Here is a comprehensive, exam-ready answer covering all the topics you have listed, drawn from Smith and Tanagho's General Urology, Campbell-Walsh-Wein Urology, Bailey & Love's Surgery, and other authoritative textbooks.
URINE EXAMINATION
Indications of Urine Examination
Urinalysis is not a screening tool for all patients but should be ordered when clinically indicated. Key indications include:
- Urinary tract symptoms - dysuria, frequency, urgency, hesitancy, nocturia
- Haematuria (gross or microscopic)
- Suspected urinary tract infection (UTI)
- Renal diseases - acute/chronic kidney disease, glomerulonephritis, nephrotic syndrome
- Hypertension and diabetes mellitus (monitoring for proteinuria)
- Renal colic / urolithiasis
- Pre-operative workup
- Fever of unknown origin
- Screening for metabolic disorders (diabetes - glycosuria; PKU - phenylketonuria)
- Monitoring treatment response in renal or urological disease
- Suspected malignancy of urothelium (cytology)
- Post-partum or antenatal surveillance
URINE EXAMINATION - TYPES
A. Macroscopic (Physical/Gross) Examination
Color:
| Color | Cause |
|---|
| Colorless | Overhydration, very dilute urine, diabetes insipidus |
| Cloudy/milky | Phosphaturia, pyuria, chyluria |
| Red/pink | Haematuria, haemoglobinuria, myoglobinuria, drugs (rifampicin) |
| Orange | Dehydration, phenazopyridine, bilirubin |
| Brown/cola | Glomerular bleeding, urobilinogen, porphyria, myoglobin |
| Green-blue | Biliverdin, Pseudomonas infection, drugs (amitriptyline, methylene blue) |
| Black | Alkaptonuria, melaninuria |
Normal urine is pale yellow due to the pigment urochrome. - Smith & Tanagho's General Urology, Campbell-Walsh-Wein Urology
Turbidity: Cloudy urine is most commonly caused by:
- Phosphaturia (benign; clears with acetic acid - alkaline urine)
- Pyuria (leukocyturia with characteristic pungent odour)
- Chyluria (lymph-urine fistula), lipiduria, hyperoxaluria
Odour: Infected urine has a pungent, ammoniacal odour. Maple syrup urine disease has a characteristic sweet odour. Foetor of bacterial UTI is due to ammonia from urea-splitting organisms.
Specific Gravity (SG): Normal 1.010-1.025. Isosthenuria (SG fixed at 1.010) indicates severe renal tubular damage. SG < 1.003 is seen in diabetes insipidus.
B. Microscopic Examination
A fresh midstream clean-catch specimen should be centrifuged (400 g, 5 min), the sediment resuspended and examined under low and high power.
Normal findings:
- 0-5 RBCs/hpf
- 0-5 WBCs/hpf
- Occasional epithelial cells
- No casts, bacteria, or significant crystals
Abnormal findings and significance:
| Finding | Significance |
|---|
| >5 RBCs/hpf | Haematuria - UTI, stones, glomerulonephritis, tumour, trauma |
| >5 WBCs/hpf | Pyuria - UTI, renal TB, interstitial nephritis |
| Red cell casts | Glomerulonephritis (pathognomonic) |
| White cell casts | Pyelonephritis, interstitial nephritis |
| Granular/waxy casts | Chronic renal disease, tubular necrosis |
| Hyaline casts | Normal (exercise, dehydration), fever |
| Fatty casts | Nephrotic syndrome |
| Bacteria | UTI (>10⁵ organisms/mL is significant on culture) |
| Uric acid crystals | Gout, uric acid lithiasis, tumour lysis |
| Calcium oxalate crystals | Hyperoxaluria, ethylene glycol poisoning |
| Phosphate crystals | Alkaline urine, infection with urea-splitting organisms |
| Cystine crystals (hexagonal) | Cystinuria |
| Epithelial cell casts | Acute tubular necrosis |
Types of casts and their significance:
- Casts form in the distal nephron/collecting duct - they take the shape of the tubule
- The matrix is Tamm-Horsfall mucoprotein
- Presence of cellular elements within casts indicates active renal pathology
C. Biochemical (Chemical) Examination
Usually performed by dipstick (test strip). Key parameters:
| Parameter | Normal | Abnormal finding | Clinical significance |
|---|
| pH | 4.6-8.0 | Acid (<4.6) / Alkaline (>8.0) | Acidosis/alkalosis, dietary, stone type assessment |
| Protein | Absent (trace <150 mg/day) | Proteinuria (>300 mg/day) | Glomerular disease, nephrotic syndrome, pre-eclampsia |
| Glucose | Absent | Glycosuria | DM, Fanconi syndrome, renal glycosuria |
| Ketones | Absent | Ketonuria | DKA, starvation, vomiting |
| Blood (haem) | Absent | Haematuria/haemoglobinuria | Stones, tumour, infection, trauma, haemolysis |
| Bilirubin | Absent | Bilirubinuria | Obstructive jaundice, hepatitis |
| Urobilinogen | Trace | Increased: hepatocellular / haemolytic; Absent: obstructive jaundice | Liver disease, haemolysis |
| Nitrite | Absent | Positive | Bacteriuria (gram-negative organisms) |
| Leukocyte esterase | Absent | Positive | Pyuria, UTI |
| Specific gravity | 1.010-1.025 | Low: DI; High: dehydration, DM | Concentrating ability assessment |
Proteinuria grading:
- Microalbuminuria: 30-300 mg/day - early diabetic nephropathy marker
- Macroproteinuria: >300 mg/day - established glomerular disease
- Nephrotic range: >3.5 g/day
Bence-Jones protein (dipstick negative but positive on heating at 40-60°C, dissolves at 100°C) - multiple myeloma.
