Glomerular filtration Passive process Occurs through Paracellular spaces Spaces between podocytes Protein binding reduces GFR Podocytes contain negative charge Repels negative charge of basic drug o Basic drugs filtered less than acidic drugs Passive tubular reabsorption Lipid soluble drugs get reabsorbed Active tubular secretion Active process Require ATP Drug excreted into urine by transporters through pumps Protein binding increases secretion rate OATP transporter o Organic anion transport protein Excretes acidic drugs: Penicillins Probenecid inhibits OATP OCTP transporter Organic cation transport protein Excretes basic drugs: Tubocurare P-gp P-glycoprotein Excretes neutral drugs: Digoxin
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
I now have enough information from authoritative sources to provide a comprehensive review of the notes with corrections. Let me compile the full response.
Here is a thorough review of your notes on renal drug excretion. Several points are correct, but there are also significant errors that need correcting.
Renal Drug Excretion - Notes Review
Figure 2-5 from Goodman & Gilman's Pharmacological Basis of Therapeutics:
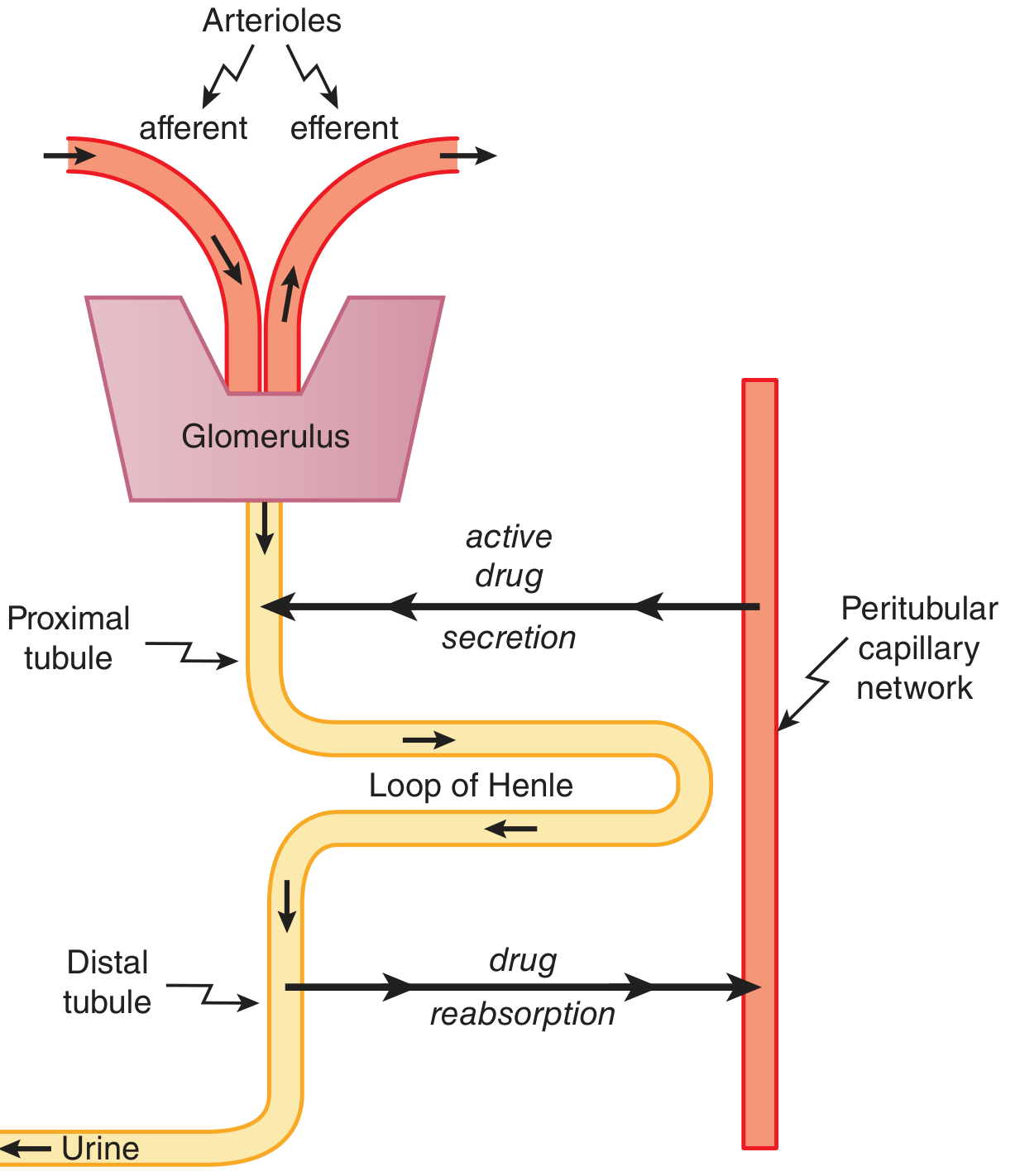
1. Glomerular Filtration
✅ Correct Points
- Passive process - correct. Filtration is driven by hydrostatic pressure, not energy expenditure.
