Osteoarthritis and gouty arthritis
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive information from the textbook. Let me compile a thorough answer.
Osteoarthritis and Gouty Arthritis
OSTEOARTHRITIS (OA)
Definition & Overview
Osteoarthritis (also called degenerative joint disease) is a disorder characterized by degeneration of articular cartilage resulting in structural and functional failure of synovial joints. It is the most common disease of joints. Despite the "-itis" suffix, it is primarily a degenerative disorder - inflammation is secondary, not primary.
- Primary (idiopathic) OA: ~95% of cases; appears insidiously as an aging phenomenon; oligoarticular; affects weight-bearing joints
- Secondary OA: ~5% of cases; arises in younger individuals from joint deformity, prior injury, or systemic disease (diabetes, obesity)
- Prevalence increases exponentially after age 50; ~40% of people over 70 are affected
Pathogenesis
Biomechanical stress is the principal mechanism. Genetic factors (polymorphisms in matrix and signaling genes) also contribute. The sequence of events:
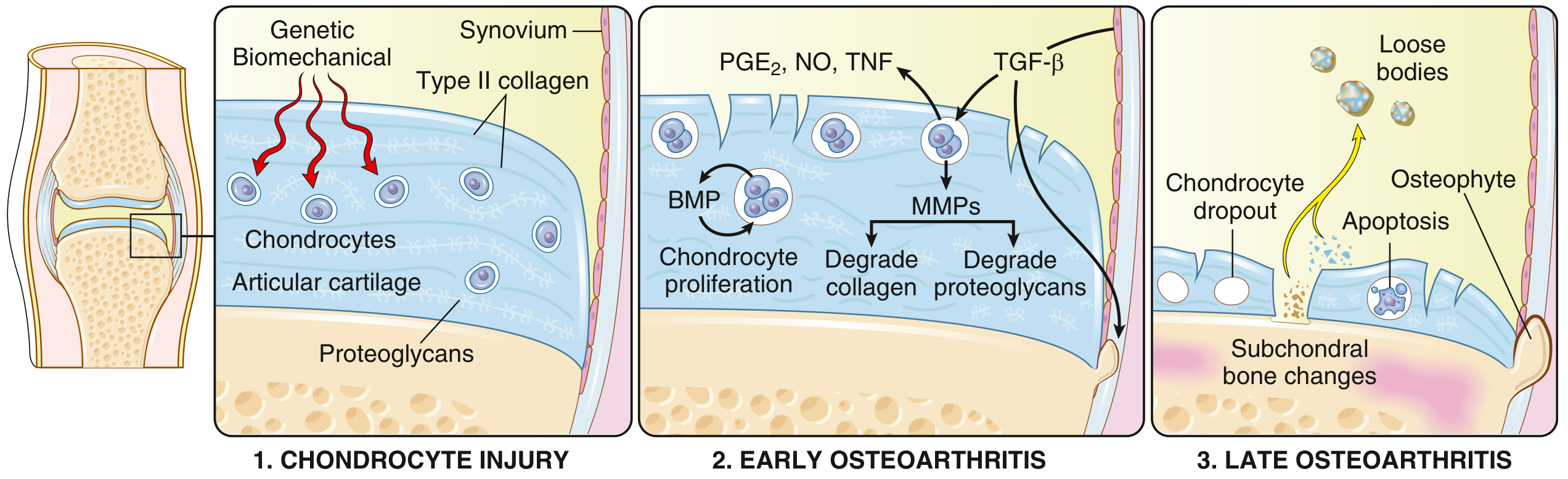
FIG. 19.31 - Stages of OA: (1) Chondrocyte injury, (2) Early OA with degradation exceeding repair, (3) Late OA with chondrocyte loss and subchondral bone damage.
- Chondrocyte injury - from biomechanical stress, in a genetically predisposed patient
- Early OA - chondrocytes proliferate and attempt repair, but release MMPs (matrix metalloproteinases) that degrade collagen and proteoglycans. Inflammatory mediators (PGE2, NO, TNF) perpetuate damage. TGF-β attempts counter-regulation but is overwhelmed.