D. Cytological Examination
Urine cytology examines exfoliated urothelial cells for:
- High-grade transitional cell carcinoma (TCC)/urothelial carcinoma - most useful
- Carcinoma in situ (CIS) - urine cytology is especially valuable as CIS may not be visible on cystoscopy
- Viral inclusions (CMV, BK virus in transplant patients)
- Atypical/suspicious cells warranting further investigation
Technique: Fresh voided specimen or bladder washings; Papanicolaou staining. Sensitivity for high-grade TCC ~80-90%, but poor for low-grade tumours.
E. Bacteriological (Microbiological) Examination
Indications: Suspected UTI, pyelonephritis, renal TB, post-treatment surveillance.
Specimen: Midstream clean-catch urine (MSU); catheter specimen (CSU); suprapubic aspiration (SPA - gold standard for neonates).
Significant bacteriuria: ≥10⁵ colony-forming units (CFU)/mL in symptomatic patients (Kass's criterion). In catheterised patients or SPA, even lower counts are significant.
Common pathogens:
- E. coli (70-80% community UTIs)
- Klebsiella, Proteus mirabilis, Enterococcus, Pseudomonas aeruginosa (hospital-acquired)
- Staphylococcus saprophyticus (young women)
Renal TB: Urine shows sterile pyuria (WBCs on microscopy but no growth on standard culture). Requires Lowenstein-Jensen medium or PCR for Mycobacterium tuberculosis. Early morning urine (EMU) x 3 specimens.
Clinical Significance of Abnormal Urine Findings
| Abnormal Finding | Clinical Significance |
|---|
| Haematuria | Glomerulonephritis (RBC casts), urolithiasis, UTI, tumour, trauma, coagulopathy, schistosomiasis |
| Proteinuria (>3.5 g/day) | Nephrotic syndrome (minimal change disease, membranous GN, FSGS, DM) |
| Pyuria + bacteria | Bacterial UTI |
| Sterile pyuria | Renal TB, chlamydial urethritis, treated UTI, interstitial nephritis, analgesic nephropathy |
| Glycosuria (normal blood glucose) | Renal glycosuria (Fanconi syndrome, proximal tubular defect) |
| Haemoglobinuria | Intravascular haemolysis (G6PD deficiency, mismatched transfusion, PNH, falciparum malaria) |
| Myoglobinuria | Rhabdomyolysis (trauma, statin toxicity, electric shock) |
| Bilirubin in urine | Conjugated hyperbilirubinaemia (obstructive jaundice, hepatitis) |
| Casts (RBC) | Active glomerulonephritis - pathognomonic |
| Casts (WBC) | Pyelonephritis, acute interstitial nephritis |
| Granular/waxy casts | Chronic renal failure |
| Ketonuria | DKA, starvation, prolonged vomiting |
RENAL FUNCTION TESTS
Creatinine and Blood Urea Nitrogen (BUN)
Blood Urea Nitrogen (BUN)
- Reference range: 7-18 mg/dL
- BUN is a product of protein (amino acid) catabolism via the urea cycle in the liver
- Urea is freely filtered at the glomerulus and approximately 40-50% is passively reabsorbed in the proximal tubule
Causes of elevated BUN (azotaemia):
- Prerenal: Dehydration, hypovolaemia, heart failure, GI bleeding (digestion of blood adds to urea load), high protein diet, hypercatabolic states (sepsis, corticosteroids)
- Renal: Acute/chronic kidney disease (intrinsic renal failure)
- Postrenal: Urinary tract obstruction
Causes of low BUN: Severe liver disease (impaired urea synthesis), malnutrition, SIADH, overhydration.
