechanism |
|---|---|
| Malnutrition | Compete for nutrients, reduce appetite, cause malabsorption |
| Anemia | Blood loss (hookworm) + nutritional competition |
| Stunted growth | Chronic nutrient deprivation |
| Impaired cognition | Malnutrition affecting brain development |
| Reduced school attendance | Illness burden |
| Impaired immune development | Chronic parasitism |
Diagnosis
| Method | Details |
|---|---|
| Stool microscopy (wet mount) | Direct smear or concentration method - identifies eggs |
| Kato-Katz technique | Semi-quantitative - counts eggs per gram of feces (EPG) - standard for surveys |
| Harada-Mori method | Filter paper larval culture - differentiates hookworm species |
| NAAT/PCR | Research settings; high sensitivity and specificity |
| Parasite | Egg Appearance |
|---|---|
| Ascaris | Bile-stained, mammillated (bumpy outer coat); 60x45 μm |
| Trichuris | Barrel/football-shaped with bipolar mucoid plugs; 50x22 μm |
| Hookworm | Thin-shelled, oval, 4-8 cell stage when passed; 60x40 μm |
Treatment
| Drug | Dose | Coverage |
|---|---|---|
| Albendazole | 400 mg single dose (adults and children >2 yrs) | All STHs |
| Mebendazole | 500 mg single dose | All STHs |
| Ivermectin | 200 mcg/kg | Strongyloides; used in combination for STH |
- Both albendazole and mebendazole are donated by WHO for mass drug administration (MDA) programmes.
- Single-dose treatment is effective, easy to administer by non-medical personnel.
- Park's Textbook of Preventive and Social Medicine
Prevention and Control
1. Preventive Chemotherapy (Mass Drug Administration - MDA)
| Community STH Prevalence | Deworming Frequency |
|---|---|
| >20% | Once a year |
| >50% | Twice a year |
- Target groups: pre-school children, school-age children, women of reproductive age, pregnant women (2nd and 3rd trimester)
- Integrated with school health programs, child health days, and supplementation programs
2. Sanitation
- Construction and use of latrines - prevent open defecation
- Safe disposal of human feces
- Improvement of sewage systems
3. Personal Hygiene
- Handwashing with soap before eating and after defecation
- Wearing shoes/footwear - prevents hookworm skin penetration
- Washing and cooking vegetables properly
4. Safe Water and Food
- Drink clean/treated water
- Wash vegetables thoroughly before consumption
- Avoid using raw human feces as fertilizer (night soil)
5. Health Education
- Community awareness about transmission routes, hygiene, and sanitation
Summary Table
| Feature | Ascaris | Trichuris | Hookworm |
|---|---|---|---|
| Common name | Roundworm | Whipworm | Hookworm |
| Size | 20-35 cm | 30-50 mm | 8-13 mm |
| Entry route | Mouth (eggs) | Mouth (eggs) | Skin (larvae) |
| Pulmonary migration | Yes (Loeffler's) | No | Yes |
| Site in body | Small intestine | Large intestine | Small intestine (jejunum) |
| Key complication | Obstruction, biliary | Rectal prolapse | Iron deficiency anemia |
| Egg production/day | 240,000 | 3,000-20,000 | 5,000-30,000 |
| Treatment | Albendazole/Mebendazole | Albendazole/Mebendazole | Albendazole/Mebendazole |
In summary: STHs are the world's most widespread parasitic infections, thriving wherever open defecation and poor sanitation exist. They silently rob millions of children of nutrition, growth, and cognitive potential. The WHO's global strategy - periodic deworming + improved sanitation + hygiene education - aims to eliminate STH-related morbidity in children worldwide.
epidemiological triad of helminthiasis
Epidemiological Triad of Helminthiasis
The Epidemiological Triad - Concept
"The above model - agent, host and environment - has been in use for many years. It helped epidemiologists to focus on different classes of factors, especially with regard to infectious diseases." - Park's Textbook of Preventive and Social Medicine
Applied to Helminthiasis (STH)
- Ascaris lumbricoides (roundworm) - Ascariasis
- Trichuris trichiura (whipworm) - Trichuriasis
- Necator americanus / Ancylostoma duodenale (hookworms) - Hookworm disease
LEG 1: AGENT FACTORS
A. Agent Factors in Ascariasis (Ascaris lumbricoides)
| Property | Details |
|---|---|
| Taxonomic class | Nematoda (roundworm) |
| Adult habitat | Lumen of small intestine (moves freely) |
| Size | Female: 20-35 cm; Male: 12-30 cm |
| Egg production | ~240,000 eggs/day per female (extremely high) |
| Infective form | Embryonated egg (requires 2-3 weeks in soil) |
| Infectivity | High - eggs resistant to many disinfectants |
| Egg viability | Months to years in soil under favourable conditions |
| Reservoir | Man is the only reservoir |
| Infective material | Feces containing fertilized eggs |
| Period of communicability | Until all fertile females destroyed; stools negative |
| Life span of adult | 6-12 months (max 1.5 years) |
B. Agent Factors in Trichuriasis (Trichuris trichiura)
| Property | Details |
|---|---|
| Taxonomic class | Nematoda (whipworm) |
| Adult habitat | Caecum and colorectum (anterior end embedded in mucosa) |
| Size | Male: 30-45 mm; Female: 30-35 mm |
| Egg production | 200-10,000 eggs/day; female lives >5 years |
| Infective form | Embryonated egg (embryonization takes 21 days in soil) |
| Resistance | Can withstand cold temperatures; killed by desiccation (dryness) |
| Infective material | Feces; infection is directly from feces |
| Life span of adult | Over 5 years (long-lived) |
C. Agent Factors in Hookworm Infection (N. americanus / A. duodenale)
| Property | Details |
|---|---|
| Taxonomic class | Nematoda (hookworm) |
| Adult habitat | Small intestine (jejunum) - attached to villi |
| Size | Male: 8-11 mm; Female: 10-13 mm; anterior end dorsally curved |
| Egg production | A. duodenale: 10,000-30,000/day; N. americanus: 5,000-10,000/day |
| Infective form | Filariform larva (L3) - unique: penetrates skin actively |
| Development in soil | Egg → rhabditiform larva (1-2 days) → filariform larva (5-10 days) |
| Larval viability | Up to 1 month in moist, shaded soil |
| Reservoir | Man is the only important reservoir |
| Infective material | Soil contaminated with infective larvae (immediate source) |
| Life span | A. duodenale: ~1 year; N. americanus: ~4 years |
| Pathogenic mechanism | Suck blood from intestinal mucosa → iron deficiency anemia |
LEG 2: HOST FACTORS
A. Host Factors in Ascariasis
| Host Factor | Details |
|---|---|
| Age | Infection rates highest in children aged 3-8 years; they are the most important disseminators |
| Immunity | Adults develop some resistance; high host-parasite tolerance |
| Nutrition | Worms compete for food and possibly Vitamin A; worsens malnutrition |
| Worm load | Disease severity directly proportional to number of worms harboured |
| Behavior | Children playing on contaminated soil, putting hands in mouth |
| Susceptibility | Universal; no natural solid immunity |
B. Host Factors in Trichuriasis
| Host Factor | Details |
|---|---|
| Age | Children most affected; heavy infections worse in children |
| Worm burden | Light infections (most) - asymptomatic; heavy infections - dysentery, rectal prolapse |
