Write me 20 marks short note on acute pain management based on chapter 35 of book tintinalli emergency medicine 11 th edition
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive content from Chapter 35. I have enough material to write a thorough 20-mark short note. Let me now compose the answer based on everything captured from the textbook.
Acute Pain Management
Short Note - 20 Marks
Based on Chapter 35, Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 11th Edition
Introduction
Pain is the most common presenting symptom in the emergency department (ED), accounting for 70-80% of all patient presentations. Despite advances in pain research, oligoanalgesia - the systematic undertreatment of pain - remains a significant problem. Vulnerable groups including ethnic minorities, the elderly, children, and cognitively impaired patients are at greatest risk. While concerns over opioid misuse are legitimate (initial opioid prescriptions have been associated with persistent use months later), appropriate treatment of severe acute pain must not be withheld.
Pathophysiology
Pain is the physiologic response to a noxious stimulus, while suffering is its expression - modified by cognitive, behavioral, and sociocultural factors. Individual pain experience varies with medical history, emotional state, culture, and environment. Fear and anxiety worsen pain; concentrated focus on another task can suppress it entirely.
The peripheral nervous system - nociceptors, C-fibers (slow, aching, burning), and A-delta fibers (fast, sharp, well-localized) - initiates somatic pain sensation. These afferents synapse in the dorsal horn of the spinal cord, where the pain signal is modulated before ascending to the brain. The brain then integrates the signal and produces the subjective experience of pain.
Key pain types include:
- Nociceptive pain - from tissue damage; responds well to NSAIDs and opioids
- Neuropathic pain - from nerve injury; poorly responsive to opioids; managed with tricyclics, anticonvulsants, or SNRIs
- Visceral pain - poorly localized, often with associated autonomic symptoms
Self-reporting is the gold standard for quantifying pain severity, as no external observer can fully appreciate the modifying variables that shape an individual's experience.
Pain Assessment
Accurate assessment is the foundation of pain management. Key principles:
- Pain should be assessed at triage and reassessed after each intervention
- No single scale is universally superior; the choice should suit the patient
Pain Scales (Table 35-2)
| Scale | Method | Notes |
|---|---|---|
| Visual Analog Scale (VAS) | 100-mm line; patient marks intensity | Minimum clinically significant change = 13 mm; acceptable relief = 30 mm decrease |
| Numeric Rating Scale (NRS) | 0-10 self-report with descriptors | Most commonly used; can be adapted for visual/speech difficulties |
| Verbal Quantitative Scale | 0-10 without descriptors | Easy to administer |
| Adjective Rating Scale | Ordered descriptors (none to worst) | Easy; allows marks between labels |
| 5-Point Global Scale | 0-4 patient rating | A 1-point decrease = large change |
Pain score alone does not reliably predict the dose of analgesia required - it has only a moderate relationship to analgesic need.
Special Populations (Pain Scale Performance)
- Children: Behavioral or observational scales (e.g., FLACC, FACES scale) are used for preverbal patients
- Elderly: Cognitive impairment may limit verbal reporting; behavioral cues and caregiver input become important
- Cognitively impaired: Observer-based scales required
Pharmacologic Acute Pain Treatment
The key to effective pharmacologic management is selecting an agent appropriate for pain intensity, onset, safety, route, and efficacy.
Approach to Initial Analgesic Selection
The classic "tiered (stepwise) approach" - starting with weak agents regardless of pain severity and escalating - is now considered suboptimal as it prolongs suffering. The preferred approach is to match analgesic potency to pain intensity from the outset:
- Mild pain: Acetaminophen or NSAIDs
- Moderate pain: NSAIDs ± weak opioids; consider combinations
- Severe pain: Systemic opioids; regional/local anesthesia as adjunct
Whenever possible, a mechanistic approach is preferred over opioid symptom masking. Example: in migraine, serotonin agonists (triptans) or dopamine antagonists (phenothiazines, metoclopramide) target the mechanism rather than masking pain.
1. Non-Opioid Analgesics
Acetaminophen (Paracetamol)
- Mechanism: Inhibits central prostaglandin synthesis; may modulate the endocannabinoid system
- Effective for mild-moderate pain; useful as part of multimodal regimens
- IV formulation (1 g) provides faster onset and is useful when oral route unavailable
- Safe in renal impairment; maximum dose 4 g/day (reduced in liver disease, alcoholism, malnutrition)
NSAIDs (Non-Steroidal Anti-Inflammatory Drugs)
- Mechanism: Inhibit COX-1 and COX-2 enzymes → reduce prostaglandin synthesis → peripheral and central anti-inflammatory and analgesic effects
- Particularly effective for:
- Musculoskeletal pain
- Renal colic and biliary colic (smooth muscle spasm)
- Dysmenorrhea
- Dental and soft tissue inflammation
- IV ketorolac (15-30 mg) is widely used in the ED for moderate-severe pain; comparable to opioids for renal colic
- Caution: renal impairment, GI bleeding risk, cardiovascular events, platelet inhibition
- COX-2 selective agents (celecoxib) spare GI effects but carry cardiovascular risk
Nitrous Oxide (N₂O)
- 50% N₂O in O₂ (Entonox) provides rapid-onset, short-duration analgesia and anxiolysis
- Useful for procedural pain and dressing changes
- Onset: ~2-3 minutes; wears off rapidly on discontinuation
- Avoid in: pneumothorax, bowel obstruction, middle ear problems
2. Opioid Analgesics
Opioids act on mu, kappa, and delta receptors in the CNS and periphery to reduce pain transmission and perception.
Indications: Severe nociceptive pain (trauma, ischemia, post-procedural). Opioids have little to no role in acute neuropathic pain or chronic pain flares.
Common Opioids in the ED
| Drug | Route | Dose | Onset | Notes |
|---|---|---|---|---|
| Morphine | IV/IM | 0.1 mg/kg; titrate 2-4 mg IV q5-10 min | 5 min (IV) | Gold standard; histamine release; caution in renal failure |
| Fentanyl | IV/IN | 1-2 mcg/kg IV; 2 mcg/kg intranasal | 1-2 min (IV) | Short-acting; preferred in hemodynamic instability; intranasal useful in children |
| Hydromorphone | IV | 0.2-0.4 mg IV | 5 min | More potent than morphine (5:1); useful in morphine-intolerant patients |
| Oxycodone | PO | 5-10 mg q4-6h | 30-60 min | Oral use; moderate-severe pain |
| Codeine | PO | 30-60 mg | 30-60 min | Prodrug (CYP2D6); variable efficacy; not recommended in children |
| Tramadol | PO/IV | 50-100 mg | 30 min | Weak mu-agonist + SNRI; avoid in seizure-prone patients |
Opioid Dosing Principles
- IV titration is safest - small incremental doses with reassessment
- Weight-based dosing for children
- Reassess at expected time to peak effect (morphine IV: 15-20 min)
- Avoid IM route when IV access available - variable absorption
- Caution in elderly: reduce starting dose by 25-50%
Opioid Side Effects
- Nausea/vomiting: give antiemetic concurrently
- Respiratory depression: rare with proper titration; treat with naloxone 0.4-2 mg IV
- Constipation, urinary retention, pruritus
- Hypotension (especially in hypovolemic patients)
Patient-Controlled Analgesia (PCA)
- Allows patient to self-administer small incremental IV opioid doses within preset limits
- Reduces oligoanalgesia; improves satisfaction and reduces nurse-administered variability
3. Adjuvant and Non-Traditional Analgesics
Ketamine (Sub-dissociative)
- Dose: 0.1-0.5 mg/kg IV (sub-dissociative)
- NMDA receptor antagonist; effective for opioid-refractory pain, neuropathic pain, and procedural analgesia
- Can reduce total opioid consumption ("opioid-sparing")
- Side effects: dysphoria, hallucinations (less common at low doses); give midazolam 1-2 mg to reduce emergence reactions if needed
Nitrous Oxide
(Covered above)
Alpha-2 Agonists (e.g., dexmedetomidine, clonidine)
- Analgesic and sedative properties
- Used as opioid adjuncts; useful in procedural sedation
Anticonvulsants (Gabapentin, Pregabalin)
- For neuropathic pain components; reduce central sensitization
- Increasingly used in multimodal perioperative analgesia
Antidepressants (TCAs, SNRIs)
- Neuropathic pain management; not for acute severe pain
4. Regional and Local Anesthesia
When possible, regional anesthesia is an excellent opioid-sparing option (see Chapter 36).
- Local infiltration: Lidocaine, bupivacaine for wound repair, minor procedures
- Peripheral nerve blocks: Femoral, fascia iliaca, ulnar, radial, digital blocks - especially effective with ultrasound guidance
- Topical anesthesia: EMLA cream, LET (lidocaine-epinephrine-tetracaine) gel for wound/venipuncture in children
Ultrasound guidance has significantly improved the safety and success of regional nerve blocks in the ED.
Special Pain Situations
Abdominal Pain
- Withholding analgesia to preserve diagnostic findings is no longer supported by evidence - adequate analgesia does not impair abdominal exam accuracy
- NSAIDs and opioids are both appropriate depending on severity and etiology
- Renal colic: IV ketorolac is first-line; IV opioid if inadequate
Headache/Migraine
- Mechanistic approach preferred: IV prochlorperazine 10 mg, metoclopramide 10 mg, or sumatriptan
- IV dexamethasone 8-10 mg reduces recurrence
- Opioids are not first-line for migraine - they worsen medication overuse headache and are less effective
Sickle Cell Pain Crisis
- Often undertreated; patients have high opioid tolerance from chronic exposure
- Aggressive IV opioid titration required; consider PCA
- NSAIDs and IV fluids are useful adjuncts
Elderly Patients
- Start with lower doses and titrate slowly
- Beware renal impairment affecting NSAID and morphine-6-glucuronide clearance
- NSAIDs: use with caution; consider acetaminophen first
- Risk of falls, delirium with opioids and sedatives
Pediatric Patients
- Weight-based dosing essential
- Intranasal fentanyl (2 mcg/kg) is a well-tolerated alternative to IV
- Oral sucrose and non-pharmacologic methods for neonates
- Avoid codeine in children (CYP2D6 variability risk)
Multimodal Analgesia
Using agents with different mechanisms in combination:
- Reduces individual drug doses and side effects
- Provides additive or synergistic analgesia
- Example: Acetaminophen + NSAID + low-dose opioid + regional block
This approach is now the standard of care for managing moderate-severe acute pain.