Serum Creatinine
- Reference range: Males 0.7-1.2 mg/dL; Females 0.5-1.0 mg/dL
- Creatinine is a product of muscle creatine phosphate metabolism - it is produced at a constant rate proportional to muscle mass
- Almost entirely excreted by glomerular filtration (5-10% tubular secretion at normal GFR; as GFR falls, tubular secretion contributes more)
- Creatinine is NOT reabsorbed by the tubules
Clinical significance:
- A reliable marker of GFR - serum creatinine rises as GFR falls
- A parabolic (inverse, non-linear) relationship exists: a doubling of creatinine indicates ~50% loss of GFR
- Important limitation: Creatinine may remain in normal range despite significant GFR loss (the "creatinine-blind zone") because of compensatory hyperfiltration by remaining nephrons
- Factors falsely raising creatinine: drugs (cimetidine, trimethoprim, fenofibrate), rhabdomyolysis (muscle breakdown), high meat intake
- Factors falsely lowering creatinine: low muscle mass (elderly, malnutrition, amputation), advanced liver disease
eGFR (estimated GFR): The preferred clinical tool. Calculated using CKD-EPI or MDRD formula from serum creatinine, age, sex, and race. Normal >90 mL/min/1.73 m². eGFR <60 for >3 months = CKD.
BUN : Creatinine Ratio
- Normal ratio: 10:1 to 15:1 (in mg/dL units); 40:1-60:1 in mmol/L
- Ratio >20:1 (prerenal or postrenal): Hypovolaemia, GI bleeding, high protein intake, hypercatabolism, obstructive uropathy. In prerenal states, elevated ADH causes increased proximal tubular water and urea reabsorption, disproportionately raising BUN.
- Ratio 10:1 (intrinsic renal disease): Acute tubular necrosis, glomerulonephritis - BUN and creatinine rise proportionately
| Parameter | Prerenal AKI | Intrarenal AKI |
|---|
| BUN/Cr ratio | >20 | <20 |
| Urine Na (mmol/L) | <20 | >40 |
| FENa (%) | <1% | >1% |
| Urine osmolality | >500 mmol/kg | <350 mmol/kg |
| Sediment | Normal / hyaline casts | Muddy brown granular casts |
- Comprehensive Clinical Nephrology 7th Ed., Textbook of Family Medicine 9th Ed.
IMAGING OF THE URINARY TRACT
Plain X-Ray KUB (Kidney, Ureter, Bladder)
Definition and Purpose
A plain abdominal radiograph (without contrast) covering the region from the upper poles of the kidneys to the base of the bladder. KUB stands for Kidneys, Ureters, Bladder.
Indications
- Suspected renal/ureteric calculi (first-line screening)
- Flank pain / acute renal colic
- Follow-up of known radio-opaque urinary calculi (post-ESWL or post-ureteroscopy)
- Assessment of stone burden before surgical planning (PCNL, ESWL)
- Abdominal pain - assess bowel gas pattern, organomegaly
- Pre-IVU scout film (baseline for contrast study)
- Monitoring for catheter or stent position
- Screening for calcification (adrenal, lymph node, AAA calcification)
Technique
Patient in supine position, AP view. The film must include the diaphragm to the symphysis pubis, covering the entire urinary tract. No bowel preparation required for emergency; some advocate for it electively.
Normal Findings on Plain KUB
- Kidneys: Visible as soft-tissue shadows ("renal outline") alongside the psoas shadow. Right kidney slightly lower than left. Size: 11-14 cm (3.5 vertebral body lengths). Smooth outlines.
- Psoas shadow: Symmetric, well-defined lateral margin of the psoas major muscle bilaterally.
- Ureters: Not visible on plain KUB.
- Bladder: May be seen as a soft-tissue density in the pelvis if full.
- Bowel gas: Scattered gas in non-dilated small and large bowel.
- Bony structures: Lumbar vertebrae, sacrum, pelvis, lower ribs - no lytic/sclerotic lesions.
Abnormal Findings
| Finding | Clinical Significance |
|---|
| Radio-opaque shadow in renal area/ureteric course | Renal/ureteric calculus (calcium oxalate, calcium phosphate - 70-80% radiopaque) |
| Radiolucent stones | Uric acid, pure cystine, indinavir stones (not visible on KUB; seen on CT) |
| Absent/obliterated psoas shadow | Retroperitoneal collection, haematoma, psoas abscess |
| Enlarged renal shadow | Hydronephrosis, polycystic kidney disease, renal tumour |
| Small kidney(s) | Chronic renal disease, renal artery stenosis, reflux nephropathy |
| Dilated bowel loops (paralytic ileus) | Peritonitis, ureteric colic (reflex ileus), post-operative |
| Soft tissue mass displacing bowel | Retroperitoneal tumour, large renal mass |
| Calcification in renal area | Nephrocalcinosis (hyperparathyroidism, RTA, medullary sponge kidney), TB |
| Calcification in pelvis | Phlebolith (common benign vascular calcification) - distinguished from ureteric stone by "bull's eye" lucent centre |
| Spinal abnormalities | Spina bifida (associated with neurogenic bladder) |
| Eggshell calcification | Renal cyst, lymph node |
Sensitivity: KUB detects ~45-85% of stones. Pure uric acid and small stones are missed. NCCT (non-contrast CT) is the gold standard for stone diagnosis.
