Explain me muscles from the topic of anatomy of musculoskeletal system for mbbs first year. Your explanation/notes should be useful for midterms and finals
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have all the information I need to write comprehensive MBBS first-year notes on muscles. Let me compose the full, exam-ready answer.
Muscles - Anatomy of the Musculoskeletal System
MBBS First Year - Exam Notes
1. CLASSIFICATION OF MUSCLE TYPES
The body has three types of muscle tissue, and knowing their differences is a classic MCQ/short answer topic:
| Feature | Skeletal Muscle | Cardiac Muscle | Smooth Muscle |
|---|---|---|---|
| Location | Attached to bones | Heart wall (myocardium) + large vessel roots | Walls of hollow organs, blood vessels, skin, eye |
| Control | Voluntary (somatic motor) | Involuntary (visceral motor) | Involuntary (visceral motor) |
| Appearance | Striated (striped) | Striated | Non-striated (smooth) |
| Cell structure | Long multinucleated fibers, parallel bundles | Branching network of individual cells linked electrically | Elongated/spindle-shaped fibers |
| Contraction | Powerful, fatigable | Less powerful than skeletal, fatigue-resistant | Slow, sustained |
| Innervation | Somatic + branchial motor nerves | Visceral motor nerves | Visceral motor nerves |
Exam tip: Skeletal muscle = somatic/voluntary = striated. Cardiac = visceral + striated (unique combo). Smooth = visceral + non-striated.
- Gray's Anatomy for Students, p. 41
2. NAMING OF SKELETAL MUSCLES
Muscles are named based on:
- Shape - e.g., rhomboid major, deltoid
- Attachments - e.g., sternohyoid (sternum + hyoid), brachioradialis
- Function - e.g., flexor pollicis longus, extensor carpi radialis
- Position - e.g., palmar interosseous, lateral pterygoid
- Fiber orientation - e.g., external oblique (fibers run obliquely), transversus abdominis
- Number of heads - e.g., biceps (2 heads), triceps (3), quadriceps (4)
- Size - e.g., gluteus maximus/medius/minimus
3. GROSS ANATOMY OF SKELETAL MUSCLE
A. Connective Tissue Coverings (High-yield!)
Each muscle has three layers of connective tissue - a common exam question:
| Layer | What it covers | Composition |
|---|---|---|
| Epimysium | Entire muscle belly | Dense irregular CT; merges with deep fascia |
| Perimysium | Individual fascicles (bundles of fibers) | Connective tissue; carries blood vessels + nerves |
| Endomysium | Individual muscle fibers (cells) | Delicate reticular fibers around each cell |
Memory trick: EPA - Epi wraps the whole (E = External), Peri wraps the packet (fascicle), Endo wraps each (individual fiber)
B. Tendons and Aponeuroses
- Tendon: Cord of dense fibrous CT connecting muscle to bone. Formed when epimysium/perimysium fuse at the muscle ends.
- Aponeurosis: Flat, sheet-like tendon (e.g., palmar aponeurosis, epicranial aponeurosis)
- At each end, the sarcolemma's outer coat fuses with tendon fibers; tendon fibers collect into bundles that connect to bone.
C. Attachments
- Origin: The proximal/fixed attachment - usually the less mobile bone
- Insertion: The distal/mobile attachment - the bone that moves
- Note: These are functionally defined and can reverse during movement (e.g., when doing pull-ups, the humerus is fixed and the body moves)
4. MICROSCOPIC ANATOMY OF SKELETAL MUSCLE FIBER
This is the most detailed section - expect questions in histology vivas and MCQs.