| Nutritional status | Poor nutrition aggravates the severity |
| Immunity | Partial acquired immunity in adults; children remain highly susceptible |
| Cognitive development | Heavy infection impairs school performance and cognitive function |
C. Host Factors in Hookworm
| Host Factor | Details |
|---|---|
| Age and sex | All ages and both sexes susceptible; highest incidence in 15-25 year age group in endemic areas |
| Nutrition | Malnutrition is a predisposing factor; well-nourished individuals with adequate iron intake are less severely affected |
| Host-parasite balance | In endemic areas, inhabitants develop a balance - harbour parasite without clinical signs; infection rate may reach 100% but most are light infections |
| Occupation | Higher prevalence in agricultural workers than town workers; an occupational disease of farming communities in many tropical countries |
| Immunity | Little known; delicate balance upset by malnutrition and intercurrent infections |
| Iron stores | Pre-existing iron deficiency (common in women, children) worsens clinical disease |
LEG 3: ENVIRONMENTAL FACTORS
A. Environmental Factors in Ascariasis
| Factor | Role |
|---|---|
| Soil type | Clay soils are most favourable for Ascaris egg development |
| Temperature | Low temperature inhibits egg development; high UV/sunlight kills eggs |
| Moisture | Adequate moisture needed for egg embryonation |
| Oxygen | Required for development |
| Open defecation | Seeding of soil - the most important factor for widespread distribution |
| Sanitation | Lack of latrines allows fecal-oral contamination cycle |
| Crowding | Concentration of infection around houses of young children |
| Food handling | Use of untreated night soil (human feces) as crop fertilizer |
| Water supply | Contaminated water sources transmit eggs |
B. Environmental Factors in Trichuriasis
| Factor | Role |
|---|---|
| Soil | Eggs embryonate in soil (21 days required) |
| Temperature | Can withstand cold; killed by drying/desiccation |
| Moisture | Essential for egg survival |
| Sanitation | Poor fecal disposal allows soil contamination |
| Open defecation | Primary driver of soil seeding with eggs |
| Vegetable contamination | Eggs on raw vegetables consumed unwashed |
C. Environmental Factors in Hookworm
| Factor | Role |
|---|---|
| Soil type | Damp, sandy, or friable soil with decaying vegetation - most favourable. Sandy > clay for hookworm (opposite of Ascaris) |
| Temperature | 24-32°C optimal; eggs fail to develop <13°C; larvae killed at 45-50°C |
| Oxygen | Required for growth and development of larvae |
| Moisture | Essential; dryness rapidly fatal to larvae |
| Rainfall | Adequate rainfall (≥40 inches/year) promotes larval survival |
| Shade | Larvae seek shade; direct sunlight kills them |
| Barefoot walking | Walking on contaminated soil = skin penetration |
| Sanitation | Lack of latrines - defecation in soil used for agriculture |
| Occupation | Farming communities - bare feet + contaminated soil + warm climate |
| Altitude | Less common at high altitudes (cold temperatures unfavourable) |
The Triad in Summary - All Three STHs
ENVIRONMENT
(the soil between them)
/ \
/ Contaminated soil, \
/ poor sanitation, \
/ warm/moist climate, \
/ open defecation \
/ \
AGENT ———————————————————————————— HOST
(Worm/Eggs/Larvae) (Human)
Ascaris: eggs in soil Children 3-8 yrs
Trichuris: eggs in soil Agricultural workers
Hookworm: larvae in soil Malnourished, barefoot
| Component | Ascariasis | Trichuriasis | Hookworm |
|---|---|---|---|
| Agent | A. lumbricoides eggs | T. trichiura eggs | N. americanus/A. duodenale filariform larvae |
| Entry | Oral (eggs) | Oral (eggs) | Skin penetration |
| Key host factor | Children 3-8 yrs | Children, heavy worm load | Age 15-25, farmers, malnourished |
| Key env. factor | Clay soil, open defecation | Moist soil, poor sanitation | Sandy moist soil, barefoot, warm (24-32°C) |
| Reservoir | Man only | Man only | Man only |
Breaking the Triad = Disease Control
"The primary mission of epidemiology is to provide information that results in breaking one of the legs of the triangle, thereby disrupting the connection among environment, host, and agent, and stopping the outbreak." - Park's Textbook
| Target | Intervention |
|---|---|
| AGENT | Deworming (albendazole/mebendazole) - kill adult worms |
| HOST | Nutrition improvement, iron supplementation, health education, wearing shoes |
| ENVIRONMENT | Sanitary latrines, safe water, food hygiene, avoid using night soil as fertilizer |
- Park's Textbook of Preventive and Social Medicine (primary source throughout)
- Sherris & Ryan's Medical Microbiology 8e
WASH programme of nepal sailent concept and features
Nepal WASH programme salient features concepts water sanitation hygiene national policy 2024
Nepal WASH sector plan ODF open defecation free SDG6 MoWS features components
https://giwmscdnone.gov.np/media/pdf_upload/Draft_WASH_SDP_P…
https://www.fsmtoolbox.com/assets/pdf/25._SDP_-_Final-_Eng.p…
WASH Programme of Nepal - Salient Concepts and Features
What is WASH?
Nepal recognizes access to safe water, sanitation, and hygiene as a fundamental human right under the Constitution of Nepal 2015, which states every citizen has the right to live in a healthy and clean environment.
Governing Structure
| Body | Role |
|---|---|
| Ministry of Water Supply (MoWS) | Lead ministry for WASH in Nepal |
| Department of Water Supply and Sewerage Management (DWSSM) | Implementation and technical oversight |
| National Sanitation and Hygiene Coordination Committee (NSHCC) | Multi-sector coordination |
| Provincial and Local Governments (753 Palikas) | Frontline WASH delivery after federalization |
| Water Users' and Sanitation Committees (WUSCs) | Community-level management |
| Development Partners | UNICEF, WHO, World Bank, ADB, INGO support |
Key Policy and Planning Documents
| Document | Year | Significance |
|---|---|---|
| National Sanitation Policy | 1994 | First dedicated sanitation policy |
| Rural Water Supply and Sanitation National Policy | 2004 | Guided rural WASH expansion |
| Urban Water Supply and Sanitation Policy | 2009 | Urban-specific framework |
| Sanitation and Hygiene Master Plan | 2011 | Roadmap for ODF achievement |
| WASH Sector Development Plan (SDP 2016-2030) | 2016 | Aligned with SDG 6; current guiding plan |
| National Policy for Water Supply, Sanitation and Hygiene (NP-WASH 2025) | 2025 | Latest comprehensive national WASH policy |
| Draft WASH SDP (2024-2043) | 2024 | 20-year strategic roadmap |
WASH SDP Vision Statement
"Assured, safe, and easily accessible water supply and sanitation services, and hygiene." Goal: By 2100 BS (2043 AD), secure universal access to safe water supply and sanitation, accomplishing the SDGs. - Draft WASH SDP 2024-2043
Salient Concepts of Nepal's WASH Programme
1. WASH as a Fundamental Human Right
- The Constitution of Nepal 2015 guarantees clean water and sanitation as a constitutional right.