Clinical Context:
- Renal calculi: A radiopaque shadow in the line of the ureter (L1-L5, then along the bony pelvic brim, into pelvis) suggests ureteric calculus. Pain is colicky with radiation to groin/testicle.
- Urinary tract obstruction: Plain KUB may show dilated bowel (paralytic ileus from ureteric colic), or loss of psoas shadow from inflammatory mass.
Intravenous Urography (IVU) / Intravenous Pyelography (IVP)
Definition
IVU (IVP) is a radiological examination in which intravenous iodinated contrast medium is injected; as it is filtered by the kidney and excreted in the urine, sequential X-rays demonstrate the renal parenchyma, pelviocalyceal system, ureters, and bladder opacified with contrast. - NKF Primer on Kidney Diseases 8e
Indications
- Haematuria (investigating source - upper vs. lower tract)
- Renal/ureteric calculi - to assess obstruction, anatomy, and collect system
- Suspected urinary tract obstruction (hydronephrosis / hydroureter)
- Renal anomalies (horseshoe kidney, duplex system, ectopic kidney)
- Recurrent UTI (structural abnormalities, reflux)
- Suspected urothelial tumour of the upper tract
- Flank pain / loin pain
- Pre-surgical planning
- Suspected PUJ (pelviureteric junction) obstruction
- Bladder mass assessment
Note: IVU has been largely replaced by CT urography (CTU) in modern practice, which provides superior detail, speed, and multi-organ assessment. However, IVU remains relevant in settings with limited CT availability.
Procedure / Technique
- Pre-procedure: Check serum creatinine (contraindicated if significantly elevated), allergy history, hydration status, metformin (hold 48 hours pre-procedure), thyroid function if history of thyroid disease.
- Scout film (KUB): Plain AP radiograph of the entire urinary tract.
- Contrast injection: 1-2 mL/kg of non-ionic iodinated contrast (e.g., iohexol, iomeprol) injected IV as a bolus.
- Timed films:
- 1-3 min (nephrogram phase): Renal parenchyma opacifies homogenously - assesses renal size, outline, and perfusion.
- 5 min: Pelviocalyceal system fills - PCS anatomy, calyces, pelvis.
- 10-15 min: Ureters fill - course, calibre, filling defects, obstruction.
- 20-25 min: Full length ureters + bladder.
- Post-micturition film: Residual urine, bladder emptying, lower ureteric detail.
- Compression: A compression band may be applied over the ureters to enhance pelvicalyceal filling.
- Oblique views for ureteric calculi or bladder lesions.
Normal IVU Findings
- Bilateral symmetrical nephrogram within 3 minutes
- Smooth renal outlines; right kidney at L1-L3, left at T12-L2
- PCS: Elegant calyceal pattern with sharp fornices and papillae
- Ureters: Pencil-thin, course along transverse processes, cross the SI joint to the pelvis
- Bladder: Smooth wall, rounded, no filling defects
- Normal post-void: minimal residual
Abnormal IVU Findings
| Finding | Clinical Significance |
|---|
| Delayed / absent nephrogram | Severe obstruction, renal artery occlusion, absent kidney |
| Dense prolonged nephrogram | Acute ureteric obstruction (contrast concentrates due to low GFR) |
| Dilated PCS + dilated ureter | Urinary tract obstruction - level seen at point of hold-up |
| Filling defect in ureter | Calculus (radiolucent on KUB but filling defect on IVU), blood clot, tumour, air bubble |
| Blunt calyces ("clubbing") | Chronic pyelonephritis, reflux nephropathy |
| Spider leg calyces | Medullary sponge kidney |
| Hydronephrosis | PUJ obstruction, ureteric calculus, external compression |
| Distorted calyces | Renal mass (tumour, cyst - "stretching" or "amputation" of calyces) |
| No contrast in one kidney | Non-functioning kidney (XGP, chronic obstruction, agenesis) |
| Bladder filling defect | Tumour, calculus, blood clot, enlarged prostate impression |
| Bladder trabeculation | Bladder outflow obstruction (BPH, urethral stricture, neurogenic bladder) |
| Vesicoureteric reflux | Contrast refluxing up ureters on post-void film |
| Horseshoe kidney | Calyces point medially/posteriorly, low-lying kidneys with medial fusion |
Contraindications to IVU:
- Severe contrast allergy (relative - premedicate)
- Renal failure (creatinine >200 mmol/L) - contrast nephrotoxicity risk
- Myelomatosis (contrast may precipitate acute renal failure in myeloma kidney)
- Diabetes mellitus with metformin (hold metformin)
- Pregnancy (radiation risk)
- Severe dehydration (increases contrast nephrotoxicity)
Retrograde Ureteropyelography (Retrograde Urogram)
Definition
Retrograde ureteropyelography (RGU/retrograde urogram) is a radiological technique in which contrast medium is injected in a retrograde direction (upward from the bladder) into the ureter via a ureteric catheter placed cystoscopically, opacifying the ureter and renal pelvis/calyces without relying on renal function.