- Late OA - chondrocyte dropout (apoptosis), full-thickness cartilage loss, subchondral bone changes, osteophyte formation at articular margins
Key molecular mediators include:
- Degradative: MMPs, aggrecanases, PGE2, nitric oxide, TNF, IL-1
- Reparative (inadequate): TGF-β, BMP (bone morphogenetic protein)
Morphology
Advanced OA shows:
- Fibrillation and loss of articular cartilage - cartilage becomes frayed, vertical clefts form
- Loose bodies ("joint mice") - fragments of dislodged cartilage and subchondral bone in the joint space
- Bone eburnation - exposed subchondral bone is polished ivory-like from friction
- Subchondral cysts - synovial fluid forced into bone through fracture gaps via a ball-valve mechanism
- Osteophytes - bony outgrowths at articular margins, capped by fibrocartilage, that gradually ossify
- Mild synovitis - congested, fibrotic synovium with scattered chronic inflammatory cells (minimal, unlike RA)
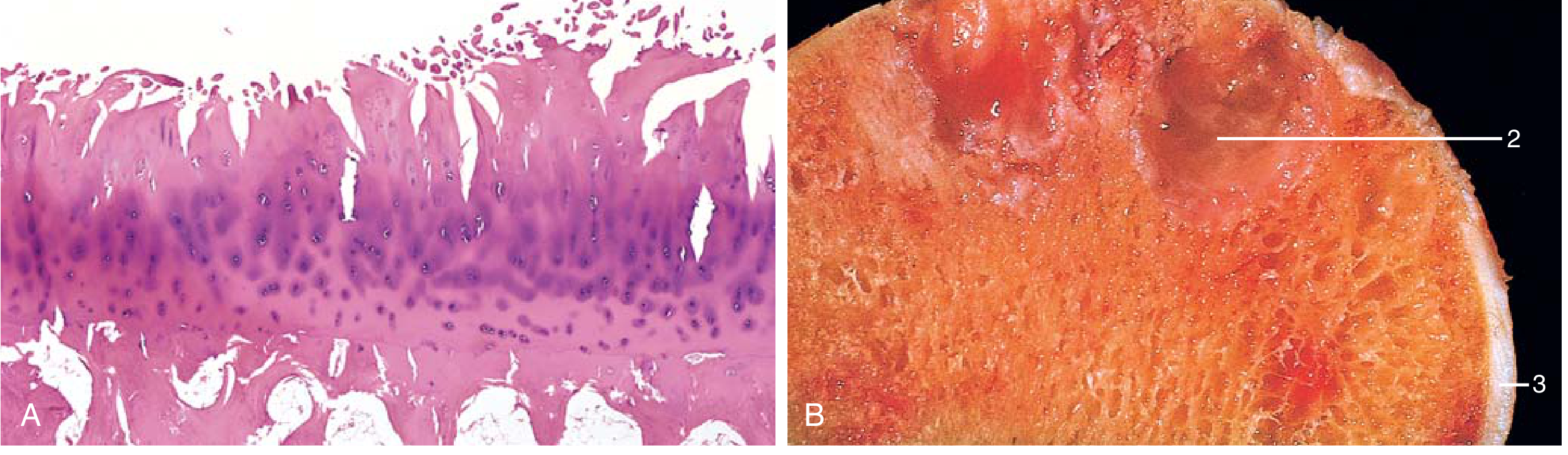
FIG. 19.32 - (A) Fibrillation of articular cartilage. (B) Eburnated articular surface showing: (1) exposed subchondral bone, (2) subchondral cyst, (3) residual articular cartilage.
Clinical Features
- Typically presents in patients in their 50s+; if younger, search for an underlying cause
- Symptoms: joint pain worsening with use, morning stiffness (brief, <30 min), crepitus, limited range of motion
- Osteophytes on spine - compress cervical/lumbar nerve roots → radicular pain, muscle spasms, atrophy, neurologic deficits
- Joints involved: hips, knees, lower lumbar and cervical vertebrae, proximal and distal interphalangeal (PIP/DIP) finger joints, first carpometacarpal joints, first tarsometatarsal joints
- Heberden nodes - osteophytes at DIP joints; more common in women
- Bouchard nodes - osteophytes at PIP joints
- No joint fusion (unlike RA)
- Radiographic severity does not correlate well with pain and disability
Treatment
- Pain management (acetaminophen, NSAIDs to reduce inflammation)
- Intra-articular corticosteroids
- Activity modification, weight loss
- Joint replacement for severe cases
- No disease-modifying therapy currently prevents or halts OA progression
GOUTY ARTHRITIS
Definition & Overview
Gout is characterized by transient attacks of acute arthritis initiated by monosodium urate (MSU) crystals deposited within and around joints. It is driven by hyperuricemia (plasma urate >6.8 mg/dL), which is necessary but not sufficient for gout to develop.