Non-Pharmacologic Methods
Not to be underestimated:
- Verbal reassurance and information reduces anxiety and can reduce analgesic requirements
- Immobilization and splinting for fractures
- Ice/heat application
- Positioning and elevation
- Distraction and relaxation techniques (especially in children)
- Anxiolytics (e.g., midazolam) when anxiety amplifies pain and verbal reassurance is insufficient
Discharge Analgesia and Opioid Stewardship
- The minimum effective dose of the least potent opioid should be prescribed at discharge
- Short courses (3-7 days) with clear instructions
- Non-opioid regimens should be maximized before opioids are added
- Patient education: storage, disposal, no sharing
- Screening tools (AUDIT, DAST) can identify at-risk patients before prescribing
Summary
Acute pain management in the ED requires:
- Accurate, repeated assessment using appropriate scales
- Matching analgesic potency to pain severity from the outset (not tiered escalation)
- Multimodal analgesia - combining non-opioids, opioids when needed, and regional techniques
- Special attention to vulnerable populations (elderly, pediatric, cognitively impaired)
- Mechanistic approaches for specific pain syndromes (migraine, renal colic)
- Responsible opioid use with stewardship at discharge
- Non-pharmacologic adjuncts as part of holistic care
Oligoanalgesia must be actively combated - undertreating pain is harmful, but so is overprescribing opioids. The goal is individualized, effective, safe analgesia.
Source: Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 11th Edition - Chapter 35: Acute Pain Management (James Ducharme), pp. 270-280
Pain pathways
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have everything needed - comprehensive text from Harrison's, Ganong's, and Morgan & Mikhail's, plus three excellent diagrams. Here is the complete, well-illustrated note on pain pathways.
Pain Pathways
Sources: Harrison's Principles of Internal Medicine 22e, Ganong's Review of Medical Physiology 26e, Morgan & Mikhail's Clinical Anesthesiology 7e
Overview: The Four Key Processes
Pain signalling from injury to conscious experience involves four sequential processes:
- Transduction - noxious stimulus converted to electrical signal at the nociceptor
- Transmission - signal conducted along peripheral nerves to the spinal cord and brain
- Modulation - signal amplified or suppressed at dorsal horn and supraspinal levels
- Perception - conscious experience of pain at cortical level
1. PERIPHERAL MECHANISMS - Transduction
Primary Afferent Nociceptors
A peripheral nerve contains three types of axons: primary sensory afferents (cell bodies in the dorsal root ganglion), motor neurons, and sympathetic postganglionic neurons.
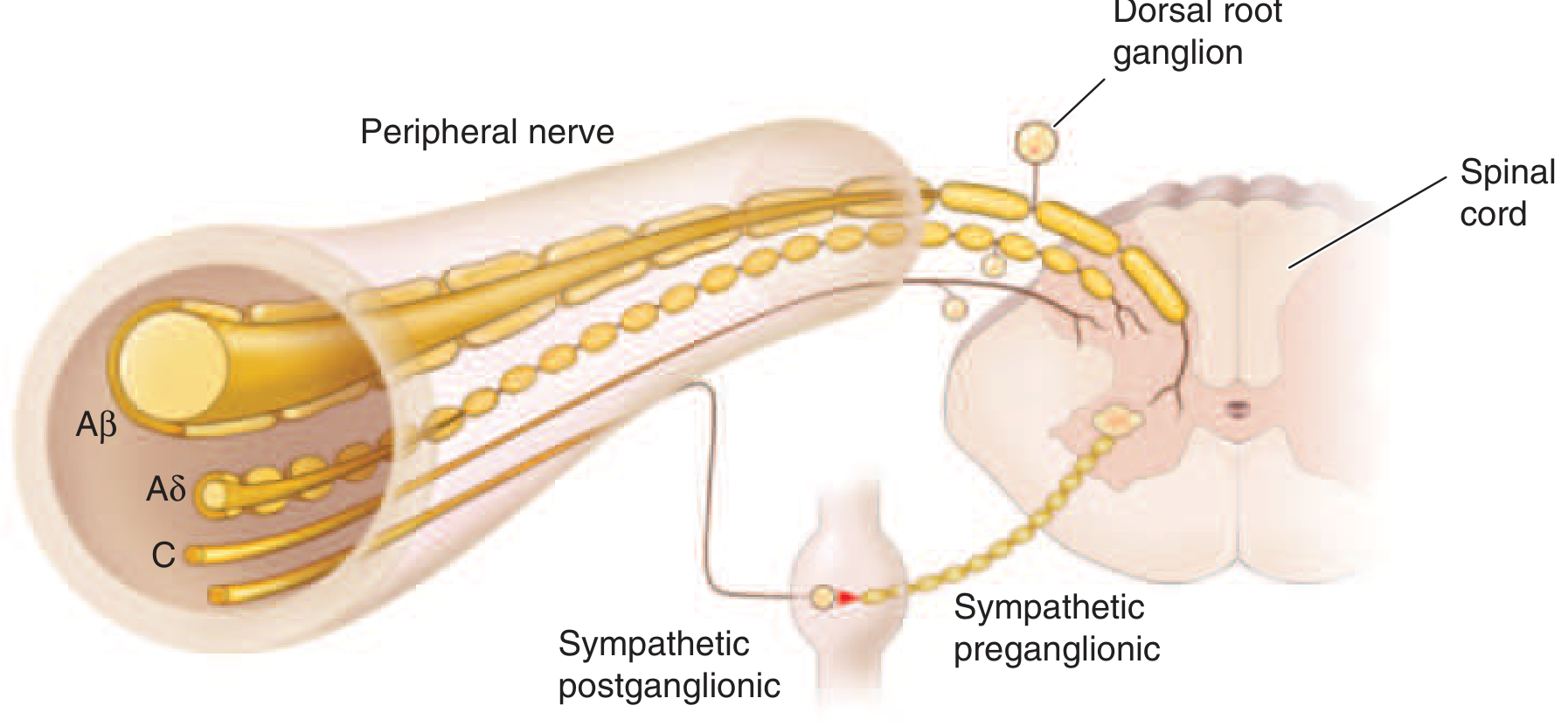
Primary afferents are classified into three types:
| Fiber | Diameter | Myelination | Conduction | Function |
|---|---|---|---|---|
| A-beta (Aβ) | Large | Heavily myelinated | Fast (30-70 m/s) | Light touch, proprioception - NOT normally painful |
| A-delta (Aδ) | Small | Thinly myelinated | Medium (5-30 m/s) | Fast, sharp, well-localized "first pain" |
| C fibers | Smallest | Unmyelinated | Slow (0.5-2 m/s) | Slow, burning, diffuse "second pain" |
Aδ and C fibers are the primary nociceptors - blocking them abolishes pain completely.
What Activates Nociceptors?
Individual nociceptors respond to multiple noxious stimuli:
- Intense heat or cold
- Intense mechanical distortion (pinch, crush)
- Acidic pH (H+ ions)
- Chemical irritants: ATP, serotonin, bradykinin (BK), histamine
- The TRPV1 receptor (vanilloid receptor) mediates heat and acid pain, and is the target of capsaicin
Peripheral Sensitization
After tissue injury or inflammation, nociceptor thresholds are lowered and firing frequency increased for all stimulus intensities. This is called peripheral sensitization.
Mediators responsible: bradykinin, prostaglandins (PGs), leukotrienes, nerve growth factor, H+ ions.
Mechanism: inflammatory mediators activate intracellular signal transduction in nociceptors → increased production and membrane insertion of ion channels → lowered threshold for mechanical, thermal, and chemical stimuli.
Nociceptor-Induced Neurogenic Inflammation
Activated nociceptors are not just passive messengers - they actively release substance P and CGRP from peripheral terminals, which:
- Cause vasodilation
- Trigger mast cell degranulation (histamine release)
- Attract leukocytes
- Increase inflammatory mediator production
This perpetuates and amplifies the inflammatory response ("neurogenic inflammation").
Silent Nociceptors
A large proportion of Aδ and C fibers innervating viscera are completely insensitive in normal, non-inflamed tissue. In the presence of inflammation, these silent nociceptors become activated by mechanical stimuli - explaining why diseased deep viscera can become a source of severe, debilitating pain.
2. CENTRAL MECHANISMS - Transmission
Dorsal Horn Entry
The axons of primary afferent nociceptors enter the spinal cord via the dorsal root and terminate in the dorsal horn of the spinal gray matter (Rexed laminae I, II, V).
Neurotransmitters released at the first synapse:
- Glutamate - rapid excitation of second-order dorsal horn neurons (AMPA receptors)
- Substance P and CGRP - slower, longer-lasting excitation (NK-1 receptors)
Spinothalamic Tract (STT) - The Main Ascending Pain Pathway
Second-order neurons in the dorsal horn decussate (cross) to the contralateral anterolateral white matter, forming the spinothalamic tract. This ascends through the lateral medulla, pons, and midbrain to reach the thalamus.