Indications
- Failed or non-diagnostic IVU - when the kidney is not functioning or IVU is inadequate
- Renal failure (does not rely on GFR; contrast is not absorbed systemically in significant amounts)
- Contrast allergy to IV contrast
- Evaluation of ureteral obstruction - defines level, length, and nature of stricture
- Filling defects in ureter or PCS seen on IVU - differentiates calculus, clot, tumour, extrinsic compression
- Haematuria workup when other investigations are inconclusive
- Pre-operative planning - before ureteroscopy, PCN, or ureteroplasty
- PUJ obstruction - to confirm diagnosis and length of stricture
- Evaluation of trauma to the ureter
- Stent placement guidance
- Upper tract urothelial carcinoma evaluation
Technique (Retrograde Ureteropyelography)
- Anaesthesia: Spinal or general anaesthesia (procedure is done under cystoscopic guidance).
- Positioning: Lithotomy position.
- Cystoscopy: Rigid or flexible cystoscope is inserted; both ureteric orifices are identified.
- Ureteric catheterisation: A 5-6 Fr open-ended ureteric catheter (or Chevassu catheter) is advanced under vision into the ureteric orifice and up the ureter.
- Contrast injection: Water-soluble iodinated contrast (e.g., urografin 15-25%) is gently injected in controlled amounts (5-10 mL) under fluoroscopic guidance. Avoid over-distension (risk of pyelosinus backflow, bacteraemia, and post-procedure fever).
- Fluoroscopic images: AP and oblique films are taken to image the ureter, PUJ, and pelviocalyceal system.
- Retrograde pyelogram vs. retrograde ureterogram: If the catheter is advanced to the renal pelvis, a pyelogram is obtained; if it only fills the ureter, it is a ureterogram.
- Ureteric catheter placement: A stent or catheter may be left in situ as part of treatment.
Normal Retrograde Urogram Findings
- Ureter smooth, uniform calibre throughout (3-4 mm)
- No filling defects, no strictures
- Smooth, symmetric pelviocalyceal system
- No extravasation of contrast
- Normal PUJ without delay
Abnormal Findings and Clinical Significance
| Abnormal Finding | Clinical Significance |
|---|
| Filling defect in ureter | Calculus (smooth outline), urothelial tumour (irregular), blood clot (changes shape), radiolucent calculus |
| "Column of contrast" stops at a point - cutoff | Ureteric obstruction - extrinsic compression (pelvic tumour, retroperitoneal fibrosis, lymph nodes) or intrinsic stricture |
| Ureteric stricture | Seen as a segment of narrowing - causes: TB, previous surgery, schistosomiasis, radiation, trauma |
| PUJ hold-up | PUJ obstruction - classic "champagne glass" or flask-shaped pelvis with narrow PUJ |
| Hydronephrosis | Dilated calyces and pelvis proximal to obstruction |
| Irregular/filling defect in pelvis or calyces | Urothelial carcinoma of the renal pelvis, papillary necrosis (ring shadows in calyces) |
| Extravasation of contrast | Ureteral perforation, forniceal rupture |
| Duplex system | Two separate collecting systems opacified |
| Medial displacement of ureter | Retroperitoneal fibrosis (ureters deviate medially and are encased) |
| Lateral displacement | Aortic aneurysm, retroperitoneal mass |
| "Cobra head" sign | Ureterocele (ballooning of distal ureter with thin radiolucent halo) |
Ultrasonography (USG) in Urogenital Diseases
Importance and Advantages
- No ionising radiation - safe in children and pregnant women
- Real-time imaging - dynamic assessment of organ vascularity (Doppler)
- Portable and widely available
- Can detect hydronephrosis, renal masses, calculi (with posterior acoustic shadowing), bladder abnormalities
- Guides percutaneous procedures (biopsies, nephrostomy)
Indications in Urogenital Diseases
| Condition | What USG Shows |
|---|
| Renal calculi | Echogenic foci with posterior acoustic shadowing; ureteric calculi may be seen at VUJ or PUJ |
| Hydronephrosis | Dilated pelviocalyceal system; graded I-IV (SFU classification) |
| Renal masses | Cystic vs. solid differentiation (Bosniak classification for cysts); renal cell carcinoma (solid, hyperechoic or heterogeneous) |
| Renal agenesis/ectopia | Absent renal shadow in fossa |
| Horseshoe kidney | Isthmus visible anterior to aorta; low-lying medially fused kidneys |
| Polycystic kidney disease | Multiple bilateral renal cysts enlarging kidneys |
| Renal vein thrombosis | Doppler shows absent renal vein flow |
| Testicular torsion | Absent blood flow on Doppler to the affected testis |
| Prostate | Volume calculation (normal <30 mL); BPH; post-void residual volume; prostatic calculi |
| Bladder tumour | Intraluminal mass; staging (muscle invasion); post-void residual |
