What is the use of APL valve in Anesthesia Machine
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough, textbook-grounded answer on the APL valve:
APL (Adjustable Pressure-Limiting) Valve in the Anesthesia Machine
The APL valve - also called the "pop-off" valve or pressure relief valve - is an operator-adjustable relief valve that is one of the core safety components of the anesthesia breathing circuit.
Location in the Circuit
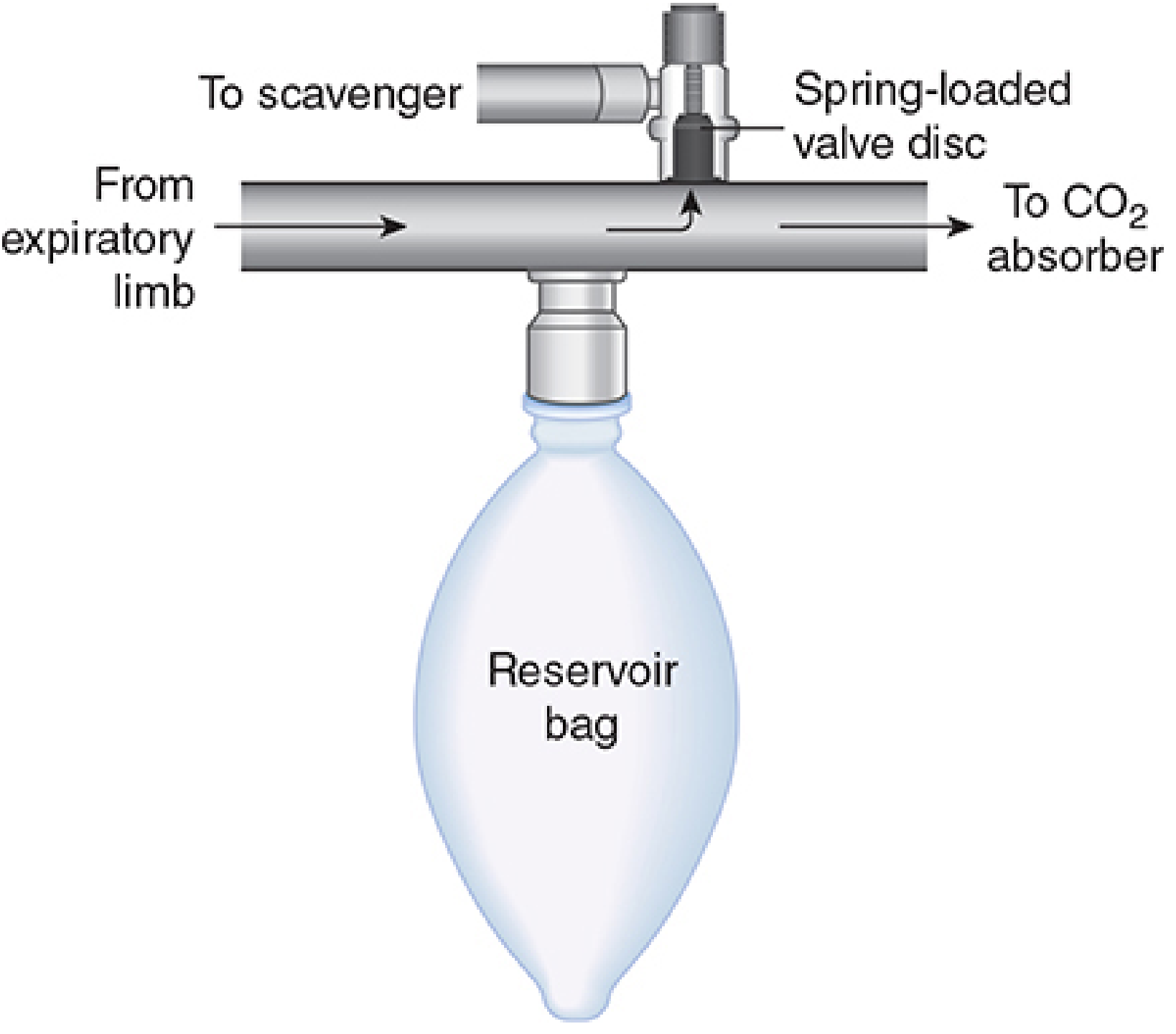
The APL valve is placed between the CO2 absorber and the expiratory valve, close to the reservoir bag (see diagram below). This position, before the absorber, helps conserve the absorber's capacity and minimizes the venting of fresh gas.