- Primary gout: ~90% of cases; most commonly due to reduced renal excretion of uric acid (cause usually unknown)
- Secondary gout: ~10%; due to identifiable causes of hyperuricemia
Pathogenesis of Hyperuricemia
Uric acid is the final end-product of purine catabolism in humans (we lack uricase). Sources of excess urate:
Overproduction:
- Increased purine synthesis via the de novo pathway or salvage pathway defects
- Partial HGPRT (hypoxanthine guanine phosphoribosyltransferase) deficiency - interrupts the salvage pathway
- Complete HGPRT absence = Lesch-Nyhan syndrome (severe neurologic manifestations dominate)
- Rapid cell lysis (tumor lysis syndrome from chemotherapy)
Underexcretion:
- Uric acid is normally filtered by the glomerulus, then almost completely reabsorbed by the proximal tubule, with a small fraction secreted by the distal nephron
- Reduced distal secretion is the basis of primary gout in most patients
- Chronic renal disease reduces excretion
Other contributing factors (beyond hyperuricemia):
- Age and duration of hyperuricemia (gout usually appears after 20-30 years of sustained hyperuricemia)
- Alcohol consumption (increases urate production and impairs excretion)
- Diet high in purines (red meat, shellfish)
- Only ~10% of hyperuricemic individuals ever develop gout
Mechanism of Joint Inflammation
Once MSU crystals precipitate in the joint:
- Resident synovial macrophages phagocytose urate crystals
- Crystals activate the cytosolic NLRP3 inflammasome
- Inflammasome activates caspase-1 → cleaves pro-IL-1β into active IL-1β
- IL-1β recruits and activates neutrophils into the joint
- Neutrophils release cytokines, free radicals, and proteases
- Crystals also rupture phagolysosomal membranes → lysosomal enzyme leakage
- Result: intense acute inflammatory arthritis, which typically remits spontaneously in days to weeks
Morphology
Acute gouty arthritis:
- Intense neutrophilic infiltrate in synovium and synovial fluid
- MSU crystals in neutrophil cytoplasm - long, slender, needle-shaped, negatively birefringent under polarized light
- Synovium is edematous and congested
Chronic tophaceous arthritis:
- Repeated attacks → urate crystals encrust the articular surface