- The NP-WASH 2025 explicitly states: "Recognise WASH as a basic human right, prioritising it over other water uses and ensuring affordability, equitable access, and gender-responsive design."
- This rights-based approach means WASH is not merely a development goal but a legal entitlement of every citizen.
2. Open Defecation Free (ODF) Nepal - Core Concept
- 1994 - National Sanitation Policy first identified sanitation as a health priority
- 2003 - Community-Led Total Sanitation (CLTS) launched
- 2004 - School-Led Total Sanitation programme introduced
- 2011 - Sanitation and Hygiene Master Plan published - roadmap for ODF
- 2019 - Nepal declared Open Defecation Free (ODF) - a landmark achievement
- No person defecates in the open (fields, forests, water bodies, roadsides)
- Every household has access to and uses a toilet/latrine
- Pour-flush latrine with single offset pit/septic tank is most common (93% of ODF-certified households)
3. Three-Pillar Structure of WASH
W A S H
/ | \
/ | \
WATER SANITATION HYGIENE
| Pillar | Coverage Goals | Current Status (JMP) |
|---|---|---|
| Water Supply | Safe, reliable drinking water for all | 58% basic; 19% safely managed; 88% system coverage |
| Sanitation | Improved toilets; safe fecal disposal; wastewater management | 61% safely managed toilets; 5% wastewater safely treated |
| Hygiene | Handwashing, menstrual hygiene, food hygiene | >80% access to water + soap |
4. JMP Service Ladder Framework
| Level | Water | Sanitation |
|---|---|---|
| Safely managed | On-premises, available when needed, free of contamination | Uses improved facility, not shared, waste safely treated |
| Basic | Improved source, collection time ≤30 min | Improved facility, not shared |
| Limited | Improved source, collection >30 min | Shared improved facility |
| Unimproved | Unprotected well/spring | Pit latrine without slab, hanging latrine |
| No service | Surface water | Open defecation |
Salient Features of Nepal's WASH Programme
Feature 1: Community-Led Total Sanitation (CLTS)
- Launched in Nepal in 2003 - a behaviour change approach that does not offer subsidies for toilet construction.
- Instead, it triggers communities to self-recognize the problem of open defecation through participatory tools (village mapping, fecal-oral transmission pathways, "walk of shame").
- The community collectively takes responsibility and action - no individual household subsidy.
- Communities are then certified ODF after verification.
- This community ownership model was fundamental to Nepal achieving ODF status.
Feature 2: Gender Equality and Social Inclusion (GESI)
- Nepal's WASH programme explicitly mainstreams GESI across all activities.
- 33% mandatory representation of women in Water Users' and Sanitation Committees (WUSCs).
- Special attention to Women, Poor and Excluded (WPE) groups and marginalized communities.
- Four GESI dimensions addressed:
- Gender - women's specific needs, menstrual hygiene management (MHM)
- Caste/ethnic groups/religious minorities
- Remoteness - geographically disadvantaged communities
- Poverty - cross-subsidy mechanisms for the poorest
- Cross-subsidy mechanism: profiting utilities support WASH access for the poor within communities (installation costs, tariff relief).
- Disability-inclusive and child-friendly WASH facilities are mandated.
Feature 3: Menstrual Hygiene Management (MHM)
- Specifically addressed in Nepal's WASH policy as a cross-cutting hygiene priority.
- Nepal has faced cultural challenges including Chhaupadi (practice of isolating menstruating women in remote western Nepal).
- WASH programme includes:
- Menstrual hygiene education in schools
- Construction of separate, private, gender-sensitive toilet facilities in schools and health facilities
- Distribution of sanitary materials in remote areas
- Legal prohibition of Chhaupadi (Penal Code amendment)
Feature 4: WASH in Schools (WinS) and Health Care Facilities (WinHCF)
- Every school must have functional water supply, separate toilets for boys and girls, and handwashing stations.
- Hygiene education integrated into school curricula.
- Students are key agents of change who carry hygiene messages home.
- School-Led Total Sanitation (2004) - students motivate families toward ODF.
- National Standards for WASH in Health Care Facilities (Draft 2019) developed.
- Functional water, sanitation, and hygiene required at all hospitals, PHCCs, and health posts.
- Critical for infection prevention and control, maternal care, and patient dignity.
Feature 5: Decentralised Federal Governance
| Level | Responsibility |
|---|---|
| Federal | National policy, standards, planning, funding allocation |
| Provincial | Provincial WASH plans, coordination, technical support |
| Local (Palika) | WASH service delivery, community schemes, local plans |
- 753 local governments (Palikas) are now the primary WASH service providers.
- Each Palika is expected to prepare a local-level WASH plan aligned with national SDP.
- NWASH-MIS (Management Information System) tracks local WASH expenditure and progress.
Feature 6: "One House - One Connection" Principle
- The sector vision is: "Accessible safe water and sanitation services for all" through the "one house one connection" principle.
- Every household to have its own functional water connection and private toilet.
- Eliminates dependence on shared facilities and open sources.
Feature 7: Climate Resilience and Disaster WASH
- Nepal is highly vulnerable to floods, landslides, droughts, and earthquakes.
- NP-WASH 2025 integrates Integrated Water Resources Management (IWRM) principles to minimize climate and environmental risks.
- WASH in emergencies is a dedicated theme in SDP.
- Climate-resilient infrastructure designs are prioritized.
- Disaster-responsive technologies and nature-based solutions promoted.
- Circular economy principles applied to wastewater management.
Feature 8: Total Sanitation and Behaviour Change Communication (BCC)
| Strategy | Details |
|---|---|
| CLTS | Community-Led Total Sanitation - no subsidies, collective action |
| SLTS | School-Led Total Sanitation - students as change agents |
| Mass media campaigns | TV, radio, social media for hygiene messages |
| IEC materials | In local languages and culturally appropriate formats |
| Global observances | World Water Day, Global Handwashing Day - Nepal actively participates |
| Health education | Integration into school curricula |
| Social mobilization | Community volunteers, FCHVs (Female Community Health Volunteers) |
Feature 9: Sanitation Marketing
- Recognizing that pure BCC alone is insufficient, Nepal uses sanitation marketing to stimulate demand and supply for improved toilets.
- Promotes affordable latrine designs, local supply chains for toilet materials, and private sector involvement.
- Used especially in Terai districts (8 districts including Saptari, Siraha, Dhanusa, Mahottari, Sarlahi, etc.) where sanitation coverage was only 35-50%.
Feature 10: Wastewater and Fecal Sludge Management (FSM)
- Going beyond toilets, Nepal addresses safe treatment of waste - a newer but critical component.
- Currently only 5% of wastewater is safely treated (JMP) - a major gap.
- Institutional and Regulatory Framework for Faecal Sludge Management in Urban Areas published (2017).
- Faecal sludge from pit latrines and septic tanks needs collection, transport, treatment, and safe disposal.