A. The Muscle Fiber (Cell)
- Diameter: 10-80 micrometers
- In most muscles, each fiber runs the entire length of the muscle
- Each fiber has only one nerve ending, located near the middle
- Cell membrane = sarcolemma (true plasma membrane + outer polysaccharide coat with collagen fibrils)
- Cytoplasm = sarcoplasm
B. Organizational Hierarchy (Smallest to Largest)
Myosin/Actin filaments → Sarcomere → Myofibril → Muscle fiber → Fascicle → Muscle
C. The Myofibril
Each muscle fiber contains hundreds to thousands of myofibrils. Each myofibril is made of:
- ~1,500 myosin filaments (thick, ~10-15 nm)
- ~3,000 actin filaments (thin, ~5-7 nm)
These interdigitate to produce the banding pattern (striation):
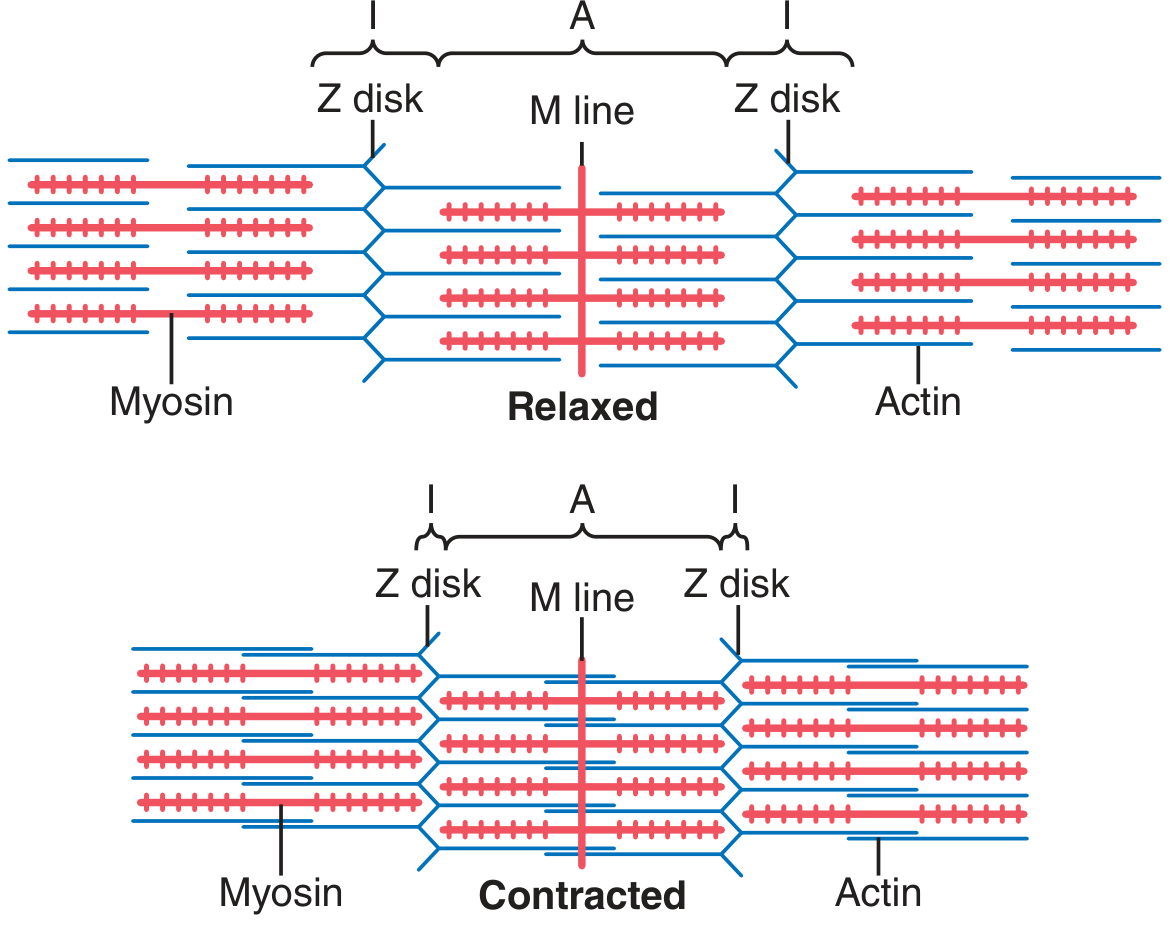
| Band/Line | What it is | Contains |
|---|---|---|
| A band (dark) | Anisotropic = dark in polarized light | Myosin + overlapping actin ends |
| I band (light) | Isotropic = light in polarized light | Actin only (no myosin) |
| Z disk/line | Bisects I band | Anchors actin filaments; boundary of sarcomere |
| M line | Bisects A band | Connects myosin tails; center of sarcomere |
| H zone | Central pale region within A band | Myosin only (no overlapping actin) - disappears during contraction |
Memory trick for bands: "I like icing (I = actin only, pale), A band has All (both actin and myosin)"