| Pelviureteric junction obstruction | Antenatally - fetal pyelectasis; postnatally - hydronephrosis with non-visualised ureter (PUJ cause) |
| Scrotal pathology | Epididymo-orchitis, hydrocele, varicocele, epididymal cysts |
| Ovarian/uterine pathology | Fibroid, ovarian cysts, ectopic pregnancy |
Limitations of USG: Operator-dependent; poor for ureters; limited by bowel gas and body habitus; cannot detect small calculi; poor for uric acid stones.
HAEMATURIA
Causes of Haematuria
Haematuria is defined as the presence of red blood cells in urine (>3-5 RBCs/hpf on microscopy). It may be gross (macroscopic) or microscopic.
Classification by Origin
Upper Urinary Tract:
- Glomerulonephritis (IgA nephropathy - most common cause of recurrent haematuria worldwide, post-streptococcal GN, Henoch-Schönlein purpura, MPGN, focal segmental GS)
- Renal calculi / nephrolithiasis
- Renal cell carcinoma (painless haematuria - classic triad: haematuria, loin pain, flank mass)
- Transitional cell carcinoma of the renal pelvis
- Renal tuberculosis
- Polycystic kidney disease
- Medullary sponge kidney
- Renal trauma / injury
- Renal vein thrombosis
- Arteriovenous malformation
- Sickle cell trait/disease
- Alport syndrome (hereditary nephritis with deafness and ocular defects)
Lower Urinary Tract:
- Urinary tract infection (cystitis, urethritis)
- Carcinoma of the bladder (transitional cell carcinoma) - most common cause of painless haematuria in adults >40 years
- Ureteric calculi
- Bladder calculi
- Urethral stricture
- Benign prostatic hyperplasia (BPH)
- Carcinoma of the prostate
- Schistosomiasis (Schistosoma haematobium - "Egyptian haematuria")
- Bladder trauma / cyclophosphamide-induced haemorrhagic cystitis
- Urethral caruncle / polyp
Systemic Causes:
- Coagulopathy (haemophilia, warfarin, antiplatelet therapy)
- Thrombocytopaenia
- Infective endocarditis
- Malignant hypertension
- Radiation therapy (radiation cystitis)
Important localisation clue - Three-glass test:
- Initial haematuria (first glass only): Anterior urethral lesion
- Terminal haematuria (last glass only): Bladder neck, prostate, posterior urethra
- Total haematuria (all three glasses): Kidney, ureter, or posterior bladder
Homoeopathic Therapeutics for Haematuria
The following medicines are commonly indicated based on totality of symptoms, constitutional picture, and characteristic modalities:
| Medicine | Key Indications |
|---|
| Cantharis vesicatoria | Haematuria with intolerable burning, strangury (painful straining to void); intense urging; bloody urine; cutting pain before, during, and after urination; worse touch, cold water |
| Berberis vulgaris | Haematuria from renal calculi; radiating pain from kidneys down the ureter; burning, sore pain; turbid, mucous urine; pale, earthy face; worse motion, jarring |
| Phosphorus | Haematuria from bright red blood; bleeding from any mucous membrane; renal inflammation; haematuria with weakness; fatty degeneration of kidneys |
| Terebinthina (Oil of Turpentine) | Haematuria with smoky, bloody urine; strangury; burning in urethra; nephritis; haemorrhages from mucous membranes; urine smells like violets |
| Nitric acid | Haematuria with oxalic acid or uric acid diathesis; offensive urine; burning, tearing pains; alternating constipation and diarrhoea; splinter-like pains |
| Arnica montana | Haematuria from trauma; bruised, sore feeling; dark blood; urine dark with smoky appearance after injuries |
| Hamamelis virginiana | Passive venous haemorrhage; dark, non-coagulable blood; haematuria from venous congestion; phlyctenular haematuria; haemorrhage associated with varicosities |
| Ipecacuanha | Bright-red haematuria with nausea; active haemorrhage; uterine and renal haemorrhage |
| Digitalis | Haematuria in cardiac failure with renal congestion; smoky urine; scanty urine |
| Ferrum phosphoricum | Haematuria in first stage of inflammation; bright red blood; no other strong indications; first aid remedy |
| Erigeron canadensis | Haematuria from bladder irritation; bloody urine with violent dysuria; haemorrhage from kidneys and uterus |
| Lycopodium | Renal calculi with haematuria; right-sided; red sandy sediment; bloating; 4-8 PM aggravation |
| Sarsaparilla | Haematuria from calculi; urine passes better standing; bloody urine at end of micturition; gravel in urine; pain at end of urination |
Note: Homoeopathic prescribing is based on the totality of symptoms (mental, general, and particular) and must be individualised. The above represents commonly used indicated remedies.