- Interruption of the STT produces permanent deficits in pain and temperature discrimination
- This is the anatomical basis of contralateral pain/temperature loss in Brown-Séquard syndrome and anterolateral cordotomy
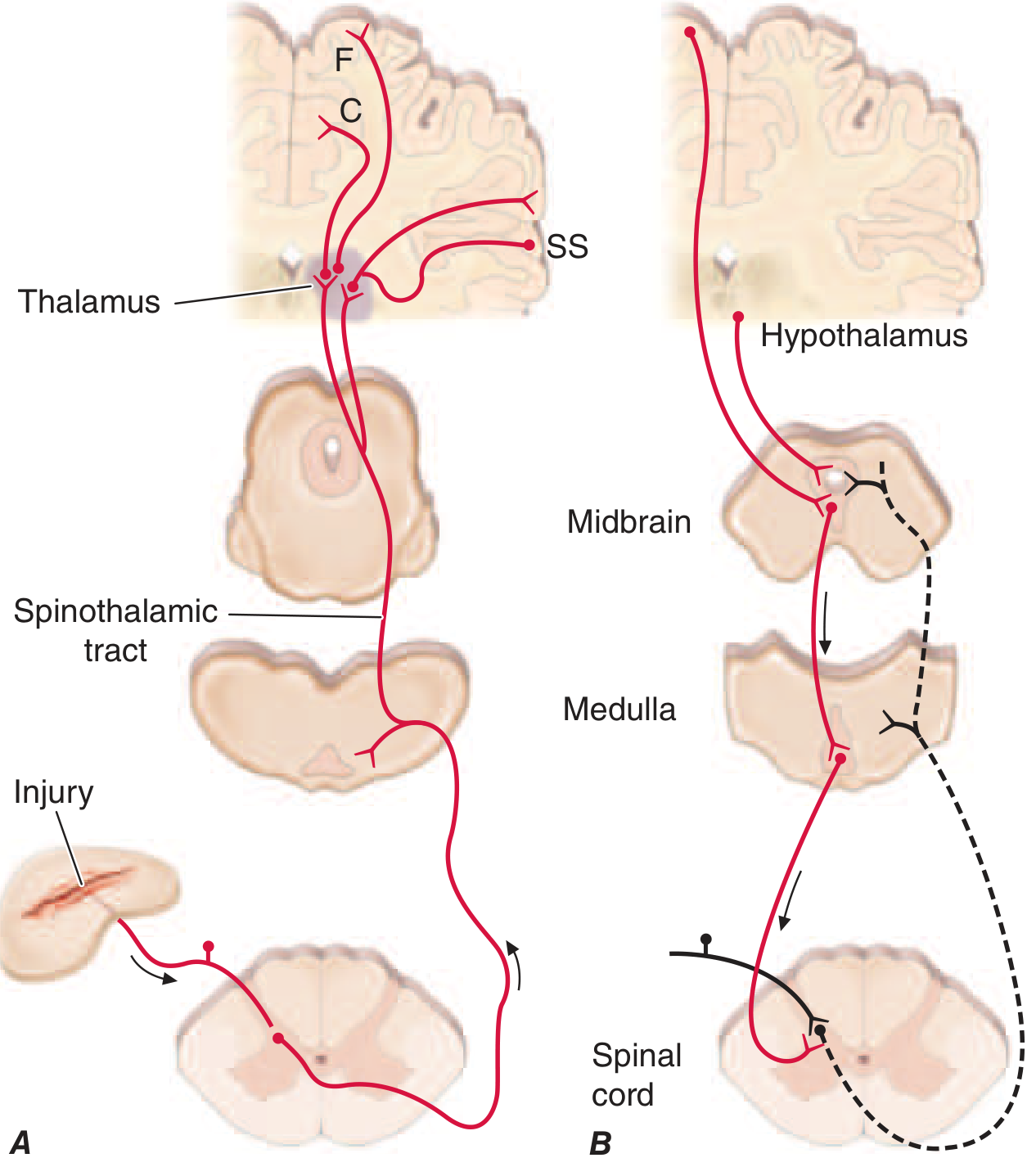
Thalamic Projections and Cortical Processing
STT axons diverge at the thalamus and project to multiple cortical areas, each subserving a different dimension of pain:
| Projection | Cortical Target | Function |
|---|---|---|
| Lateral thalamus | Somatosensory cortex (S1, S2) | Sensory-discriminative: location, intensity, quality of pain |
| Medial thalamus | Anterior cingulate cortex | Affective-motivational: suffering, unpleasantness, emotional response |
| Medial thalamus | Insular cortex | Autonomic responses, visceral pain, emotional integration |
This dual cortical processing explains why frontal lobe lesions can reduce the suffering component of pain while preserving the ability to localize it.
Referred Pain
The convergence-projection hypothesis explains referred pain: visceral afferents and somatic afferents converge on the same second-order dorsal horn neurons. The brain cannot distinguish the true source and "projects" the sensation to the somatic (skin) territory.
Examples:
- Cardiac ischemia → left arm/jaw pain (T1-T4 convergence)
- Diaphragmatic irritation → shoulder tip pain (C3-C4 dermatome)
- Appendicitis → periumbilical pain (T10) before right iliac fossa localization
3. PAIN MODULATION
Pain intensity is highly variable for similar injuries - reflecting active modulation of the signal at multiple levels.
Gate Control Theory (Dorsal Horn Level)
Proposed by Melzack & Wall (1965). Rubbing an injured area reduces pain because:
- Large Aβ fibers (activated by touch/rubbing) collateralize into the dorsal horn and activate inhibitory interneurons
- These interneurons suppress the relay of nociceptive input from Aδ and C fibers - effectively "closing the gate"
Clinical application: TENS (Transcutaneous Electrical Nerve Stimulation) uses electrodes to activate Aα and Aβ fibers near an injury to achieve pain relief via this gate mechanism.
Opioid Modulation at the Dorsal Horn
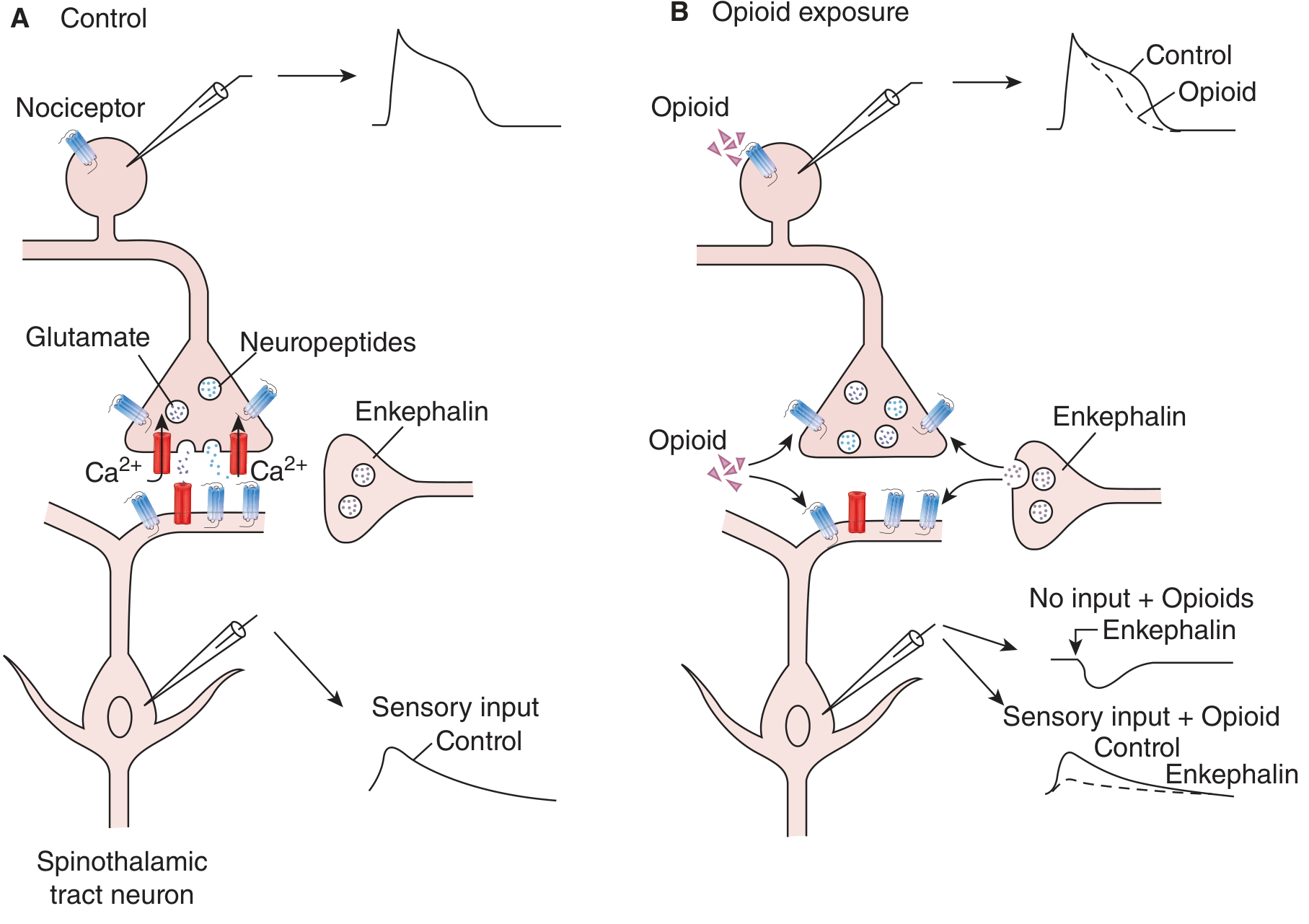
Endogenous opioid interneurons (containing enkephalin and dynorphin) are located in the superficial dorsal horn and modulate nociceptive transmission via:
- Presynaptic inhibition: opioid receptors on nociceptor terminals → decrease Ca²⁺ influx → less glutamate/substance P release
- Postsynaptic inhibition: opioid receptors on dorsal horn neurons → increase K⁺ conductance → hyperpolarization → reduced excitability
Exogenous opioids (morphine, fentanyl) mimic these endogenous mechanisms.