- Protein binding reduces GFR (effectively) - correct. Only unbound (free) drug is filtered; protein-bound drug is too large to pass the filtration barrier.
- Podocytes contain negative charge - correct. The glomerular filtration barrier (GBM and podocyte glycocalyx) carries a strong negative charge.
❌ Errors to Correct
"Paracellular spaces / Spaces between podocytes"
This is incorrect on two counts:
-
The filtration route is transcellular through the filtration slits, not classically "paracellular." More precisely, filtrate passes through the fenestrations of the glomerular endothelium, then through the glomerular basement membrane (GBM), then through the filtration slits between podocyte foot processes (bridged by the slit diaphragm). The gaps between podocyte foot processes are the filtration slits - not generic "paracellular spaces."
-
Drugs do not filter primarily through the spaces between podocyte cell bodies. They pass through the three-layered filtration barrier: fenestrated endothelium → GBM → podocyte filtration slits. - (Comprehensive Clinical Nephrology, 7th Ed.)
"Podocytes repel negative charge of basic drugs; basic drugs filtered less than acidic drugs"
This is incorrect. The negative charge of the filtration barrier repels negatively charged (anionic/acidic) molecules, not basic ones. Most drugs are small enough that charge selectivity is more relevant for plasma proteins than for typical small-molecule drugs, but the principle is:
- Acidic drugs (which carry a negative charge at physiological pH) are repelled by the negatively charged barrier → filtered less than neutral or basic drugs
- Basic drugs (positively charged at physiological pH) are actually attracted toward the negatively charged membrane and face less charge-based resistance
Your notes have this backwards. The correct statement is: acidic drugs are filtered less (repelled by negative charge); basic drugs are filtered more (attracted by negative charge).
2. Passive Tubular Reabsorption
✅ Correct
- Lipid-soluble drugs get reabsorbed - correct. Non-ionized, lipophilic drugs passively diffuse back across the tubular epithelium from the filtrate into the peritubular capillaries. This is why converting a drug to polar/ionized form (e.g., by metabolic conjugation) is essential for renal clearance of lipophilic agents. - (Goodman & Gilman's, p. 51)
- The pH of the urine is also relevant: weak acids are ionized (and thus trapped in tubular urine) in alkaline urine, increasing excretion; the reverse applies for weak bases.
3. Active Tubular Secretion
✅ Correct Points
- Active process - correct.
- Drug excreted into urine by transporters - correct.
- Protein binding increases secretion rate - this is nuanced but directionally correct: unlike filtration, tubular secretion can handle protein-bound drug because the carrier proteins strip the drug from plasma proteins as free drug is removed; however, the net rate is still ultimately limited by the free fraction. This is a commonly tested point.
- Probenecid inhibits OAT (organic anion transporters) - correct, and used clinically to prolong penicillin levels.