HORSESHOE KIDNEY
Description
Horseshoe kidney is the most common renal fusion anomaly, occurring in approximately 1 in 400 live births (some sources cite 1 in 400-600), with a 2:1 male predominance. The two kidneys are fused at their lower poles by an isthmus of renal parenchyma (90% of cases) or fibrous tissue (10% of cases). - Bailey & Love's Surgery 28th Ed.
Embryology: During the 6th-9th weeks of gestation, the metanephric blastemas fuse at their lower poles before completing cephalad migration. The isthmus becomes trapped beneath the inferior mesenteric artery (IMA), preventing further ascent. This results in:
- Low-lying kidneys (isthmus at L4-L5 vertebral level)
- Malrotation - renal pelves face anteriorly (instead of the normal medial position)
- Calyces point medially and posteriorly (instead of laterally)
- High insertion of the ureters on the renal pelvis (aberrant)
Clinical Significance
Most horseshoe kidneys are asymptomatic and discovered incidentally on imaging. When symptomatic:
- Pelviureteric Junction (PUJ) Obstruction: Due to high ureteral insertion, aberrant vessels crossing the PUJ, and the malrotated position. Leads to recurrent flank pain, hydronephrosis.
- Urinary Stasis and Calculi: Impaired drainage predisposes to stone formation (prevalence of stones ~20%). Stones often lodge in lower pole calyces.
- Recurrent UTI: Stasis predisposes to infection.
- Associated Anomalies:
- Genital anomalies (hypospadias, cryptorchidism, bicornuate uterus, duplex vagina)
- Cardiovascular anomalies (VSD, ASD, coarctation of aorta)
- Vesicoureteric reflux
- Turner syndrome (~7% of girls with Turner syndrome have horseshoe kidney)
- Increased incidence of Wilms' tumour (nephroblastoma) - 2x higher than general population
- Increased incidence of TCC of the renal pelvis (from chronic stasis/infection)
- Carcinoid tumours of the horseshoe kidney (rare but well-documented association)
- Abdominal aortic aneurysm surgery hazard - isthmus lies anterior to the aorta and may complicate surgery
- Trauma - isthmus is vulnerable to compression against the lumbar spine in abdominal trauma
Radiological Modalities and Findings
Plain X-Ray KUB
- Low-lying kidney shadows, medially directed lower poles