Primary Functions
1. Venting Excess Gas to the Scavenger
The APL valve regulates the flow of excess gas from the expiratory limb of the breathing circuit into the waste gas scavenging system. Without it, fresh gas continuously flowing from the flowmeters would build up pressure in a closed circuit. Waste-gas scavengers depend on the APL valve (and the ventilator spill valve) to receive vented gases, reducing operating room pollution that may pose a health hazard to surgical personnel. - Morgan & Mikhail's Clinical Anesthesiology, 7e
2. Controlling Breathing Circuit Pressure During Manual and Spontaneous Ventilation
The APL valve is the primary means of controlling airway/circuit pressure during bag (manual) ventilation and spontaneous breathing. By adjusting the spring tension on the control dial, the clinician sets the pressure at which the valve opens and vents gas. - Miller's Anesthesia, 10e
Mechanism of Action
The valve works on a spring-loaded disc principle (see diagram below):
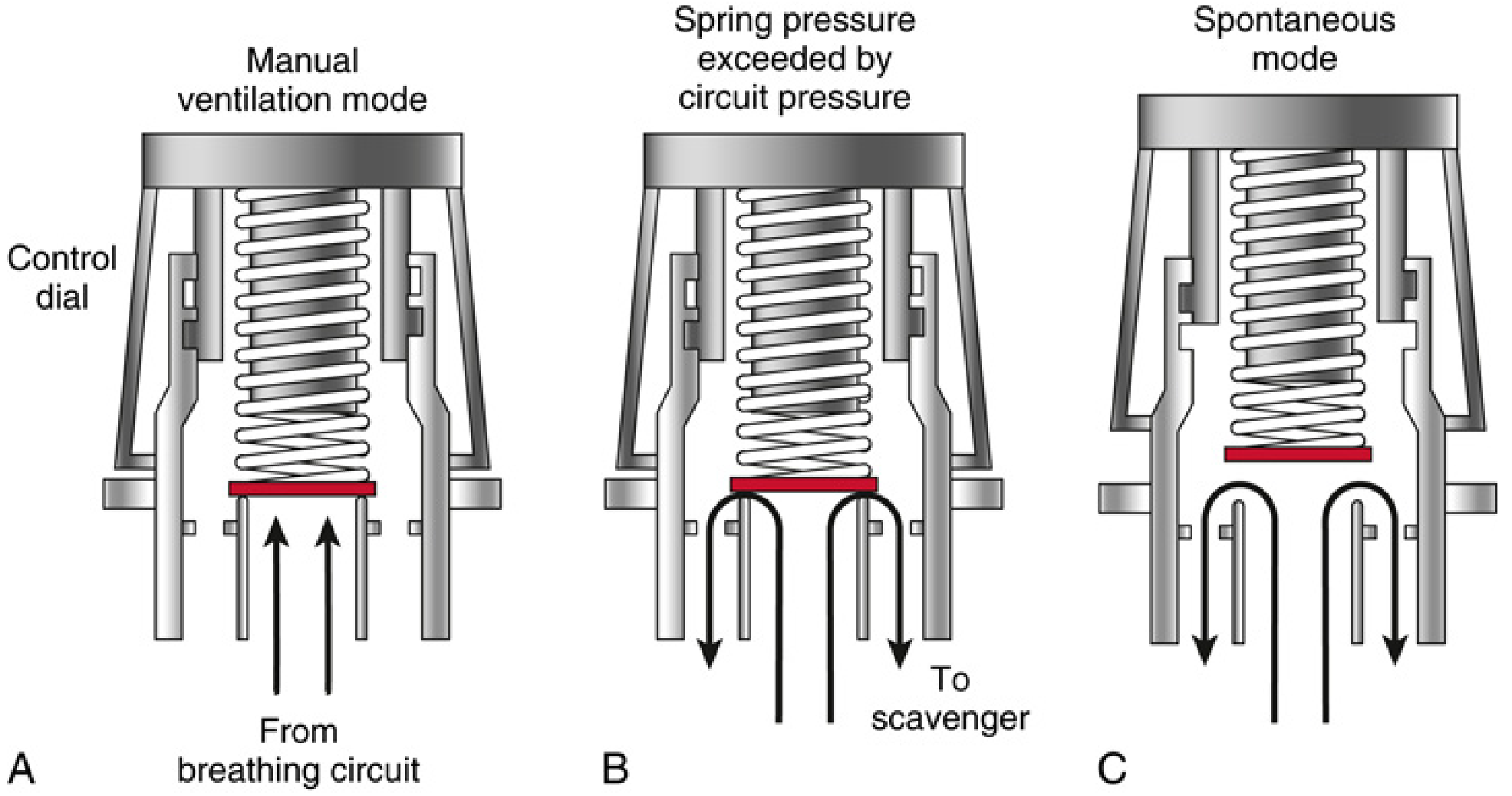
- (A) Manual ventilation mode: The operator tightens the control dial to increase spring tension, raising the threshold pressure at which gas can escape. The valve stays closed until circuit pressure exceeds the set value.