Descending Inhibitory System
The brain exerts powerful top-down control of pain via a descending modulatory pathway:
- Periaqueductal gray (PAG) in the midbrain - the central node; rich in opioid receptors
- Projects to rostroventromedial medulla (RVM) and locus coeruleus (LC)
- Descending axons reach the dorsal horn of the spinal cord
- Release serotonin (from RVM) and norepinephrine (from LC) to inhibit pain transmission
This pathway explains:
- Stress-induced analgesia (soldiers in battle unaware of injuries)
- Placebo analgesia (endogenous opioid release)
- How morphine, at supraspinal sites, activates this system to produce analgesia
Central Sensitization
When nociceptors generate prolonged activity (as in inflammation), dorsal horn neurons become hyperexcitable. Three mechanisms (Morgan & Mikhail):
- Wind-up: repetitive C-fiber stimulation causes progressive increase in action potential generation in wide dynamic range (WDR) neurons via NMDA receptor activation
- Receptor field expansion: dorsal horn neurons begin responding to inputs from previously subthreshold somatic areas
- Hyperexcitability of flexion reflexes
Central sensitization underlies:
- Allodynia - pain from normally non-painful stimuli (e.g., light touch on sunburned skin)
- Hyperalgesia - exaggerated pain from mildly painful stimuli
- Chronic pain states - where the central nervous system becomes the primary pain generator
Ketamine (NMDA antagonist) directly blocks this mechanism - the basis for its use in neuropathic and opioid-refractory pain.
4. PERCEPTION - Cortical Processing
Pain is both sensation and emotion. The subjective experience integrates:
- Sensory-discriminative dimension (somatosensory cortex): "where, how intense, what quality"
- Affective-motivational dimension (anterior cingulate cortex, insula): "how unpleasant, how distressing"
- Cognitive-evaluative dimension (prefrontal cortex): prior experience, expectations, context
Factors modulating perception:
- Fear and anxiety → amplify pain (via limbic connections)
- Focused distraction, stress, morphine → suppress pain (via PAG activation)
- Cultural beliefs, past pain history, emotional state → alter threshold and tolerance
Clinical Correlations
| Concept | Clinical Relevance |
|---|---|
| Aδ vs C fibers | Aδ blocked first by local anesthetics → sharp pain lost before dull ache |
| TRPV1 | Target for capsaicin patches in neuropathic pain |
| Gate control | Rationale for TENS, acupuncture, rubbing injuries |
| Descending inhibition | Mechanism of opioid supraspinal analgesia; antidepressants (SNRIs) potentiate NE/5HT inhibition |
| Wind-up / NMDA | Rationale for ketamine; explains opioid tolerance escalation |
| Referred pain | Explains cardiac, biliary, and renal colic referral patterns |
| Silent nociceptors | Explains visceral hypersensitivity in IBD, IBS, interstitial cystitis |
| Brown-Séquard | Contralateral STT loss → contralateral pain/temp loss below lesion |
Summary Diagram (Conceptual)
NOXIOUS STIMULUS
↓
[NOCICEPTOR - Transduction]
TRPV1, ion channels, BK/PG sensitization
↓
[PRIMARY AFFERENT - Transmission]
Aδ (fast, sharp) / C fibers (slow, burning)
Cell bodies in Dorsal Root Ganglion
↓
[DORSAL HORN - 1st Synapse]
Glutamate + Substance P / CGRP
Modulation: Gate control, Opioids, Enkephalin
↓
[SPINOTHALAMIC TRACT - Contralateral]
Crosses at cord level → Anterolateral column
Ascends: Medulla → Pons → Midbrain → Thalamus
↓
[THALAMUS - Relay]
Lateral → Somatosensory cortex (S1/S2)
Medial → Anterior cingulate + Insular cortex
↓
[CORTEX - Perception]
Discriminative + Affective dimensions
DESCENDING INHIBITION (top-down):
Cortex/Hypothalamus → PAG → RVM/LC → Dorsal Horn
(Serotonin + Norepinephrine suppression)
Sources: Harrison's Principles of Internal Medicine 22e, Ch. 14 (Pain: Pathophysiology and Management) | Ganong's Review of Medical Physiology 26e, Ch. 8-9 | Morgan & Mikhail's Clinical Anesthesiology 7e, Ch. Pain Management
Write me 20 marks short note on local anesthetic agents based on chapter 36 of book tintinalli emergency medicine 11 th edition
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have all the content I need from Chapter 36 of Tintinalli's to write a comprehensive 20-mark short note. Here it is:
Local Anesthetic Agents
Short Note - 20 Marks
Based on Chapter 36: Local and Regional Anesthesia, Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 11th Edition (Gibbs & Wu)
Introduction
Local anesthetics (LAs) are agents used to reduce pain from acute injuries or procedures performed in the ED. The most common routes of administration include topical, subdermal infiltration, and infiltration around peripheral nerves (regional anesthesia). Selecting the right agent requires understanding pharmacology, toxicity, and the clinical context of use.
Classification
Local anesthetics are divided into two structural classes based on the linkage between their aromatic ring and intermediate chain:
| Class | Bond | Metabolism | Examples |
|---|---|---|---|
| Esters | Ester bond | Hydrolyzed by plasma cholinesterases | Procaine, tetracaine, chloroprocaine, benzocaine |
| Amides | Amide bond | Metabolized by hepatic microsomal enzymes | Lidocaine, bupivacaine, ropivacaine, levobupivacaine, mepivacaine, prilocaine |
Memory aid: Amides have two "i"s in the name (lidocaine, bupivacaine, prilocaine).
Mechanism of Action
Local anesthetics work by reversibly blocking voltage-gated sodium (Na⁺) channels, preventing depolarization and inhibiting propagation of nerve impulses along the axon.
- The drug enters the axon in its unionized form and binds the inner face of the Na⁺ channel in its ionized form
- Blockade is use-dependent - rapidly firing nerves are blocked preferentially
- Nerve fibers are blocked in a specific sequence based on fiber size:
- Pain and temperature (small Aδ and C fibers) - blocked first
- Touch and deep pressure (larger fibers) - blocked second
- Motor function (largest Aα fibers) - blocked last
This differential blockade allows pain relief while preserving motor function at appropriate concentrations.
Pharmacology: Key Determinants
1. Onset of Action - Determined by pKa
- The pKa is the pH at which 50% of the drug is ionized and 50% is unionized
- The unionized (free base) form crosses lipid membranes to enter the nerve
- Lower pKa = more drug in unionized form at physiologic pH = faster onset
- Agents with lower pKa: mepivacaine, lidocaine, prilocaine (faster onset)
- Agents with higher pKa: bupivacaine (slower onset)
- The pH of LA solutions is acidic (3.3-6.8), which shifts drug toward ionized form - this explains the initial pain on injection and reduced efficacy in infected/acidic tissues
2. Duration of Action - Determined by Protein Binding
- Higher protein binding = longer receptor affinity = longer duration
- Bupivacaine, tetracaine, ropivacaine: high protein binding → long duration (2-8 hours)
- Lidocaine, prilocaine: medium binding → intermediate duration (1-2 hours)
- Procaine: low binding → short duration (15-45 minutes)
3. Potency - Determined by Lipid Solubility
- More lipophilic agents penetrate nerve membranes more easily → higher potency
- Bupivacaine: high lipid solubility → highly potent
- Procaine: low lipid solubility → low potency
Individual Agents (Table 36-2)
| Agent | Class | Onset | Duration (no epi) | Max Dose (mg/kg) | Notes |
|---|---|---|---|---|---|
| Lidocaine | Amide | Fast (<1 min) | 30-120 min | 4 (7 with epi) | Most commonly used; versatile |
| Bupivacaine | Amide | 2-10 min | 120-240 min | 3 (5 with epi) | Long-acting; high cardiotoxicity |
| Levobupivacaine | Amide | 10-20 min | >1000 min | 2 | L-enantiomer of bupivacaine; less cardiotoxic |
| Ropivacaine | Amide | 10-45 min | 120-350 min | 3 | Less cardiotoxic than bupivacaine; preferred for regional blocks |
| Mepivacaine | Amide | 3-20 min | 30-120 min | 4 | Rapid onset; no epinephrine needed |
| Prilocaine | Amide | 5-6 min | 30-120 min | 5 | Risk of methemoglobinemia |
| Procaine | Ester | 5 min | 15-90 min | 7 | Short-acting; high allergenic potential |
| Chloroprocaine | Ester | 5-6 min | 30-60 min | 8 | Fastest onset ester; low toxicity |
| Tetracaine | Ester | 7 min | 120-240 min | 1.5 | Long-acting; topical use (LET gel) |
Vasoconstrictors (Epinephrine)
Adding epinephrine (adrenaline) to LA solutions provides significant advantages:
- Causes local vasoconstriction → reduces systemic absorption → prolongs duration and increases maximum safe dose
- Provides a marker of intravascular injection (sudden tachycardia if injected IV)
- Achieves hemostasis at the injection site
- Standard concentration: 1:100,000 to 1:200,000 (5-10 micrograms/mL)
Absolute contraindications to epinephrine-containing LAs:
- End-arterial territories: digital blocks (fingers, toes), penis, nose, ear pinna
- Patients on MAO inhibitors or non-selective beta-blockers
- Known coronary artery disease or peripheral vascular disease (relative)
Note: The traditional teaching to avoid epinephrine in digital blocks has been challenged by evidence; however, most ED protocols still caution against it.