- Urban WASH policy includes wastewater standards for industries and establishments discharging to public sewers.
Feature 11: Private Sector and NGO Engagement
- NP-WASH 2025 explicitly encourages private sector and NGO investment in WASH infrastructure, service delivery, and technology.
- Corporate Social Responsibility (CSR) approaches encouraged from profitable utilities.
- Establishments (hotels, malls, hospitals, schools) must ensure adequate WASH facilities as a licensing precondition.
- Social entrepreneurs are promoted as innovative service providers.
Feature 12: WASH Financing and Investment
| Indicator | Status |
|---|---|
| Current WASH expenditure | ~2.8% of GDP |
| Funding gap | ~2% of GDP (insufficient) |
| Total cost of WASH SDP (2024-2043) | NRs. 4,272,228 million (~2023 prices) |
| 71.9% of water projects (2018) | Not well-functioning - need repair/rehabilitation |
- Sustainable financing is a major challenge - current funding only covers capital costs; operation and maintenance (O&M) severely underfunded.
- Life cycle cost assessment, financial expenditure tracking, and JMP/GLAAS indicators used for data-driven financing decisions.
Current WASH Status at a Glance (JMP Indicators)
| Service | Coverage |
|---|---|
| Basic water supply | 58% of population |
| Safely managed water supply | 19% |
| Water system coverage | 88% |
| Safely managed sanitation (toilets) | 61% |
| Wastewater safely treated | 5% |
| Access to water + soap for handwashing | >80% |
| ODF status | Achieved (2019) - being maintained |
Summary: Salient Features at a Glance
| # | Feature | Key Concept |
|---|---|---|
| 1 | Constitutional right | WASH is a legal human right in Nepal |
| 2 | ODF achievement | Nepal declared Open Defecation Free in 2019 |
| 3 | Three pillars | Water + Sanitation + Hygiene are inseparable |
| 4 | JMP ladder | Progress from no service → safely managed |
| 5 | CLTS | Community-led, no-subsidy behaviour change for ODF |
| 6 | GESI | 33% women in committees; equity for marginalized groups |
| 7 | MHM | Menstrual hygiene as core hygiene component |
| 8 | WASH in Schools/HCF | Students as change agents; facility standards |
| 9 | Federalization | 753 Palikas as primary WASH service providers |
| 10 | One house-one connection | Universal individual access goal |
| 11 | Climate resilience | IWRM, disaster WASH, nature-based solutions |
| 12 | FSM/Wastewater | Beyond toilets to safe waste treatment |
| 13 | Sanitation marketing | Demand-supply approach for toilet adoption |
| 14 | BCC/Mass media | Behaviour change through education and campaigns |
| 15 | Sustainable financing | Life-cycle costs, O&M funding, private sector |
In summary: Nepal's WASH programme has evolved from a basic sanitation campaign to a comprehensive, rights-based, federally governed, climate-sensitive, and equity-focused national initiative. The achievement of ODF in 2019 was a milestone, but the bigger challenge now is moving from basic access to safely managed water and sanitation for every citizen - leaving no one behind.
IMNCI Programme nepal
IMNCI programme Nepal integrated management neonatal childhood illness features components DoHS
https://www.slideshare.net/slideshow/integrated-management-o…
CB-IMNCI Nepal FCHVs community based newborn care key family practices indicators monitoring DoHS annual report
IMNCI Programme in Nepal
What is IMNCI?
Historical Development in Nepal (Chronological)
1983 → Control of Diarrhoeal Disease (CDD) Programme initiated
↓
1987 → Acute Respiratory Infection (ARI) Control Programme initiated
↓
1997 → Evaluation: Treatment model > Referral model at community level
↓
1997/98 → ARI + CDD combined → CB-AC Programme
↓
1998/99 → Nutrition + Immunization added → CBAC Programme
↓
1999 → Government merged CBAC into IMCI →
"Community-Based Integrated Management of Childhood Illness (CB-IMCI)"
(covers: Pneumonia, Diarrhoea, Malaria, Measles, Malnutrition)
↓
2003 → IMCI piloted in Mahottari district, expanded nationally
↓
2004-2005 → Community-Based Newborn Care Programme (CB-NCP) piloted
(Morang Innovative Neonatal Intervention Program)
↓
2009 → CB-IMCI implemented in all 75 districts of Nepal
↓
2012 → CB-NCP scaled up - treatment for neonatal sepsis rose from 3% → 75%
↓
October 14, 2014 (2071/6/28) → CB-IMCI + CB-NCP merged →
"CB-IMNCI" - Community-Based Integrated Management of
Neonatal and Childhood Illnesses (current programme)
- Source: DoHS Annual Reports; PMC10900553
Why Integration? The Rationale
- A child with pneumonia may also be malnourished
- A febrile child may have malaria AND measles
- A child with diarrhea may also have ear infection
An integrated approach is therefore necessary - cost-effective, comprehensive, and emphasizes prevention, promotion, AND standard case management. - Park's Textbook of Preventive and Social Medicine
Three Components of the IMNCI Strategy
IMNCI STRATEGY
/ | \
/ | \
Case Management Health Community &
at Health System Family
Facilities Strengthening Practices
(FB-IMNCI) (CB-IMNCI)
All three components must be implemented simultaneously for maximum effectiveness.
Component 1: Case Management at Health Facilities (FB-IMNCI)
- Standardized assessment, classification, and treatment of sick children using algorithmic guidelines
- Health workers follow color-coded triage and classification charts
- Addresses: pneumonia, diarrhea, malaria, measles, malnutrition, ear problems, fever
Component 2: Health System Strengthening
- Training and supervision of health workers
- Supply of essential medicines (amoxicillin, ORS, zinc, iron, chlorhexidine)
- Development of IMNCI training sites
- Referral system strengthening
Component 3: Community and Family Practices (CB-IMNCI)
- Promotion of key family and community practices for child health
- FCHVs as the backbone of community-level delivery
- Health education, counseling, and distribution of commodities at household level
CB-IMNCI: Nepal's Community-Based Model
Age Groups Covered:
| Age Group | Programme Focus |
|---|---|
| 0-28 days (Newborn) | Birth asphyxia, bacterial infection (neonatal sepsis), jaundice, hypothermia, low birth weight, breastfeeding counseling |
| 29 days - 2 months (Young infant) | Infection, jaundice, hypothermia, breastfeeding support |
| 2 months - 5 years (Child) | Pneumonia, diarrhea, malaria, measles, malnutrition, ear problems, fever |
Role of FCHVs (Female Community Health Volunteers)
FCHVs' Role in CB-IMNCI:
| Function | Activity |
|---|---|
| Health promotion | Maternal, newborn, and child health education at household and community level |
| Commodity distribution | Iron, zinc tablets, ORS packets, chlorhexidine (4% gel for umbilical cord care) - NO diagnostic skills required |
| Referral | Immediate referral of newborns and children with danger signs to health facilities |
| Monthly mother's group meetings | Community education sessions, counseling, and health promotion |
| Register maintenance | Complete monthly registers and submit reports to health facilities |
| Postnatal home visits | Support breastfeeding, warmth, cord care, danger sign recognition |
FCHVs are selected by the local community - this gives them credibility, acceptance, and sustained presence in communities. They are not paid but are given incentives and recognition.