- (B) Spring pressure exceeded: When breathing circuit pressure rises above the set spring tension (e.g., during a bag squeeze), the disc lifts off the valve seat and excess gas vents to the scavenger.
- (C) Spontaneous mode: The control dial is opened fully - the disc is lifted off the seat entirely, allowing gas to flow freely to the scavenger with minimal resistance, so the patient can breathe spontaneously without effort against a partially closed valve.
In the pressure-regulating type, circuit pressure is independent of fresh gas flow rate. - Miller's Anesthesia, 10e
Modes of Ventilation and APL Behavior
| Mode | APL Valve Status |
|---|---|
| Spontaneous ventilation | Fully open (minimal resistance) |
| Manual (bag) ventilation | Partially closed - operator sets desired peak pressure |
| Mechanical ventilation | Excluded/isolated from the circuit (bag/ventilator switch turned to "ventilator") |
When the machine is switched to the ventilator mode, the APL valve is functionally removed from the circuit - either by a bag/ventilator selector switch or automatically on newer machines. The ventilator then uses its own internal spill valve (pneumatically closed during inspiration to allow positive pressure generation). - Morgan & Mikhail's Clinical Anesthesiology, 7e
Important Clinical Points
-
Oxygen flush hazard: Using the O2 flush valve during the inspiratory phase of mechanical ventilation must be avoided. At that moment, the ventilator spill valve is closed AND the APL is excluded - so the surge of oxygen (600-1200 mL/s) is delivered directly to the patient's lungs, risking barotrauma. - Morgan & Mikhail, 7e
-
Inadvertent closure: If the APL valve is accidentally left closed (fully tightened) during spontaneous or manual ventilation, pressure builds up in the circuit and can be transmitted to the patient's lungs. The reservoir bag provides some protection by its compliance characteristics but is not a substitute for proper APL valve management. - Miller's Anesthesia, 10e
-
Pre-use checklist: Standard anesthesia machine checkout requires confirming the APL valve is open before leaving the machine unattended (with selector on "Bag" mode). - Morgan & Mikhail, 7e
-
Valve malfunction: Mechanical failures (breakage, obstruction by gas-sampling line under the control knob) have been reported. Not all APL valves behave linearly - on certain machines, peak inspiratory pressure may routinely exceed the set value. Vigilant circuit pressure monitoring during manual ventilation is mandatory. - Miller's Anesthesia, 10e
-
Use in Mapleson circuits: APL valves are also a component of Mapleson semi-open circuits (A, B, C, D, E, F). Their position relative to the fresh gas inlet and reservoir bag determines circuit performance and rebreathing characteristics.
Summary
The APL valve has three core uses:
- Pressure relief - prevents dangerous pressure buildup in the circuit
- Pressure control - lets the clinician set the desired maximum circuit pressure during manual ventilation
- Scavenging interface - routes excess/waste anesthetic gases out of the circuit to the scavenging system
It is active only during bag/spontaneous mode and is bypassed during mechanical ventilation, when the ventilator's own spill valve takes over.
This is a shared conversation. Sign in to Orris to start your own chat.