Topical Anesthetic Agents (Table 36-1)
Intact Skin
| Agent | Composition | Onset | Application |
|---|---|---|---|
| EMLA (Eutectic Mixture of Local Anesthetics) | Lidocaine 2.5% + Prilocaine 2.5% | 60 min | Under occlusive dressing |
| Ametop (tetracaine gel) | Tetracaine 4% | 30 min | Under occlusive dressing |
| LMX 4/5 (liposomal lidocaine) | Lidocaine 4% or 5% | 30-60 min | Applied directly |
Open Wounds
| Agent | Composition | Onset | Use |
|---|---|---|---|
| LET gel | Lidocaine 4% + Epinephrine 0.1% + Tetracaine 0.5% | 20-30 min | Wound lacerations; avoid mucous membranes and end-arteries |
Mucous Membranes
| Agent | Composition | Onset | Use |
|---|---|---|---|
| Benzocaine spray (Hurricane) | Benzocaine 20% | 15-30 seconds | Oropharyngeal procedures |
| Viscous lidocaine 2% | Lidocaine 2% | 2-5 min | Upper airway procedures |
| ZAP gel | Benzocaine 18% + Tetracaine 2% | 5 min | Mucosal surfaces |
General Principles of Safe Use
- Always calculate total dose before injection - especially in small patients or large wounds
- Aspirate before injection to avoid intravascular deposition
- Inject slowly - reduces pain and allows detection of inadvertent IV injection
- Use smallest effective volume at the lowest effective concentration
- Alkalinization (adding NaHCO₃): raises pH of solution → more drug in unionized form → faster onset and less injection pain (1 mEq NaHCO₃ per 10 mL lidocaine)
- Warming the LA to body temperature reduces injection pain
Techniques to Reduce Pain of Injection
- Apply topical anesthetic before needle puncture
- Use small-bore needle (27-30 gauge)
- Slow injection rate
- Warm the solution
- Stretch or vibrate skin at puncture site
- Distract the patient during injection
- Insert needle through pores or hair follicles
- Use bevel-up needle orientation
Local Anesthetic Systemic Toxicity (LAST)
LAST results from dose-related sodium channel blockade in non-target tissues - primarily the brain and heart.
Risk Factors
- Excessive dose
- Inadvertent intravascular injection
- Highly vascular injection site (intercostal > paracervical > epidural > brachial plexus > sciatic/femoral)
- Patients with reduced hepatic function, cardiac disease, or extremes of age
Clinical Progression (CNS then Cardiovascular)
CNS Toxicity (early → late):
- Circumoral/tongue numbness and tingling
- Metallic taste
- Light-headedness, tinnitus, visual disturbances
- Agitation, confusion, tremors
- Seizures (hallmark of significant CNS toxicity)
- CNS depression, respiratory arrest
Cardiovascular Toxicity (later, more severe):
- Hypotension
- Conduction block (PR prolongation, QRS widening)
- Ventricular arrhythmias (especially with bupivacaine - due to its high lipid solubility and tight Na⁺ channel binding)
- Cardiovascular collapse / refractory cardiac arrest
Note: Bupivacaine is particularly cardiotoxic because it dissociates very slowly from blocked Na⁺ channels ("fast in, slow out"), making cardiac toxicity difficult to reverse.
Management of LAST
| Step | Intervention |
|---|---|
| Stop injection | Immediately cease LA administration |
| Airway/O₂ | 100% oxygen; intubate if necessary |
| Seizures | IV benzodiazepines (first line); avoid phenytoin (also Na⁺ channel blocker) |
| Cardiac arrest | Standard ACLS; avoid vasopressin and lidocaine as resuscitation agents |
| Lipid Rescue | IV 20% lipid emulsion (Intralipid) |
Lipid Emulsion Protocol (20% Intralipid):
- Bolus: 1.5 mL/kg IV over 1 minute
- Infusion: 0.25 mL/kg/min, continued for 10 minutes after hemodynamic stability
- Repeat bolus if hemodynamic instability persists
- Maximum dose: ~10 mL/kg over the first 30 minutes
Mechanism: lipid emulsion acts as a "lipid sink," sequestering the highly lipophilic LA (especially bupivacaine) from cardiac and neuronal tissue.
Special Considerations
Allergy
- True allergy to amide LAs is extremely rare
- Ester LAs produce PABA (para-aminobenzoic acid) as a metabolite - a known allergen; cross-reactivity exists among esters
- No cross-reactivity between ester and amide classes
- Patients with suspected allergy to both classes: diphenhydramine 1% or benzyl alcohol with epinephrine can be used as alternative infiltration agents
Methemoglobinemia
- Prilocaine and benzocaine can oxidize ferrous (Fe²⁺) hemoglobin to ferric (Fe³⁺) methemoglobin
- Cyanosis occurs when methemoglobin concentration exceeds 1.5 g/dL
- Treatment: IV methylene blue 1-2 mg/kg
- Risk: excessive doses, neonates (reduced methemoglobin reductase activity)
Pregnancy
- Most LAs are category B/C
- Avoid large doses; placental transfer occurs (fetal bradycardia risk with bupivacaine)
- Prilocaine avoided (methemoglobin risk to fetus)
Regional Anesthesia (Nerve Blocks)
Regional anesthesia deposits LA adjacent to peripheral nerves, providing analgesia for an entire nerve territory without wound distortion.
Advantages over subdermal infiltration:
- Eliminates wound distortion from large-volume local injection
- Superior pain control on extremities
- Less total drug required
- Reduces procedure-related anxiety
Indications: complex lacerations, fractures, dislocations, abscesses, debridement, joint procedures.
Important pre-block assessment: Document distal neurovascular status before any regional block to avoid masking primary traumatic injury. Check: skin color, temperature, capillary refill, pulses, sensation, and motor function. For digital injuries: test two-point discrimination (normal <6 mm at fingertips, often <2 mm).
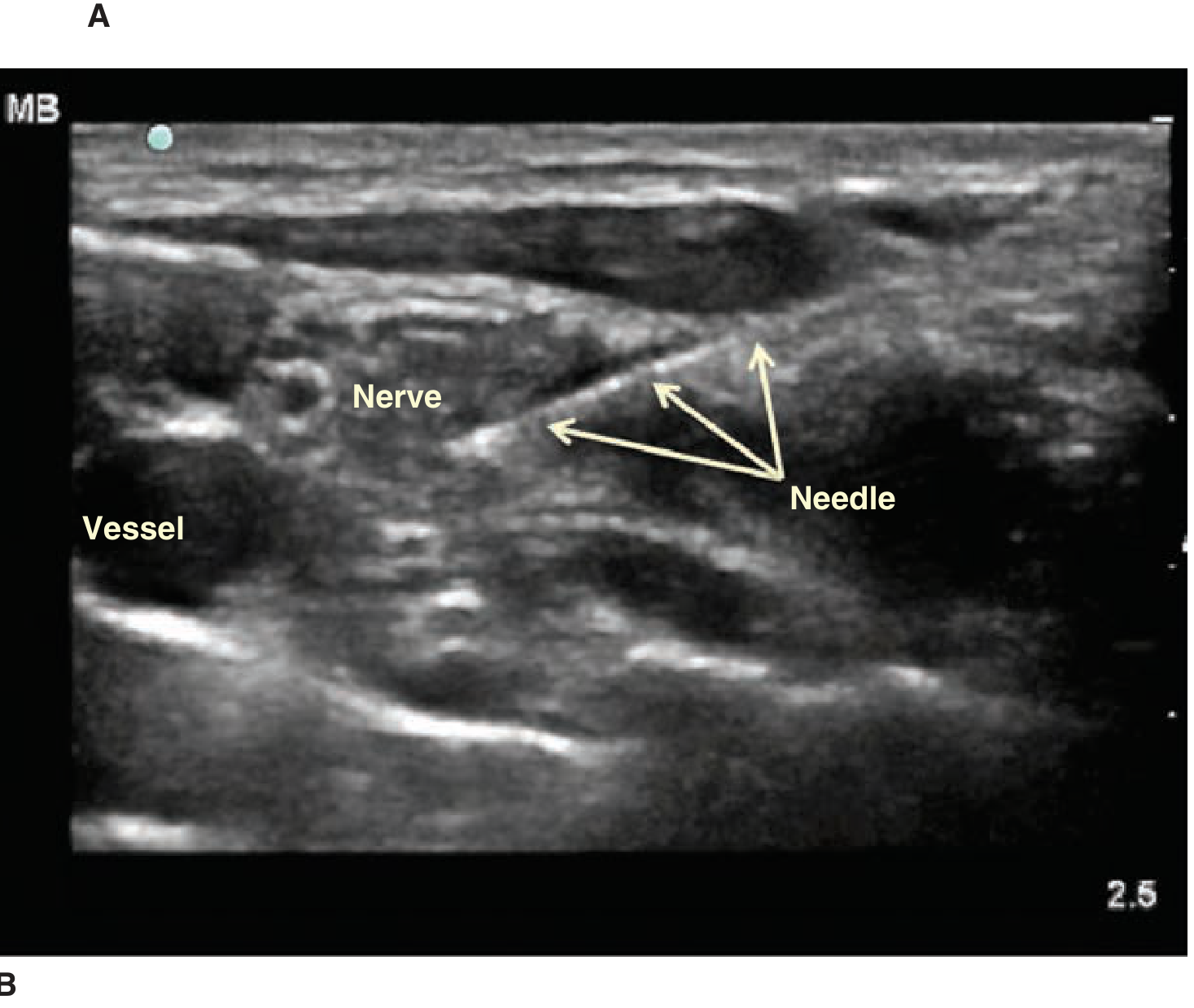
Ultrasound-Guided Nerve Blocks
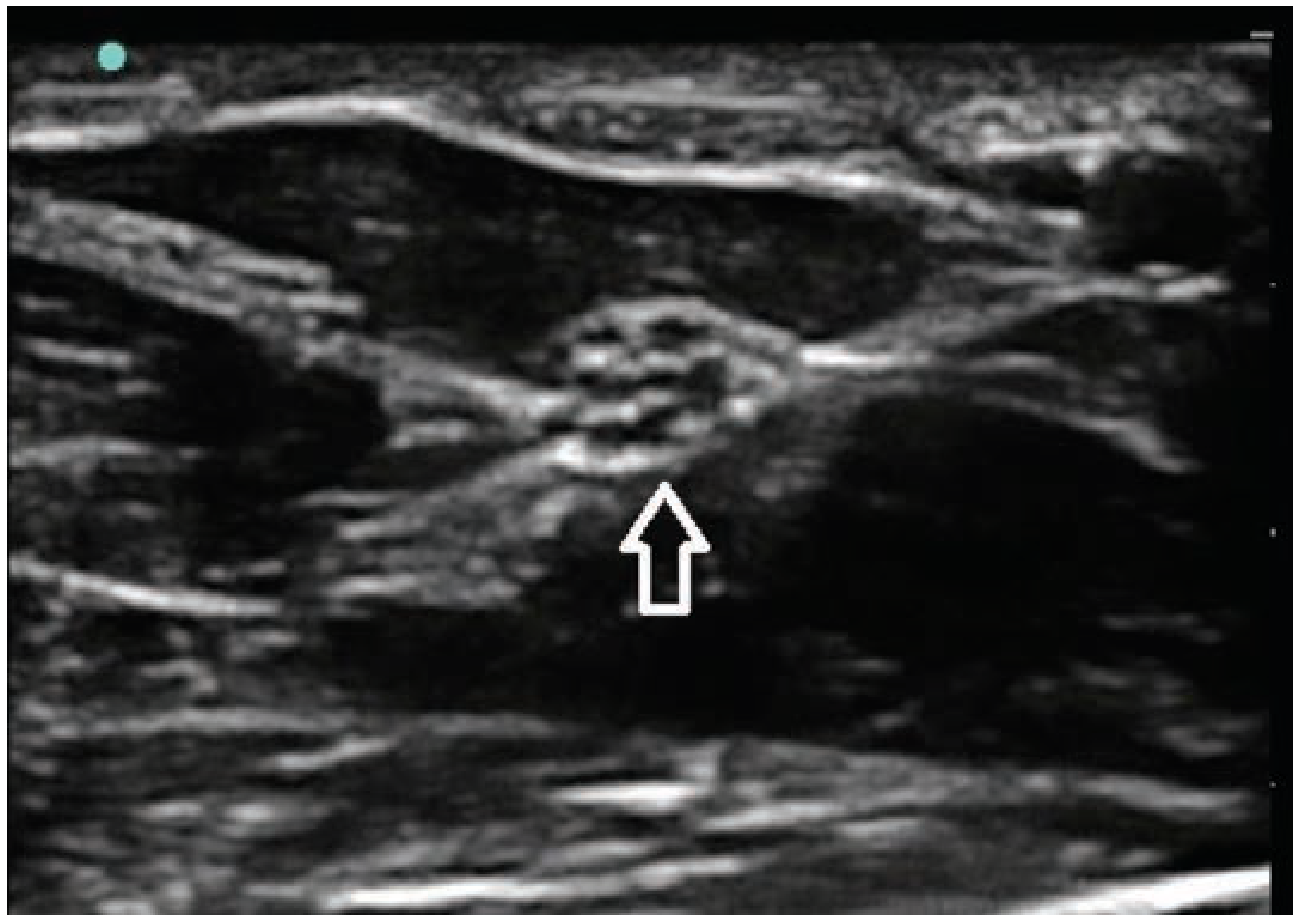