Health Workers' Role (at health posts/PHC/ORC):
- Counsel and provide health services for non-breathing cases, low birth weight babies
- Manage common childhood illnesses and neonatal sepsis
- Conduct postnatal visits through Primary Health Care Outreach Clinics (PHC/ORC)
- Provide facility-based management using FB-IMNCI guidelines
IMNCI vs Original IMCI - Key Differences
| Feature | WHO/UNICEF IMCI | Nepal's IMNCI |
|---|---|---|
| Coverage of 0-6 days | No | Yes |
| Basic Health Care Module | No | Yes |
| Home visit for newborn by provider | No | Yes |
| Training for home-based newborn care | No | Yes |
| Training days for newborns/young infants | 2 out of 11 days | 4 out of 11 days |
| Sequence of training | Child first, then young infant | Young infant first, then child |
| National malaria/anaemia guidelines | Standard | Adapted to Nepal context |
Disease-Specific Classification System
A. Pneumonia Classification:
| Classification | Signs | Action |
|---|---|---|
| Severe pneumonia / Very severe disease | Chest indrawing, stridor, danger signs | Urgent referral + first dose antibiotic |
| Pneumonia | Fast breathing (≥50/min in 2-11 months; ≥40/min in 1-5 yrs) | Oral amoxicillin (pediatric formulation), home care |
| No pneumonia: Cough or cold | No fast breathing, no chest indrawing | Soothe the throat, home care |
B. Diarrhea Classification:
| Classification | Signs |
|---|---|
| Severe dehydration | Lethargic, sunken eyes, skin pinch very slow, not able to drink |
| Some dehydration | Restless/irritable, sunken eyes, skin pinch slow, drinks eagerly |
| No dehydration | Not enough signs to classify above |
- Treatment: ORS + Zinc (zinc for 14 days reduces severity and prevents recurrence)
C. Malnutrition Classification:
- Severe acute malnutrition (SAM): MUAC <11.5cm, visible severe wasting, bilateral pitting edema
- Moderate acute malnutrition (MAM): MUAC 11.5-12.5cm
- Normal: MUAC ≥12.5cm
D. Fever (Malaria):
- Classification depends on malaria risk area, duration of fever, other signs
Newborn Specific Interventions (from CB-NCP component)
| Intervention | Details |
|---|---|
| Chlorhexidine application | 4% gel applied to umbilical cord stump for 7 days - prevents omphalitis/neonatal sepsis |
| Thermal protection | Skin-to-skin care (Kangaroo Mother Care), immediate drying, delayed bathing |
| Early initiation of breastfeeding | Within 1 hour of birth; exclusive breastfeeding for 6 months |
| Detection of birth asphyxia | Stimulation, positioning, referral |
| Low birth weight care | Counseling, KMC, referral if needed |
| Postnatal home visits | Day 1, Day 3, Day 7, Day 28 by trained health workers |
| Neonatal sepsis treatment | Antibiotics (injectable gentamicin + oral amoxicillin at community level) |
The CB-NCP pilot in Morang district showed treatment for neonatal sepsis rose from 3% to 75% - a dramatic demonstration of the programme's effectiveness.
Key Programme Monitoring Indicators (IMNCI Nepal)
| Indicator | Purpose |
|---|---|
| Incidence of pneumonia per 1,000 U5 children | Track disease burden |
| % of U5 children with pneumonia treated with antibiotics | Case management quality |
| % treated with Amoxicillin specifically | Drug appropriateness |
| Incidence of diarrhea per 1,000 U5 children | Track diarrheal burden |
| % of U5 with diarrhea treated with ORS | ORS use coverage |
| % of U5 with diarrhea treated with ORS + Zinc | Zinc co-treatment rate |
| % of newborns managed at HF/PHC/ORC | Newborn care coverage |
| % of newborns with LBW detected | Low birth weight identification |
| % of cases referred | Referral system functioning |
- 42,897 newborn cases registered and treated at health facilities
- Pneumonia incidence: 43 per 1,000 U5 children (national)
- % U5 pneumonia treated with antibiotics: 138% (>100% indicates over-diagnosis/referrals from community)
- Highest LBW proportion: Province 1 (20.39%); Lowest: Gandaki (6.4%)
Facility-Based IMNCI (FB-IMNCI)
| Condition | Facility-Level Management |
|---|---|
| Birth asphyxia | Neonatal resuscitation, NBCC |
| Neonatal sepsis | IV antibiotics, supportive care |
| Low birth weight | SNCU/NBSU, KMC |
| Pneumonia | IV/IM antibiotics, oxygen |
| Severe diarrhea | IV fluids (Ringer's lactate), ORS |
| Malaria | Appropriate antimalarials |
| Meningitis | IV antibiotics, LP if needed |
| Severe malnutrition | Therapeutic feeding (F-75, F-100), CMAM |
- NBCC (Newborn Care Corner) - at every delivery point
- NBSU (Newborn Stabilization Unit) - at CHC/FRU level
- SNCU (Special Newborn Care Unit) - at district hospital level
Pre-service IMNCI
- IMNCI content is included in the curriculum of health training institutions (nursing colleges, community medicine).
- Ensures that newly trained health professionals enter the workforce with IMNCI skills.
- Reduces dependency on in-service training alone.