D. The Sarcomere
- Definition: The functional unit of muscle contraction
- The segment of myofibril between two successive Z disks
- At rest: ~2.0-2.5 micrometers long
- At maximum contraction: actin filaments completely overlap myosin, ~2.0 µm
- Z disks connect myofibrils to each other across the fiber
E. Important Proteins (High-yield for biochemistry overlap!)
| Protein | Filament | Function |
|---|---|---|
| Myosin | Thick | Motor protein; ATPase heads form cross-bridges with actin |
| Actin | Thin | Binds myosin cross-bridge during contraction |
| Tropomyosin | Thin | At rest, blocks actin-myosin binding sites |
| Troponin (I, T, C) | Thin | Troponin C binds Ca2+; lifts tropomyosin off actin |
| Titin (Connectin) | Elastic | MW ~3.9 million Da - one of the largest proteins in the body; holds myosin in place, acts as spring |
| Alpha-actinin | Z disk | Anchors actin to Z disk |
F. T-Tubule and Sarcoplasmic Reticulum
- T-tubules = extensions of the sarcolemma; penetrate deep into the fiber around each myofibril
- Sarcoplasmic reticulum (SR) = modified ER; surrounds myofibrils; stores Ca2+
- Terminal cisternae = enlarged ends of SR; closely associated with T-tubules
- Together: form the triad (one T-tubule flanked by two terminal cisternae)
- Function: T-tubules conduct action potentials to the interior; SR releases Ca2+ to trigger contraction
5. SLIDING FILAMENT MECHANISM OF MUSCLE CONTRACTION
This is one of the most important concepts - tested in both anatomy and physiology papers.
Steps (must know in order):
- Motor nerve action potential arrives at neuromuscular junction (NMJ)
- Acetylcholine (ACh) is released from nerve terminal
- ACh opens nicotinic ACh-gated cation channels (Na+ rushes in)
- Local depolarization → opens voltage-gated Na+ channels → muscle action potential
- Action potential travels along sarcolemma and down T-tubules
- T-tubule depolarization → Ca2+ release from sarcoplasmic reticulum
- Ca2+ binds Troponin C → conformational change → tropomyosin shifts, exposing actin's myosin-binding sites
- Myosin cross-bridges attach to actin → power stroke (myosin head bends, pulls actin toward M line)
- ATP binds myosin → cross-bridge detaches
- ATP hydrolysis → myosin re-cocks for next stroke
- Actin filaments slide inward → Z disks pulled together → sarcomere shortens → muscle contracts
- Ca2+ pumped back into SR by Ca2+-ATPase pump → troponin-tropomyosin re-blocks actin → muscle relaxes
What changes and what doesn't during contraction (classic MCQ):
- A band length = constant (myosin length unchanged)
- I band = shortens (actin moves deeper into A band)
- H zone = disappears (actin fully overlaps myosin)
- Sarcomere length = shortens
6. MUSCLE FIBER TYPES (Type I vs Type II)
A frequently tested topic, especially regarding endurance vs power athletes.
| Feature | Type I (Slow Twitch / "Red") | Type II (Fast Twitch / "White") |
|---|---|---|
| Speed | Slow twitch (~100 ms) | Fast twitch (~30 ms) |
| Metabolism | Oxidative (aerobic) | Glycolytic (anaerobic) |
| Fatigue | Fatigue slowly | Fatigue rapidly |
| Myoglobin | Rich (gives red color) | Scant |
| Mitochondria | Abundant | Few |
| Glycogen | Little (PAS-negative) | Abundant (PAS-positive) |
| Vascularization | Highly vascularized | Less vascularized |
| Motor unit size | Large (several thousand fibers) | Small (<100 fibers) |
| Function | Postural muscles; endurance | Phasic muscles; explosive/power |
| Athletes | Long-distance runners, cyclists, rowers | Sprinters, weight lifters, jumpers |
| Subtype IIA vs IIB | - | IIA = intermediate; IIB = purely glycolytic |
Key principle: The fiber type of a motor unit is determined by the innervating neuron - all fibers in one motor unit are the same type.