Ultrasound guidance has transformed regional anesthesia in the ED:
- Nerves appear as white, hyperechoic, honeycomb-patterned structures in cross-section
- The needle appears as a bright white hyperechoic line on US
- Allows real-time visualization of needle tip and LA spread
- Increases success rate, reduces volume of LA required, reduces complications
Agent Selection for Regional Blocks
- Lidocaine: fastest onset (~10-20 min to optimal block); intermediate duration
- Bupivacaine / ropivacaine / levobupivacaine: longer onset (15-30 min) but duration of 4-8 hours; preferred when prolonged post-procedure analgesia is desired
- Levobupivacaine and ropivacaine are preferred for blocks where large volumes are needed due to significantly lower cardiotoxicity than bupivacaine
Common ED Nerve Blocks
| Block | Nerve | Anesthetized Area |
|---|---|---|
| Median nerve block | Median nerve at wrist | Palmar thumb, index, middle, radial half of ring finger |
| Ulnar nerve block | Ulnar nerve at wrist (deep to flexor carpi ulnaris) | 5th digit, medial half of 4th digit, medial hand |
| Radial nerve block | Radial nerve (subcutaneous field over anatomic snuffbox) | Dorsum of thumb, index, middle, radial half of ring finger |
| Digital nerve block | Volar/dorsal digital nerves | Individual finger or toe |
| Femoral nerve block | Femoral nerve in femoral triangle | Anterior thigh, knee, medial leg |
| Fascia iliaca block | Femoral + obturator + lateral femoral cutaneous | Anterior and medial thigh (hip fractures) |
Summary
Local anesthetics are indispensable in emergency medicine. Effective use requires:
- Understanding ester vs amide classification and metabolism
- Matching agent to clinical need: onset (pKa), duration (protein binding), potency (lipid solubility)
- Respecting maximum doses and using aspiration technique
- Recognizing and managing LAST - CNS symptoms precede cardiovascular collapse; treat with benzodiazepines for seizures and 20% IV lipid emulsion for cardiovascular toxicity
- Using topical agents to reduce needle pain and vasoconstrictors to extend duration
- Employing ultrasound-guided regional blocks as a powerful, opioid-sparing analgesic strategy in the ED
Source: Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 11th Edition - Chapter 36: Local and Regional Anesthesia (Gibbs & Wu), pp. 278-290
Write me 20 marks short note on regional blocks based on chapter 36 of book tintinalli emergency medicine 11 th edition
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have all the content and images needed. Here is the comprehensive 20-mark short note:
Regional Blocks
Short Note - 20 Marks
Based on Chapter 36: Local and Regional Anesthesia, Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 11th Edition (Gibbs & Wu)
Introduction
Regional anesthesia (nerve blocks) is a technique where local anesthetic is infiltrated adjacent to peripheral nerves, anesthetizing an entire nerve territory. It is used in the ED for complicated lacerations, abscess drainage, fractures, dislocations, debridement, and procedures on the extremities and face.
Advantages over subdermal infiltration:
- Eliminates wound distortion from large-volume local injection
- Requires smaller total drug volume
- Provides superior pain control on extremities
- Reduces patient anxiety and improves procedural outcomes
- With careful technique, serious complications are uncommon
Pre-Block Assessment (Mandatory)
Before any regional block, assess and document distal neurovascular status to avoid masking a primary traumatic neurovascular injury.
- Vascular: skin color, temperature, capillary refill time, pulses
- Neurologic: cutaneous sensation (pain, touch), motor function (active movement, strength)
- Digital injuries: test two-point discrimination on the volar pad before injection
- Normal: <6 mm at fingertips (often <2 mm)
- Compare with contralateral digit
Nerve Localization Techniques
1. Landmark Technique
- Most common in ED practice
- Relies on anatomical surface landmarks to guide needle placement
- Disadvantage: anatomic variation; requires larger LA volumes to compensate for imprecision
2. Peripheral Nerve Stimulator
- Uses electrically insulated needles
- Stimulates motor response at 0.5-1.0 mA when needle is near the target nerve (motor twitch)
- Reduces reliance on paresthesia and improves success rate
3. Ultrasound (US) Guidance
- Now the preferred technique in well-equipped EDs
- Nerves appear as white, hyperechoic, honeycomb-patterned structures in cross-section
- Needle visualized as a bright white hyperechoic line
- Allows real-time confirmation of needle tip position and LA spread around the nerve
Benefits of US guidance: shortens onset time, increases success rate, reduces total LA volume, reduces complications, confirms proper spread.
Onset Times
- Lidocaine: optimal analgesia at 10-20 minutes
- Bupivacaine/ropivacaine: optimal analgesia at 15-30 minutes
- Pain and temperature are affected first, then touch, deep pressure, then motor function
- Intraneural injection causes significant pain - if excessive pain occurs on injection, withdraw the needle 2-3 mm and wait for pain to subside before resuming
HAND AND WRIST BLOCKS
Digital Nerve Block
Purpose: Anesthesia to an entire finger or toe. Used for finger lacerations, paronychia drainage, nail removal/repair, fracture/dislocation reduction.
Anatomy: Each digit is supplied by four digital nerves - two palmar digital nerves (from median/ulnar nerves) on the lateral and medial volar aspects, and two smaller dorsal digital nerves (from radial/ulnar nerves) on the dorsolateral aspects.