- P-glycoprotein excretes digoxin - correct. Digoxin is eliminated by both glomerular filtration and tubular secretion via P-gp. - (Braunwald's Heart Disease)
❌ Errors to Correct
"OATP transporter"
The correct abbreviation for the renal organic anion transporter is OAT (Organic Anion Transporter), specifically OAT1 and OAT3. "OATP" (Organic Anion Transporting Polypeptide) is a different transporter family found primarily in the liver and intestine, not the kidney proximal tubule. This is a common source of confusion. - (Goodman & Gilman's, p. 51)
"OCTP transporter" for basic drugs
The correct name is OCT (Organic Cation Transporter), not "OCTP." The "P" does not belong here. The renal transporter for basic/cationic drugs is OCT2 (located on the basolateral membrane of proximal tubule cells). - (Katzung's Basic & Clinical Pharmacology, 16th Ed.)
"Tubocurare" as an example for OCT
Tubocurarine (tubocurare) is a large quaternary ammonium compound. It is primarily eliminated by biliary excretion and renal filtration, not predominantly by OCT-mediated secretion. Better classical examples for OCT substrates include metformin, amiloride, dopamine, histamine, and cimetidine.
"P-gp excretes neutral drugs"
P-glycoprotein is not selective for "neutral" drugs. It is an efflux pump that handles a broad range of substrates including large, hydrophobic, and often positively charged or amphipathic molecules. Digoxin is a good example (relatively neutral), but saying P-gp only handles "neutral drugs" is an oversimplification. P-gp substrates include digoxin, cyclosporine, loperamide, vinblastine, and many others. - (Katzung's, p. 2243)
Summary of Key Corrections
| Your Notes | Correct Version |
|---|---|
| Filtration occurs through "paracellular spaces" | Occurs through the 3-layer filtration barrier: fenestrated endothelium → GBM → podocyte filtration slits |
| Negative charge repels basic drugs; basic filtered less | Negative charge repels acidic (anionic) drugs; acidic drugs filtered less |
| OATP transporter secretes acidic drugs | OAT1/OAT3 (Organic Anion Transporter) - not OATP (which is hepatic) |
| OCTP transporter secretes basic drugs | OCT2 (Organic Cation Transporter) - drop the "P" |
| Tubocurare = OCT example | Better examples: metformin, cimetidine, amiloride |
| P-gp secretes "neutral" drugs | P-gp secretes large hydrophobic/amphipathic drugs (not restricted to neutral) |
Source: Goodman & Gilman's Pharmacological Basis of Therapeutics (Chapter 2, Renal Excretion); Katzung's Basic & Clinical Pharmacology 16th Ed.; Braunwald's Heart Disease; Comprehensive Clinical Nephrology 7th Ed.
Make summery in short
Renal Drug Excretion - Short Summary
3 Processes
| Process | Type | Key Point |
|---|---|---|
| Glomerular Filtration | Passive | Only free (unbound) drug filtered |
| Tubular Reabsorption | Passive | Lipid-soluble drugs reabsorbed |
| Tubular Secretion | Active (ATP) | Protein-bound drug CAN be secreted |
Glomerular Filtration
- Filtrate passes through: Endothelium → GBM → Podocyte filtration slits
- Negative charge repels acidic drugs (filtered less)
- Protein binding ↓ filtration
Tubular Secretion - Transporters
| Transporter | Drug Type | Example |
|---|---|---|
| OAT1/OAT3 | Acidic drugs | Penicillin, Furosemide |
| OCT2 | Basic drugs | Metformin, Cimetidine |
| P-gp | Large hydrophobic drugs | Digoxin |
- Probenecid inhibits OAT → slows penicillin excretion → prolongs drug effect
Key Corrections from Your Notes
- ❌ "OATP" → ✅ OAT (OATP is a liver transporter)
- ❌ "OCTP" → ✅ OCT
- ❌ "Basic drugs filtered less" → ✅ Acidic drugs filtered less
- ❌ "Tubocurare" for OCT → ✅ Metformin / Cimetidine
This is a shared conversation. Sign in to Orris to start your own chat.