Plasticity: Muscle fiber type is genetically determined but can be influenced by training (exercise shifts type IIB toward IIA and even type I characteristics).
Postural muscles (Type I dominant): prone to shortening with increased resting tonus - require regular stretching.
Phasic muscles (Type II dominant): prone to weakening with disuse.
- THIEME Atlas of General Anatomy and Musculoskeletal System, p. 61
7. ARCHITECTURE / SHAPES OF SKELETAL MUSCLES
The arrangement of muscle fascicles (pennation) determines force generation and range of motion:
| Type | Fascicle arrangement | Example | Feature |
|---|---|---|---|
| Parallel (strap) | Parallel to long axis | Sartorius, sternohyoid | Long range of motion |
| Fusiform | Spindle-shaped, parallel fibers | Biceps brachii | Good range of motion + force |
| Unipennate | Fibers on one side of tendon | Extensor digitorum longus | More fibers = more force |
| Bipennate | Fibers on both sides of tendon | Rectus femoris | Greatest force |
| Multipennate | Multiple pennate groups converging | Deltoid | Maximum force, reduced range |
| Circular (sphincteric) | Concentric rings | Orbicularis oculi, orbicularis oris | Closes openings |
Rule: More pennation = more fibers per unit length = more force but less range of motion
8. MUSCLE ACTIONS AND ROLES
Muscles rarely act alone - understand these roles for exam vivas:
| Role | Definition | Example |
|---|---|---|
| Agonist (prime mover) | Main muscle producing the movement | Biceps brachii in elbow flexion |
| Antagonist | Opposes the agonist; relaxes during movement | Triceps during elbow flexion |
| Synergist | Assists the agonist; may also neutralize unwanted movements | Brachialis assists biceps |
| Fixator (stabilizer) | Stabilizes proximal bone so agonist can act | Rotator cuff muscles stabilize glenohumeral joint |
9. NERVE SUPPLY OF MUSCLES
- Each skeletal muscle is innervated by a spinal nerve or its branch
- Contains motor (efferent) and sensory (afferent) fibers
- Motor nerve fibers: alpha motor neurons → innervate extrafusal fibers (main contraction); gamma motor neurons → innervate intrafusal fibers (muscle spindle)
- Sensory fibers: from muscle spindles (Ia, II afferents) and Golgi tendon organs (Ib afferents)
Neuromuscular Junction (NMJ)
- Located near the middle of each muscle fiber
- Motor end plate: specialized region of sarcolemma
- Neurotransmitter: Acetylcholine (ACh)
- Receptor: Nicotinic ACh receptor (ligand-gated Na+/K+ channel)
- ACh broken down by acetylcholinesterase in synaptic cleft
Clinical MCQ: Myasthenia gravis = autoantibodies against nicotinic ACh receptors → progressive muscle weakness. Suxamethonium (succinylcholine) = depolarizing neuromuscular blocker acts at NMJ.
10. MUSCLE ATTACHMENTS TO BONE
- Muscles attach to the periosteum of bone via tendon fibers
- Sharpey's fibers = collagen fibers of the tendon that penetrate into bone
- Where tendons cross joints, they are often protected by tendon sheaths (synovial sheaths) that reduce friction
- Sesamoid bones form within tendons where they cross bony prominences (e.g., patella in quadriceps tendon)
11. MUSCLE BLOOD SUPPLY
- Skeletal muscle is highly vascularized (especially type I fibers)
- Blood vessels enter via the perimysium and branch into capillaries within the endomysium
- Capillary beds open and close depending on metabolic demand
- Exercising muscle receives up to 80-90% of cardiac output (compared to 15-20% at rest)