Technique:
- Hand prone (palm down)
- Insert needle on the dorsal surface of the proximal phalanx
- Advance toward the volar surface, tangential to the phalanx
- Aspirate, deposit 1 mL at the volar corner, withdraw injecting another 1 mL back to skin
- Redirect needle across the dorsum of the digit, inject 1 mL band subcutaneously
- Repeat on the opposite side of the digit
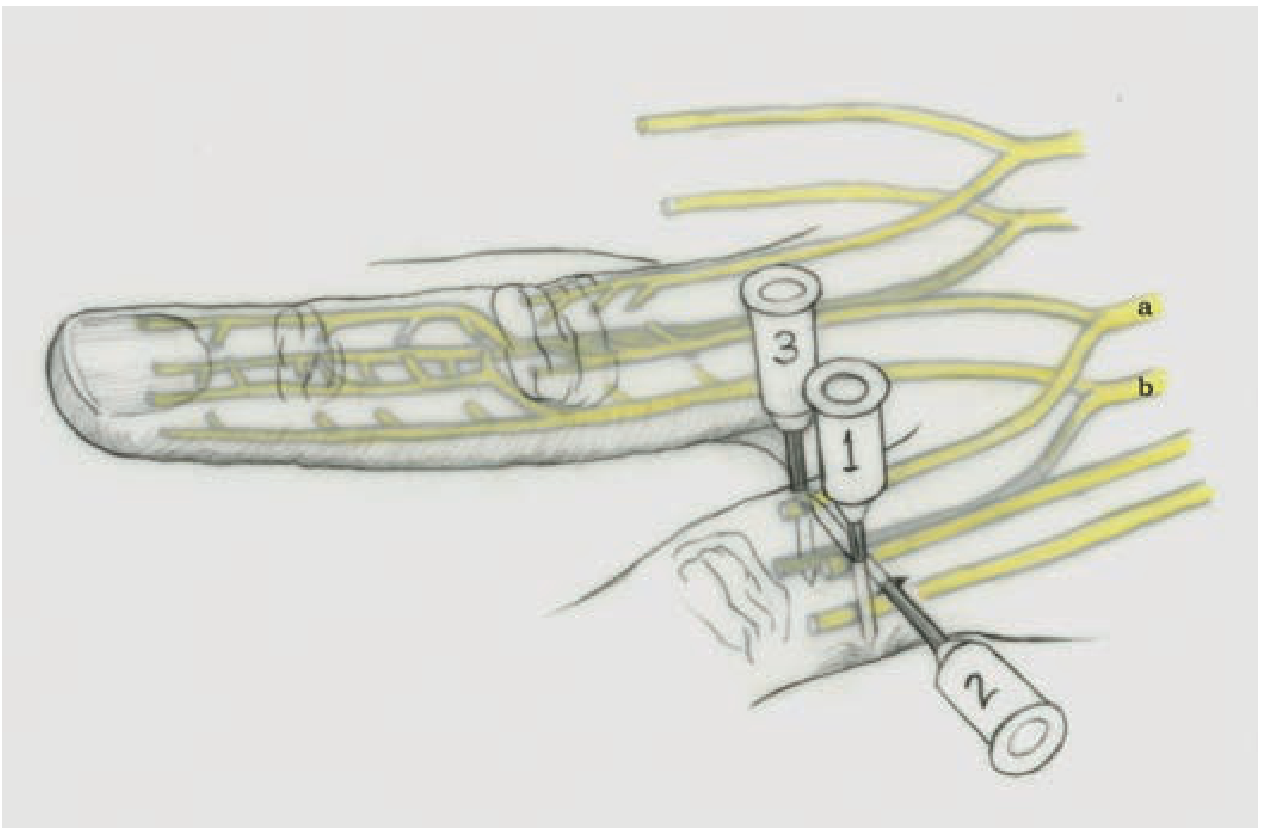
Note: Lidocaine 1% with epinephrine provides less injection pain than bupivacaine 0.5%, though duration is approximately half as long. Metacarpal block (at metacarpal heads) is an alternative particularly useful for long and ring fingers.
Transthecal (Flexor Tendon Sheath) Block: Deposits LA into the flexor tendon sheath on the palmar aspect at the distal palmar crease, providing an alternative digital block - however may not fully anesthetize the distal fingertip.
Median Nerve Block at the Wrist
Purpose: Anesthesia to the palmar surface of the thumb, index, middle finger, and radial half of the ring finger.
Anatomy: The median nerve lies between the palmaris longus and flexor carpi radialis (FCR) tendons at the wrist. Identify the palmaris longus by opposing thumb and little finger against resistance.
Technique: Raise a wheal at the proximal wrist crease. Insert the needle between the palmaris longus and FCR tendons, advance 5-10 mm deep to the flexor retinaculum, aspirate, and inject 3-5 mL.
Ulnar Nerve Block at the Wrist
Purpose: Anesthesia to the entire fifth digit, medial half of the fourth digit, and medial hand.
Anatomy: The ulnar nerve travels deep to the flexor carpi ulnaris (FCU) tendon at the wrist. Identify FCU - the most prominent ulnar-sided tendon when the patient makes a fist.
Technique: Raise a wheal 1-2 cm proximal to the distal wrist crease. Insert the needle under the FCU tendon an additional 5-10 mm past the skin surface, aspirate, and inject 3-5 mL. A dorsal subcutaneous band block may be added to ensure coverage of dorsal branches.
Radial Nerve Block at the Wrist
Purpose: Anesthesia to the dorsum of the thumb, index, middle finger, and the radial half of the ring finger and dorsum of the hand.
Anatomy: The superficial radial nerve divides into multiple branches over the anatomic snuffbox (bounded by extensor pollicis brevis, extensor pollicis longus, and the radial styloid).
Technique: Raise a wheal over the lateral radial styloid and inject 5 mL subcutaneously. Reinsert needle and redirect medially (ulnar direction) across the dorsal wrist, injecting an additional 5 mL band to capture smaller branches. A generous injection is used due to the unpredictable distribution.
LOWER EXTREMITY BLOCKS
Femoral Nerve Block
Purpose: Excellent pain control for proximal femur and hip fractures, especially in the elderly. Provides anesthesia to the anterior thigh and medial leg.
Anatomy: At the inguinal ligament and inguinal crease, the femoral nerve lies lateral to and slightly deeper than the femoral artery. Mnemonic: NAVEL from lateral to medial = Nerve, Artery, Vein, Empty space, Lymph nodes.
"Three-in-one" block: Uses the same injection site but applies distal pressure after injection to promote cephalad spread of LA, blocking the femoral, obturator, and lateral femoral cutaneous nerves simultaneously - provides broader hip and thigh coverage.
Technique:
- Patient supine; pillow under hip for obese patients
- Identify femoral artery by palpation
- Insert needle 1 cm lateral to the artery, just below the inguinal ligament
- Aspirate, inject 20-30 mL of LA with a fascial "pop" or under US guidance
- With US: deposit LA in a "donut" pattern around the nerve under direct visualization
Fascia Iliaca Block
Purpose: A more reliable alternative to the three-in-one block for hip and femur fractures. Blocks femoral, obturator, and lateral femoral cutaneous nerves by infiltrating a large LA volume beneath the fascia iliaca.
Technique (landmark):
- Draw a line from ASIS to pubic tubercle, divide into thirds
- Injection site: 1 cm below the junction of the lateral and middle thirds
- Advance needle through subcutaneous tissue and two fascial "pops" (fascia lata, then fascia iliaca)
- Inject 40 mL of LA with fan-like spread to fill the fascial compartment
- US guidance confirms the correct fascial plane (LA seen spreading beneath fascia iliaca)
FOOT AND ANKLE BLOCKS
The entire foot can be anesthetized by blocking five nerves at the level of the ankle:
| Nerve | Sensation | Block Site |
|---|---|---|
| Posterior tibial | Plantar foot (sole) | Posterior to posterior tibial artery, behind medial malleolus |
| Sural | Lateral heel and foot | Field block from Achilles tendon to lateral malleolus |
| Deep peroneal | Web space 1st/2nd toe | Between extensor hallucis longus and tibialis anterior at medial malleolus level |
| Superficial peroneal | Dorsum of foot | Subcutaneous field from lateral malleolus to tibialis anterior tendon |
| Saphenous | Medial ankle | Subcutaneous band from tibialis anterior to superior medial malleolus |
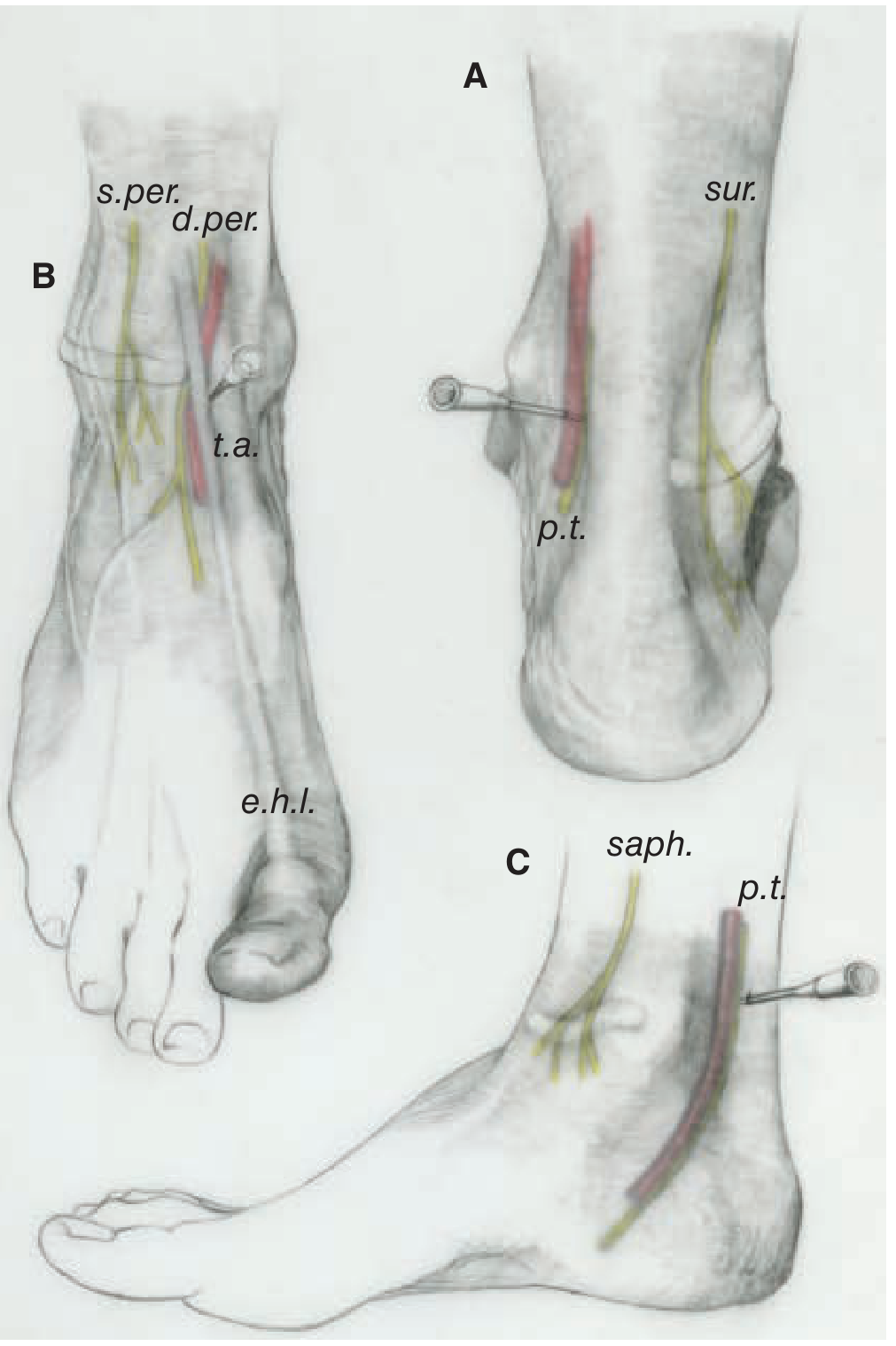
Posterior Tibial Nerve Block
- Most important nerve for plantar foot anesthesia
- Inject 5-7 mL just posterior to the posterior tibial artery at the level of the medial malleolus
- US guidance recommended to visualize artery and adjacent nerve
FACIAL NERVE BLOCKS
Facial blocks provide excellent analgesia with minimal tissue distortion. They are based on the three terminal branches of the trigeminal nerve (V1, V2, V3), each exiting through a facial foramen aligned vertically in line with the pupil.