- Pannus (hyperplastic, fibrotic, inflamed synovium) destroys underlying cartilage
- Tophi (pathognomonic of gout) - large aggregates of urate crystals in synovial membranes, articular cartilage, ligaments, tendons, and bursae; surrounded by foreign body giant cell reaction
Gouty nephropathy:
- Uric acid nephrolithiasis (kidney stones)
- Urate tophi in renal medullary interstitium/tubules → pyelonephritis risk
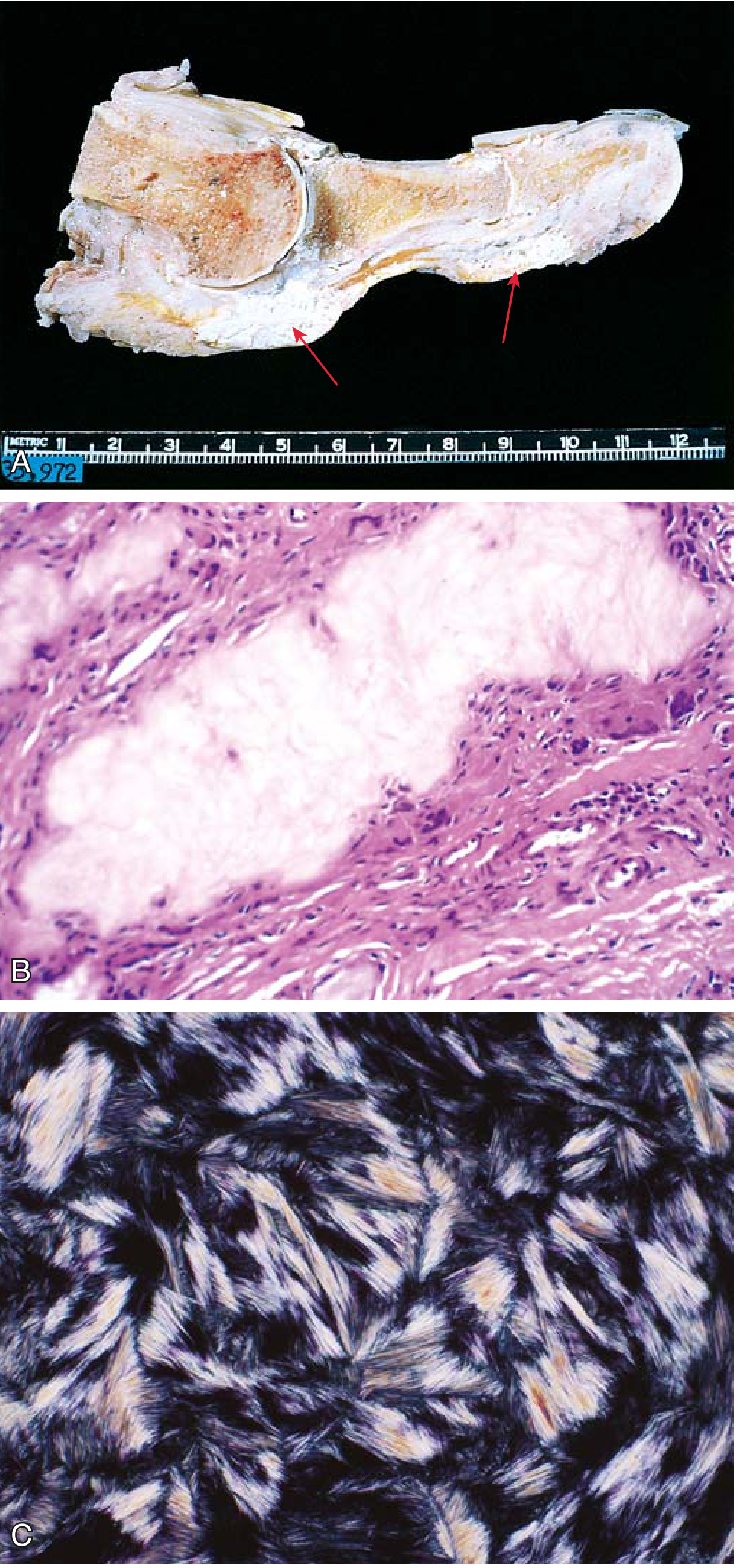
FIG. 19.40 - (A) Amputated great toe with tophi (red arrows) involving joint and soft tissues. (B) Gouty tophus: dissolved urate crystals surrounded by reactive fibroblasts, mononuclear cells, and giant cells (H&E). (C) Needle-shaped, negatively birefringent urate crystals under polarized light.
Clinical Stages (Four Recognized Stages)
| Stage | Features |
|---|---|
| 1. Asymptomatic hyperuricemia | Begins around puberty in men, after menopause in women; no symptoms |
| 2. Acute gouty arthritis | Sudden, excruciating monoarticular pain; localized hyperemia and warmth; 50% first attacks involve the 1st metatarsophalangeal (MTP) joint (podagra); self-resolving in hours to weeks without treatment |
| 3. Intercritical period | Symptom-free interval between attacks; without treatment, attacks recur more frequently and become polyarticular |
| 4. Chronic tophaceous gout | Develops ~10 years after first attack; juxtaarticular bone erosion, joint space loss, tophi visible in soft tissues |
Diagnosis
The gold standard is aspiration of synovial fluid (or tophus material) and identification of needle-shaped, negatively birefringent crystals under polarized light microscopy. Serum uric acid >6.8 mg/dL supports the diagnosis but is neither sensitive nor specific during an acute attack.
Treatment
| Goal | Agents |
|---|---|
| Acute attack - anti-inflammatory | NSAIDs (indomethacin), colchicine, systemic corticosteroids |
| Urate-lowering - reduce production | Xanthine oxidase inhibitors: allopurinol, febuxostat |
| Urate-lowering - increase excretion | Uricosuric drugs: probenecid, benzbromarone |
| Lifestyle modification | Weight loss, reduce alcohol, reduce dietary purines (red meat, organ meats, shellfish) |
Gout generally does not shorten life span but significantly affects quality of life.