12. CLINICAL CORRELATES (High-yield for exams!)
A. Muscle Paralysis
- Inability to move a muscle or group; may be associated with loss of sensation
- Causes: stroke (upper motor neuron), spinal cord injury, poliomyelitis (lower motor neuron), iatrogenic
- Long-term paralysis → secondary muscle wasting and atrophy
- Upper motor neuron (UMN) lesion: spastic paralysis, hyperreflexia, Babinski sign
- Lower motor neuron (LMN) lesion: flaccid paralysis, hyporeflexia, fasciculations, muscle wasting
B. Muscle Atrophy
- Wasting of muscle due to:
- Neurogenic: nerve damage (denervation atrophy - occurs rapidly)
- Disuse atrophy: prolonged immobilization; reversible with physiotherapy
- Myopathic: primary muscle disease (e.g., muscular dystrophy)
C. Muscle Hypertrophy
- Increase in muscle fiber diameter (not number - cells can't multiply)
- Testosterone causes hypertrophy of limb muscles
- Response to resistance training: myofibrils increase; protein synthesis up
D. Muscle Tears / Strains
- Range from small interstitial injury to complete muscle disruption
- Commonly occur in adductor longus, hamstrings, quadriceps, gastrocnemius
- Seen in athletes with sudden exertion
- MRI (inversion recovery sequence): shows edema in and around the muscle as high signal
- Treatment: RICE (Rest, Ice, Compression, Elevation); physiotherapy; surgical repair for complete tears
E. Rhabdomyolysis
- Massive breakdown of skeletal muscle → release of myoglobin into blood
- Myoglobin in urine → myoglobinuria (tea-colored urine)
- Can cause acute kidney injury (AKI)
- Causes: crush injury, extreme exercise, drugs (statins), seizures
F. Compartment Syndrome
- Increased pressure within a fascial compartment compresses muscle blood supply
- Results in ischemia → necrosis if untreated
- Classic signs: Pain (especially on passive stretch), Pressure increase, Paresthesias, Paralysis, Pallor
- Treatment: Emergency fasciotomy
13. MUSCLE STABILIZATION OF JOINTS
Key functional anatomy concept for clinical exams:
- Ankle joint (sagittal plane): stabilized mainly by triceps surae + tibialis anterior
- Knee joint: stabilized by quadriceps femoris (anterior), hamstrings (posterior)
- Hip joint (sagittal plane): stabilized by gluteal muscles (especially gluteus maximus)
- Hip joint (frontal plane): stabilized by gluteus medius and minimus - loss causes Trendelenburg sign
- Spine: stabilized by intrinsic back muscles (erector spinae group)
14. SUMMARY TABLE: QUICK REVISION
| Topic | Key Point |
|---|---|
| Muscle types | Skeletal = voluntary/striated; Cardiac = involuntary/striated; Smooth = involuntary/non-striated |
| CT layers | Epimysium > Perimysium > Endomysium |
| Functional unit | Sarcomere (Z disk to Z disk) |
| Bands: constant in contraction | A band stays same; I band + H zone shorten/disappear |
| Contraction trigger | Ca2+ from SR binds Troponin C → exposes actin sites |
| NMJ transmitter | Acetylcholine → Nicotinic receptor |
| Type I fibers | Slow, oxidative, fatigue-resistant; postural |
| Type II fibers | Fast, glycolytic, fatigue quickly; power |
| Agonist/Antagonist | Work as pairs; antagonist relaxes when agonist contracts |
| Motor unit | 1 motor neuron + all muscle fibers it innervates |
SOURCES
- Gray's Anatomy for Students - Muscular System chapter
- THIEME Atlas of General Anatomy and Musculoskeletal System - Section 5: The Muscles; Muscle fiber types
- Guyton and Hall Textbook of Medical Physiology - Chapters 6-7: Physiological Anatomy of Skeletal Muscle; Sliding Filament Mechanism
This is a shared conversation. Sign in to Orris to start your own chat.