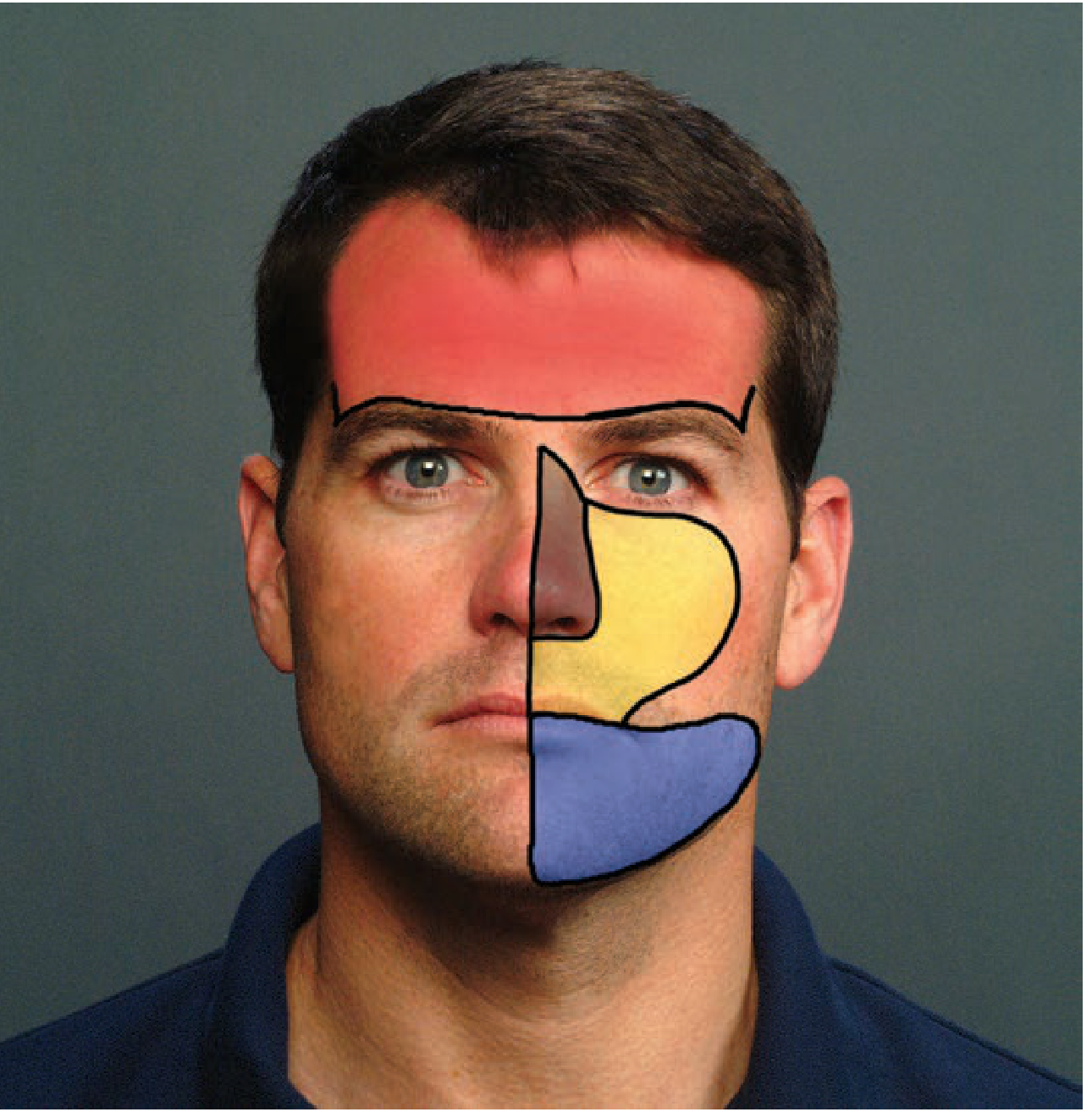
Supraorbital and Supratrochlear Nerve Block (V1)
Area anesthetized: Entire forehead up to vertex of scalp; bridge of nose.
Anatomy:
- Supraorbital nerve exits the supraorbital foramen - in line with the pupil, above the superior orbital rim
- Supratrochlear nerve exits 5-10 mm medial to the supraorbital foramen
Technique: Raise a wheal just superior to the eyebrow in line with the pupil (2-3 mL), then direct the needle medially to raise a horizontal wheal to the medial eyebrow border (additional 5 mL). Total 7-8 mL.
Uses: Forehead lacerations, scalp lacerations, eyebrow lacerations.
Infraorbital Nerve Block (V2)
Area anesthetized: Lower eyelid, medial cheek, ala and tip of nose, upper lip, upper incisors and canines.
Anatomy: Exits the infraorbital foramen, 5-10 mm inferior to the midpoint of the orbital rim, just cranial to the maxillary canine tooth.
Technique (intraoral approach - preferred):
- Apply topical anesthetic to mucosa above the maxillary canine
- Dry and retract the upper lip
- Insert needle at the gingival reflection above the canine, advance superiorly halfway to the orbital rim
- Inject 3-5 mL
Uses: Lip lacerations, cheek and nose lacerations, dental pain.
Mental Nerve Block (V3)
Area anesthetized: Labial mucosa, gingiva, lower lip adjacent to the incisors and canines.
Anatomy: The mental nerve exits the mental foramen, located inferior to the mandibular canines and first premolars.
Technique (intraoral approach):
- Apply topical anesthetic to the mucosa below the canines
- Evert the lower lip
- Insert needle at the gingival reflection, advance inferiorly approximately 1 cm
- Inject 3-5 mL
Uses: Lower lip and chin lacerations, dental procedures.
THORACIC BLOCKS
Intercostal Nerve Block
Purpose: Excellent analgesia for rib fractures, tube thoracostomy site pain, and thoracic herpes zoster. Duration: 8-18 hours with a long-acting LA.
Anatomy: The intercostal nerve, artery, and vein run in the subcostal groove of each rib. Order from superior to inferior within the groove: Vein, Artery, Nerve (VAN). Ribs 1-6 are difficult to block due to the scapula; optimal block site is at the rib angle (~6 cm lateral to midline, just lateral to paraspinous muscles).
Patient position: Sitting upright, ipsilateral arm raised with wrist resting on head (opens rib spaces).
Technique:
- Palpate inferior border of the rib
- Retract skin cephalad at the rib angle
- Insert needle bevel-up, angled 10-15 degrees cephalad
- Walk needle off the inferior rib edge into the subcostal groove (~3 mm advance)
- Aspirate carefully (for blood and air)
- Inject 2-5 mL per level
Complication: Pneumothorax in 8-9% of cases (1.4% per individual block). Monitor for 30 minutes post-procedure; bedside US can check for pneumothorax.
Agent Selection for Regional Blocks
| Agent | Onset to Full Block | Duration | Advantage |
|---|---|---|---|
| Lidocaine 1-2% | 10-20 min | 1-2 hours | Fastest onset; most popular |
| Bupivacaine 0.25-0.5% | 15-30 min | 4-8 hours | Long post-procedure analgesia |
| Ropivacaine 0.5% | 15-30 min | 4-6 hours | Long-acting; less cardiotoxic than bupivacaine |
| Levobupivacaine 0.25-0.5% | 10-20 min | >8 hours | Longest duration; least cardiotoxic of long-acting agents |
- Long-acting agents are preferred when prolonged post-procedure analgesia is desired, or when the provider may be interrupted during a long procedure
- Adding epinephrine prolongs duration and reduces systemic absorption but is contraindicated in digital and penile blocks (end-arterial territories)
Complications of Regional Blocks
| Complication | Cause | Prevention/Management |
|---|---|---|
| Failed block | Anatomic variation; wrong technique | US guidance; adequate volume; allow sufficient onset time |
| Intravascular injection / LAST | Needle in vessel; high-dose injection | Always aspirate; use test dose; inject slowly; have lipid emulsion ready |
| Nerve injury | Intraneural injection | Withdraw if patient reports sharp pain; never inject against resistance |
| Infection | Contaminated technique | Sterile technique; avoid injecting through infected tissue |
| Hematoma | Vascular puncture | Aspirate before injection; apply pressure if vessel entered |
| Pneumothorax | Intercostal block | Monitor 30 min; bedside US; CXR if symptomatic |
| Masking injury | Block conceals traumatic neuropathy | Pre-block neurovascular documentation is mandatory |
Summary
Regional nerve blocks are among the most effective analgesic tools available in the ED. Key principles:
- Always document neurovascular status before the block
- US guidance is preferred where available - improves success and safety
- Aspirate before every injection to avoid intravascular deposition
- Withdraw if intraneural pain occurs - do not inject into the nerve
- Allow adequate onset time - lidocaine ~15 min, bupivacaine ~20-30 min
- Match agent to clinical need: lidocaine for short procedures; bupivacaine/ropivacaine for prolonged analgesia
- Topical anesthetic before block placement reduces procedure-associated pain
Source: Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 11th Edition - Chapter 36: Local and Regional Anesthesia (Gibbs & Wu), pp. 280-290
This is a shared conversation. Sign in to Orris to start your own chat.