IMNCI and the Health System in Nepal
| Level | IMNCI Role |
|---|---|
| Community (FCHV) | Health promotion, commodity distribution, danger sign recognition, referral |
| Health Post | Assessment, classification, treatment of sick newborns and children |
| PHC/ORC | Outreach services, postnatal visits, case management |
| PHCC/CHC | FB-IMNCI, NBSU, referral |
| District Hospital | SNCU, pediatric inpatient care |
| Zonal/Regional/Central | Specialist pediatric care, NICU |
Key Achievements of IMNCI in Nepal
- Care-seeking for diarrhea, pneumonia, and fever in under-5 children rose to or nearly to 50% by 2014
- IMCI implemented in all 75 districts by 2009
- CB-NCP pilot in Morang: neonatal sepsis treatment 3% → 75%
- Nepal was among the first countries to formally add neonatal care to IMCI
- Significant contribution to Nepal's reduction in Under-5 Mortality Rate (U5MR): from 162/1000 (1990) to <40/1000 (2020s)
- Nepal achieved MDG4 (2/3 reduction in child mortality) largely credited to CB-IMCI/IMNCI
Challenges and Constraints
| Challenge | Details |
|---|---|
| FCHV overburdening | FCHVs carry multiple programmes; quality may suffer |
| Training quality | Standardization of training across 75+ districts is difficult |
| Supply chain gaps | Stockouts of zinc, ORS, amoxicillin, chlorhexidine at peripheral levels |
| Terai-specific issues | Lower coverage, geographic challenges in southern plains |
| Remote areas | Geography makes supervision, referral, and supply difficult |
| Post-ODF sustainability | Maintaining IMNCI programme activity post-declaration challenges |
| Private sector gap | Majority of sick children seen at private facilities not following IMNCI protocols |
| Data quality | Incomplete and sometimes inflated reporting at health facility level |
Summary at a Glance
| Feature | Details |
|---|---|
| Full form | Community-Based Integrated Management of Neonatal and Childhood Illnesses |
| Established | CB-IMNCI formed October 14, 2014 (merger of CB-IMCI + CB-NCP) |
| Managing body | Child Health Division, DoHS, MoHP, Nepal |
| Age target | 0-28 days (newborn), 29 days - 2 months (young infant), 2 months - 5 years (child) |
| Diseases covered | Pneumonia, diarrhea, malaria, measles, malnutrition, neonatal sepsis, birth asphyxia, LBW, hypothermia, jaundice |
| Key cadre | FCHVs (community), health post workers, nurses, doctors |
| Key commodities | Amoxicillin, ORS, zinc, chlorhexidine 4%, iron, Vitamin A |
| Three components | Case management + Health system strengthening + Community/family practices |
| Monitoring | HMIS monthly reporting; DoHS Annual Report |
| Impact | Major contributor to Nepal achieving MDG4 (child mortality reduction) |
IMNCI GUIDELINES FOR DIARRHOEA
IMNCI guidelines diarrhea classification assessment treatment ORS zinc plan A B C WHO
https://cdn.who.int/media/docs/default-source/2021-dha-docs/…
IMNCI Guidelines for Diarrhoea
Overview
The IMNCI algorithm asks: "Does the child have diarrhoea?" If YES → Classify for DEHYDRATION + Check if diarrhoea ≥14 days + Check if blood in stool
Step 1: ASSESSMENT - What to Ask and Look For
A. ASK:
- How long has the child had diarrhoea? (to detect persistent diarrhoea ≥14 days)
- Is there blood in the stool? (to detect dysentery)
B. LOOK AND FEEL (Four Key Signs):
| Sign | How to Check | What to Look For |
|---|---|---|
| 1. General condition | Observe the child | Lethargic/unconscious? OR Restless/irritable? |
| 2. Eyes | Look at eyes | Sunken eyes? |
| 3. Ability to drink | Offer water/ORS | Not able to drink / drinks poorly? OR Drinks eagerly, thirsty? |
| 4. Skin pinch | Pinch skin of abdomen, release | Goes back very slowly (>2 seconds)? OR Slowly? OR Normally (goes back immediately)? |
These four signs are used to classify dehydration status - the most critical step.
Step 2: CLASSIFICATION of Diarrhoea
CLASSIFICATION 1: For DEHYDRATION
🔴 SEVERE DEHYDRATION (Pink - most urgent)
| Signs Required | 2 or more of the following: |
|---|---|
| General condition | Lethargic or unconscious |
| Eyes | Sunken eyes |
| Drinking | Not able to drink or drinking poorly |
| Skin pinch | Goes back very slowly (>2 seconds) |
🟡 SOME DEHYDRATION (Yellow)
| Signs Required | 2 or more of the following: |
|---|---|
| General condition | Restless, irritable |
| Eyes | Sunken eyes |
| Drinking | Drinks eagerly, thirsty |
| Skin pinch | Goes back slowly |
🟢 NO DEHYDRATION (Green)
| Signs Required |
|---|
| Not enough signs to classify as Some or Severe Dehydration |
CLASSIFICATION 2: For Duration (Persistent Diarrhoea)
Checked in addition to dehydration classification when diarrhoea lasts 14 days or more
| Signs | Classification | Treatment |
|---|---|---|
| Diarrhoea ≥14 days + dehydration present | 🔴 SEVERE PERSISTENT DIARRHOEA | Treat dehydration first → Refer to hospital |
| Diarrhoea ≥14 days + no dehydration | 🟡 PERSISTENT DIARRHOEA | Counsel on feeding + multivitamins + zinc for 14 days + follow-up in 5 days |
CLASSIFICATION 3: For Blood in Stool (Dysentery)
| Signs | Classification | Treatment |
|---|---|---|
| Blood in the stool | 🟡 DYSENTERY | Ciprofloxacin for 3 days + follow-up in 3 days |
Step 3: TREATMENT PLANS
🟢 PLAN A - Treat Diarrhoea at Home (No Dehydration)
Rule 1: Give EXTRA FLUID
- Breastfed infants: Breastfeed more frequently and longer at each feed
- If exclusively breastfed: Give ORS in addition to breastmilk
- If not exclusively breastfed: Give ORS solution OR food-based fluids (soup, rice water, yoghurt drinks) OR clean water
| Age | Amount of ORS after each stool |
|---|---|
| < 2 years | 50-100 mL (a quarter to half a large cup) |
| 2-10 years | 100-200 mL (half to one large cup) |
| ≥ 10 years | As much as the child wants |
Rule 2: Give ZINC Supplements
- <6 months: 10 mg zinc/day for 14 days
- ≥6 months: 20 mg zinc/day for 14 days
- Zinc reduces duration and severity of diarrhea AND prevents recurrence over next 2-3 months
- Can be given at the same time as ORS - they do not interfere with each other
Rule 3: CONTINUE FEEDING
- Do not stop food; continue age-appropriate diet
- Continue breastfeeding throughout
- Resume normal diet as soon as appetite returns
- Avoid high-sugar drinks, commercial juices
Rule 4: WHEN TO RETURN immediately
- Passes many stools (increasing frequency)
- Is very thirsty (worsening dehydration)
- Has sunken eyes (dehydration sign)
- Cannot drink or breastfeed
- Gets worse overall
- Develops fever
- Has blood in stool
🟡 PLAN B - Treat SOME Dehydration with ORS (at Health Facility)
Amount of ORS for 4-hour rehydration:
| Age (approximate weight) | Amount of ORS in 4 hours |
|---|---|
| 2-4 months (3-6 kg) | 200-400 mL |
| 4-12 months (6-10 kg) | 400-700 mL |
| 12 months-2 years (10-12 kg) | 700-900 mL |
| 2-5 years (12-19 kg) | 900-1400 mL |
How to give ORS:
- Give by teaspoon or small cup - small, frequent sips
- If child vomits: wait 10 minutes then give more slowly
- Continue breastfeeding
After 4 hours:
- Reassess the child using the classification chart
- Choose the appropriate next plan (A, B, or C)
- If no dehydration: go to Plan A + give zinc for 14 days
- If some dehydration persists: repeat Plan B for another 4 hours
- If severe dehydration develops: start Plan C
Additional actions in Plan B:
- Give zinc supplements for 14 days
- Advise mother when to return immediately
- Follow-up in 5 days if not improving
Important: If mother must leave before completing 4-hour rehydration - teach her to make ORS at home, give enough ORS packets for completion + 2 extra packets, and teach the 4 Rules of Home Treatment.