Key Comparison: OA vs. Gouty Arthritis
| Feature | Osteoarthritis | Gouty Arthritis |
|---|---|---|
| Mechanism | Mechanical cartilage degeneration | Urate crystal-induced inflammation |
| Inflammation | Secondary/mild | Primary/intense (neutrophilic) |
| Demographics | Elderly; both sexes | Middle-aged men; post-menopausal women |
| Joint distribution | Weight-bearing + DIP/PIP fingers | 1st MTP joint (podagra); later polyarticular |
| Onset | Gradual, chronic | Sudden, episodic acute attacks |
| Crystal finding | None | MSU crystals - needle-shaped, negatively birefringent |
| Pathognomonic lesion | Osteophytes, bone eburnation | Tophi |
| Serology | Negative | Hyperuricemia (serum urate >6.8 mg/dL) |
| Joint fusion | No | No |
| Systemic involvement | No | Renal (nephrolithiasis, nephropathy) |
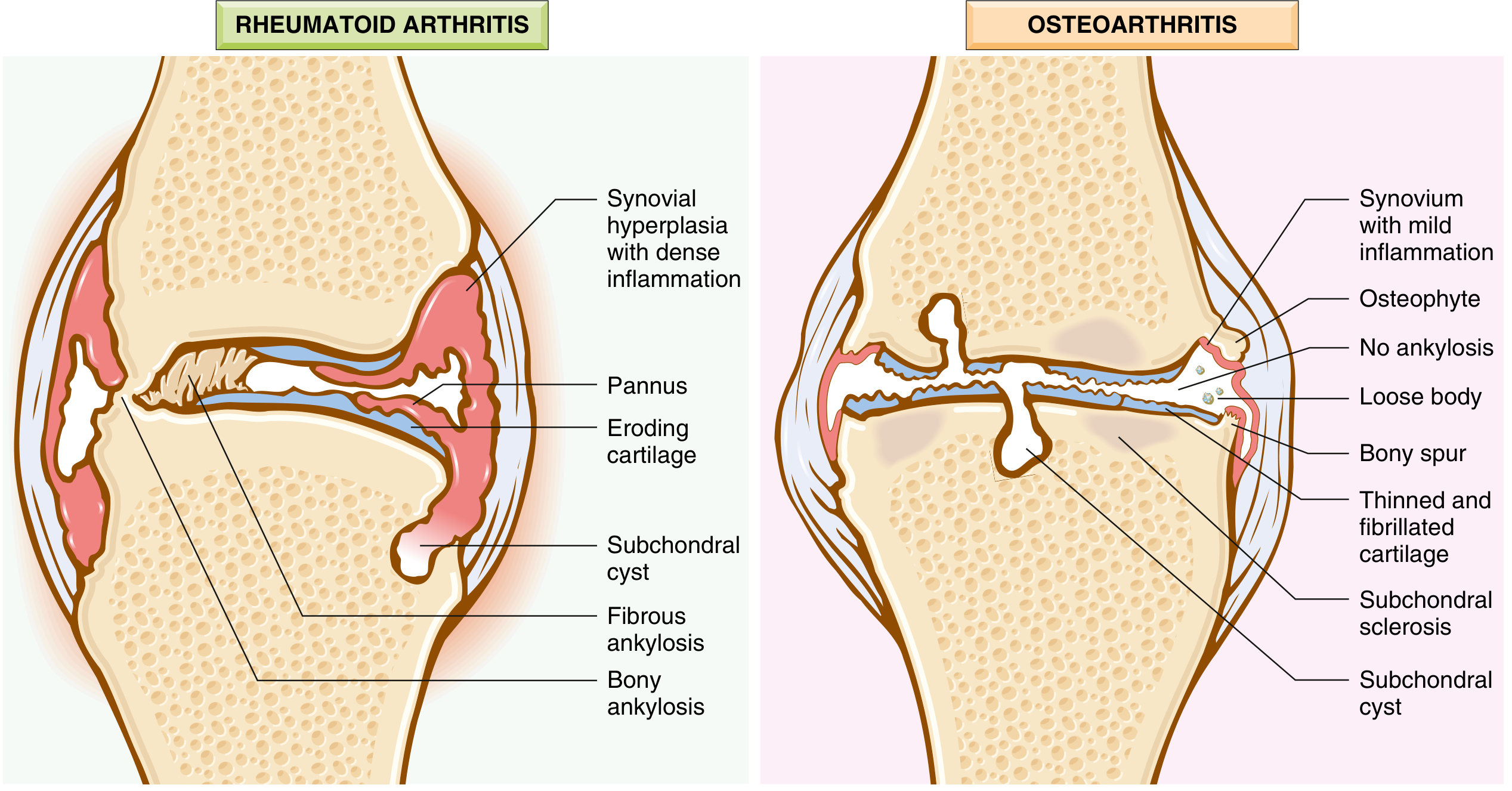
FIG. 19.33 - Joint morphology comparison. The OA panel (right) shows the classic features: osteophytes, loose bodies, thinned fibrillated cartilage, subchondral sclerosis and cysts, and only mild synovial inflammation - with no ankylosis.
Sources: Robbins & Kumar Basic Pathology, 10th ed., Chapter 19 (Joint Diseases)
This is a shared conversation. Sign in to Orris to start your own chat.