- Calculi visible if present (radiopaque)
- Isthmus may cast a soft tissue shadow across the midline anterior to the spine
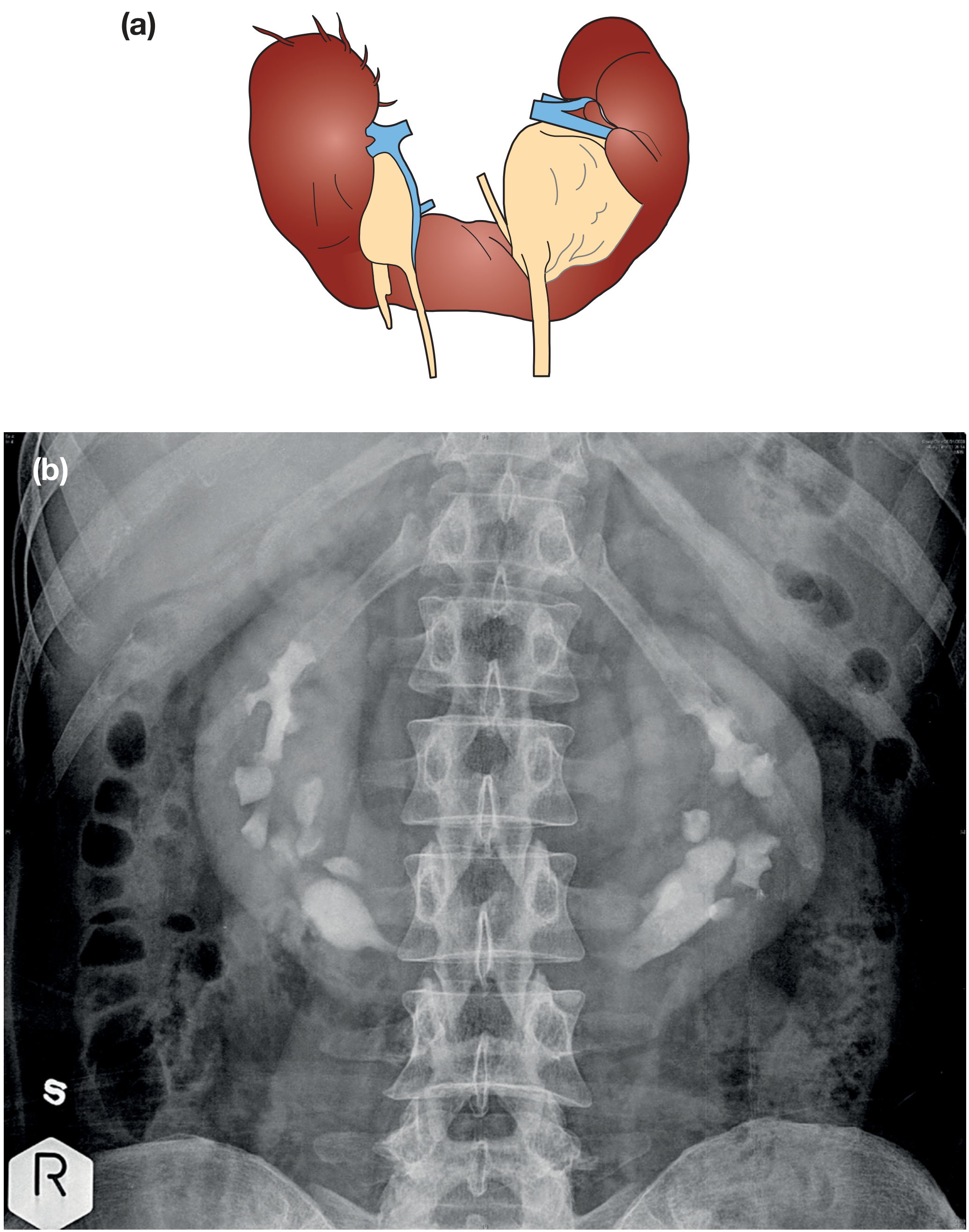
Intravenous Urography (IVU) - Classic Imaging
Classic IVU findings (as illustrated in the image above):
- Low-lying kidneys with lower poles directed medially
- Calyces pointing medially and posteriorly (in a "flower vase" or inverted configuration)
- Renal pelves facing anteriorly (as opposed to normal medial orientation)
- Possible dilation of the PCS indicating PUJ obstruction
- "Flower vase sign" - the PCS configuration resembling an inverted flower vase
- Ureters may appear to drape over the isthmus
- Delayed drainage on the affected side if PUJ obstruction is present
See the IVU image of horseshoe kidney showing posteriorly oriented calyces:
(Figure 82.2 from Bailey & Love's Surgery - (a) Anatomical illustration of horseshoe kidney showing fused lower poles; (b) IVU at 5 minutes showing posterior orientation of calyces in horseshoe kidney)
Ultrasound
- Isthmus visualised as a band of tissue anterior to the aorta and inferior vena cava
- Low-lying kidneys with medially directed lower poles
- Useful for detecting hydronephrosis, calculi, or renal masses
CT Scan / MRI (Preferred for Preoperative Assessment)
- Modality of choice for full anatomical delineation
- Clearly demonstrates: isthmus, aberrant vessels, collecting system anatomy, relation to great vessels, bowel (risk of retrorenal colon)
- Contrast CT shows: PCS anatomy, corticomedullary differentiation, renal masses, stone burden
- Essential before PCNL, isthmus division, or oncological surgery
Nuclear Medicine (Isotope Renogram - MAG3/DTPA)
- Assesses differential renal function (split function) in each moiety
- Identifies obstruction at the PUJ (drainage curves)
- Useful pre-operatively if surgical division of isthmus or pyeloplasty planned
Sources: Smith & Tanagho's General Urology 19th Ed. | Campbell-Walsh-Wein Urology | Bailey & Love's Short Practice of Surgery 28th Ed. | Comprehensive Clinical Nephrology 7th Ed. | NKF Primer on Kidney Diseases 8th Ed. | Textbook of Family Medicine 9th Ed. | Medscape Retrograde Pyelography | Johns Hopkins Medicine - KUB