🔴 PLAN C - Treat SEVERE Dehydration Quickly (Urgent)
If IV can be given (preferred):
| Age | Amount | Rate |
|---|---|---|
| Infant (<12 months) | 100 mL/kg | First 30 mL/kg in 1 hour; then 70 mL/kg in 5 hours |
| Child (≥12 months) | 100 mL/kg | First 30 mL/kg in 30 minutes; then 70 mL/kg in 2.5 hours |
- If not improving (still severe dehydration after 3 hours): send for IV therapy
- After 6 hours (infant) or 3 hours (child): reassess and reclassify → choose Plan A, B, or C
If IV cannot be given:
- If child can drink: Give ORS by nasogastric tube or mouth: 20 mL/kg/hour for 6 hours (total 120 mL/kg)
- If child cannot drink and no IV available: Refer URGENTLY to hospital with mother giving ORS sips on the way
Additional actions in Plan C:
- If child is ≥2 years AND cholera is present in the area: give antibiotic for cholera
- Advise mother to continue breastfeeding
- Once rehydrated, give zinc for 14 days
- If child has another severe classification: refer urgently to hospital
Summary Table: Complete IMNCI Diarrhoea Classification and Treatment
| Classification | Color | Key Signs | Treatment |
|---|---|---|---|
| SEVERE DEHYDRATION | 🔴 Pink | 2 of: Lethargic/unconscious; sunken eyes; not able to drink/drinking poorly; skin pinch very slowly (>2s) | PLAN C (IV fluids) or urgent referral |
| SOME DEHYDRATION | 🟡 Yellow | 2 of: Restless/irritable; sunken eyes; drinks eagerly/thirsty; skin pinch slowly | PLAN B (ORS 75mL/kg over 4 hrs) + zinc |
| NO DEHYDRATION | 🟢 Green | Not enough signs for above | PLAN A (ORS at home + zinc) |
| SEVERE PERSISTENT DIARRHOEA | 🔴 Pink | Diarrhoea ≥14 days + dehydration present | Treat dehydration → Refer to hospital |
| PERSISTENT DIARRHOEA | 🟡 Yellow | Diarrhoea ≥14 days + no dehydration | Feeding counseling + multivitamins + zinc 14 days + F/U 5 days |
| DYSENTERY | 🟡 Yellow | Blood in stool | Ciprofloxacin for 3 days + F/U 3 days |
Zinc Supplementation - Key Points
| Feature | Detail |
|---|---|
| Dose | <6 months: 10 mg/day; ≥6 months: 20 mg/day |
| Duration | 14 days (complete the course even after diarrhoea stops) |
| When to give | With ALL cases of diarrhoea (Plan A, B, and after Plan C) |
| Benefit | Reduces duration by ~25%; reduces severity; prevents future episodes for 2-3 months |
| Form | Tablet (dispersible in small amount of water/breastmilk) or syrup |
| Can combine with ORS | Yes - give at the same time |
Diarrhoea in Young Infants (0-2 months) - Special Considerations
| Sign | What to Look For |
|---|---|
| General condition | Movements - moves on own? Only when stimulated? Does not move at all? Restless/irritable? |
| Eyes | Sunken eyes |
| Skin pinch | Very slowly (>2s) or slowly? |
When to Refer (Danger Signs)
- Has severe dehydration and IV cannot be given locally
- Has severe persistent diarrhoea
- Develops deterioration despite Plan B treatment
- Has a concomitant severe classification (e.g., severe pneumonia + diarrhoea)
- Is very young (<2 months) with severe diarrhoea
Key Counselling Messages for Mothers
- Give more fluid than usual during diarrhoea
- Give zinc every day for 14 days even after diarrhoea stops
- Continue breastfeeding and normal food
- Do NOT give anti-diarrhoeals, antibiotics (unless dysentery), or anti-emetics routinely
- Know the danger signs to return immediately
- Wash hands with soap after defecation and before feeding child
- Use safe water for drinking and preparing ORS
In one sentence: IMNCI diarrhoea management follows assess → classify (dehydration + duration + blood) → treat (Plan A/B/C + zinc always for 14 days + feeding continuation) → follow up - with referral for severe dehydration and severe persistent diarrhoea.
- Park's Textbook of Preventive and Social Medicine (IMNCI charts, pp. 695-697)
- WHO Diarrhoea Treatment Guidelines (WHO/UNICEF)
GAPPD
GAPPD Global Action Plan Prevention Control Pneumonia Diarrhoea WHO UNICEF 2013 features targets
https://results.org.uk/wp-content/uploads/2013/04/6-Final-FA…
GAPPD protect prevent treat interventions list breastfeeding vaccines ORS zinc WASH antibiotics oxygen
GAPPD - Integrated Global Action Plan for the Prevention and Control of Pneumonia and Diarrhoea
1. Definition and Background
| Feature | Detail |
|---|---|
| Launched by | WHO and UNICEF |
| Year | 2013 (April 12, Geneva/Washington DC) |
| Full title | "Ending Preventable Child Deaths from Pneumonia and Diarrhoea by 2025" |
| Target population | Children under 5 years of age |
| First of its kind | First global framework to set national pneumonia and diarrhoea mortality targets |
Rationale for integration:
- Pneumonia and diarrhoea together cause ~24% of all deaths in children under 5
- Both diseases share common risk factors (malnutrition, unsafe water, poor hygiene, inadequate immunization)
- Many interventions overlap - addressing them together is more efficient and effective than single-disease approaches
- Prior single-disease approaches had failed to reduce the combined burden adequately
2. Core Framework: PROTECT - PREVENT - TREAT
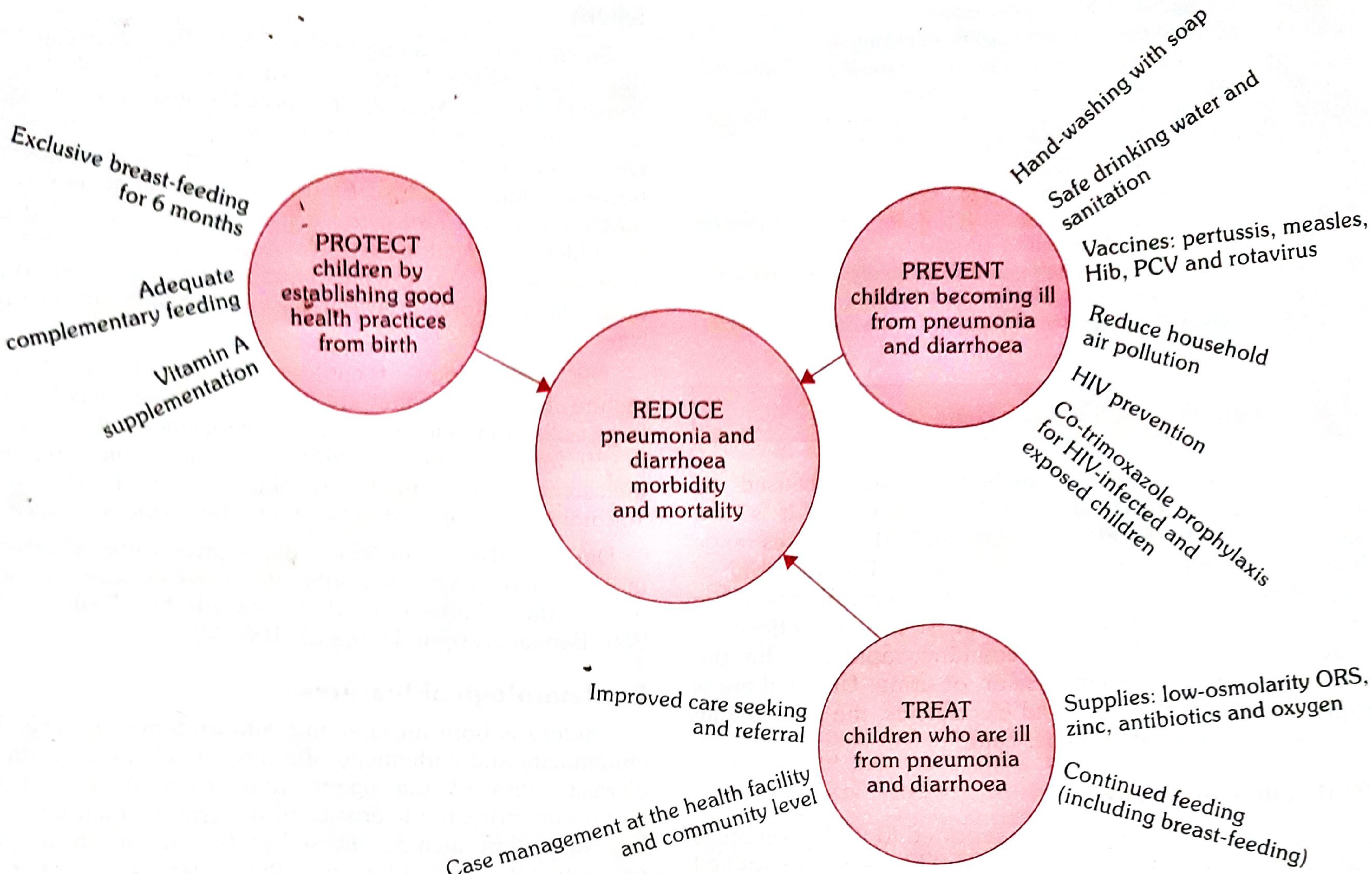
🔵 PILLAR 1: PROTECT
| Intervention | Rationale |
|---|---|
| Exclusive breastfeeding for 6 months | Passive immunity, reduces exposure to contaminated food/water |
| Adequate complementary feeding | Prevents malnutrition, maintains immune function |
| Vitamin A supplementation | Reduces severity of diarrhoea and pneumonia in deficient children |
PROTECT focuses on nutrition and nurturing practices that build a child's innate defenses from birth.
🔵 PILLAR 2: PREVENT
| Intervention | Disease Targeted |
|---|---|
| Vaccines: pertussis, measles, Hib (Haemophilus influenzae type b), PCV (pneumococcal), rotavirus | Pneumonia + Diarrhoea |
| Handwashing with soap | Both |
| Safe drinking water and sanitation | Primarily diarrhoea |
| Reduce household air pollution | Primarily pneumonia |
| HIV prevention | Both (HIV increases susceptibility) |
| Cotrimoxazole prophylaxis for HIV-infected and exposed children | Pneumonia (PCP pneumonia, other infections) |
PREVENT addresses environmental and biological exposure to pathogens.
🔵 PILLAR 3: TREAT
| Intervention | Disease Targeted |
|---|---|
| Improved care-seeking and referral | Both |
| Case management at health facility AND community level (IMCI/IMNCI) | Both |
| Supplies: Low-osmolarity ORS + zinc | Diarrhoea |
| Supplies: Antibiotics | Pneumonia (amoxicillin), Dysentery |
| Supplies: Oxygen | Severe pneumonia |
| Continued feeding (including breastfeeding) | Both |
TREAT focuses on timely access to proven treatments at both community and facility levels.
3. GAPPD Goals for 2025
| Goal | Target |
|---|---|
| Pneumonia mortality | Reduce to <3 per 1,000 live births in children <5 years |
| Diarrhoea mortality | Reduce to <1 per 1,000 live births in children <5 years |
| Severe pneumonia incidence | Reduce by 75% compared to 2010 levels |
| Severe diarrhoea incidence | Reduce by 75% compared to 2010 levels |
| Child stunting | Reduce global prevalence by 40% compared to 2010 levels |
4. GAPPD Coverage Targets
By end of 2025:
| Coverage Target | Level |
|---|---|
| Full-dose coverage of each relevant vaccine | 90% (≥80% in every district) |
| Access to appropriate pneumonia and diarrhoea case management | 90% (≥80% in every district) |
| Exclusive breastfeeding in first 6 months | At least 50% |
| Paediatric HIV | Virtual elimination |
By end of 2030:
| Target |
|---|
| Universal access to basic drinking water in health care facilities and homes |
| Universal access to adequate sanitation in health care facilities by 2030, and in homes by 2040 |
| Universal access to handwashing facilities (water + soap) in health care facilities and homes |
| Universal access to clean and safe energy technologies in health care facilities and homes |
5. Key Features and Principles
- Integrated approach - Addresses both diseases simultaneously; avoids duplication; maximizes synergies
- Evidence-based - All interventions are time-tested and proven; no new technology required
- Equity focus - Stresses reaching the poorest and most vulnerable; reducing inequalities
- Country-led - Countries analyse local data, set priorities, and monitor progress
- Multi-sectoral - Governments, health workers, CHWs, civil society, private sector, NGOs, donors all have roles
- Linkage to MDGs/SDGs - Originally aligned with MDG4 (child mortality); now extended toward SDGs (2030)
- First-ever mortality targets - National targets for pneumonia (<3/1000) and diarrhoea (<1/1000) deaths
- Community-level delivery - Community health workers are central (parallels IMNCI's CB component)
- Demand + supply side - Addresses both supply of services and demand/care-seeking behaviors
6. GAPPD in Relation to Other Programmes
| Programme | Relationship to GAPPD |
|---|---|
| IMNCI | TREAT pillar delivery mechanism; case management at community and facility level |
| EPI/Immunization | PREVENT pillar (vaccines for measles, Hib, PCV, pertussis, rotavirus) |
| WASH | PREVENT pillar (safe water, sanitation, handwashing) |
| IMAM/Nutrition | PROTECT pillar (breastfeeding, complementary feeding, Vitamin A, zinc supplementation) |
| PMTCT/HIV programme | PREVENT pillar (virtual elimination of paediatric HIV, cotrimoxazole prophylaxis) |
7. Progress and Current Status
- Since 2013, child pneumonia and diarrhoea deaths fell by ~27%
- However, 30 LMICs with the highest numbers of child pneumonia deaths will not achieve the GAPPD 2025 targets by 2030
- 80% of all child pneumonia deaths occur in just 30 countries; 50% in Nigeria, India, Pakistan, Ethiopia, and Niger alone
- Advocates are calling for: updating GAPPD targets to 2030, aligning with SDGs, strengthening targets for risk factors (wasting, LBW, air pollution), and improving access to pulse oximetry/oxygen
Summary (One Sentence)
- Park's Textbook of Preventive and Social Medicine, pp. 189-194
- WHO/UNICEF. Ending Preventable Child Deaths from Pneumonia and Diarrhoea by 2025: GAPPD. Geneva: WHO; 2013.