Describe surgical anatomy of the liver. Discuss classification, pathophysiology, clinic features, investigations and treatment of liver trauma***** ➢ Discuss amoebic liver abscess, its complications and management** Refer bailey and love along with srb general surgery books draw hand writing diagram and flow charts wherever necessary
mkdir -p /home/daytona/workspace/liver-surgery && cat > /home/daytona/workspace/…
SURGICAL ANATOMY OF THE LIVER, LIVER TRAUMA & AMOEBIC LIVER ABSCESS
Sources: Bailey & Love's Short Practice of Surgery (28th Ed.), supplemented by SRB's Manual on Clinical Surgery. All content page-referenced below.
PART A: SURGICAL ANATOMY OF THE LIVER
1. Embryology
2. Ligaments and Peritoneal Reflections
| Ligament | From | To | Surgical Significance |
|---|---|---|---|
| Falciform ligament | Umbilicus | Anterior liver surface | Remnant of umbilical vein; divides left from right anteriorly |
| Left triangular ligament | Left lobe superior | Diaphragm | Division mobilises left lobe; exposes left IVC wall |
| Right triangular ligament | Right lobe | Right hemidiaphragm | Division allows left rotation of liver |
| Lesser omentum | Stomach/duodenum | Liver hilum | Right free edge = hepatoduodenal ligament (carries portal triad) |
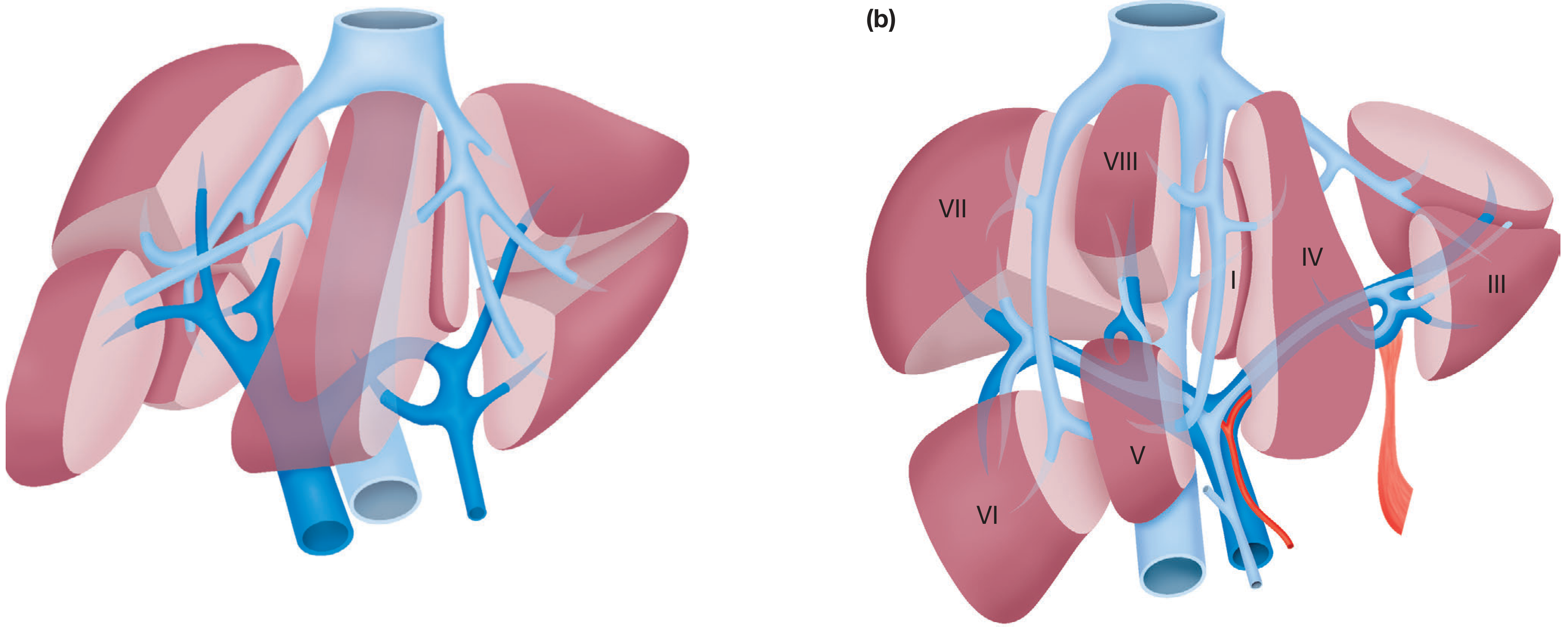
3. Segmental Anatomy (Couinaud's Classification)
┌─────────────────────────────────────────────────────────────────────┐
│ COUINAUD'S SEGMENTAL ANATOMY │
│ │
│ LEFT HEMILIVER │ RIGHT HEMILIVER │
│ (Segments I-IV) │ (Segments V-VIII) │
│ │ │
│ Seg I = Caudate lobe │ Seg V = Ant. inferior │
│ Seg II = L. lat. sup. │ Seg VI = Post. inferior │
│ Seg III = L. lat. inf. │ Seg VII = Post. superior │
│ Seg IV = L. medial │ Seg VIII= Ant. superior │
│ (quadrate lobe) │ │
│ │ │
│ ←——— Principal (Cantlie's) plane ———→ │
│ (IVC → gallbladder fossa; line of MHV) │
└─────────────────────────────────────────────────────────────────────┘
- Cantlie's line (principal plane): runs from gallbladder fossa to IVC; divides liver into true left and right halves
- The falciform ligament marks the surface boundary but NOT the true lobar division
- Hepatic veins run between segments; portal pedicles run within segments
4. Blood Supply
COELIAC TRUNK
|
┌──────────────────┐
Left gastric Common hepatic artery
|
┌──────────────────┐
Gastroduodenal Proper hepatic artery
|
┌───────────────────┐
Left hepatic A. Right hepatic A.
(Segments II,III,IV) (Segments V,VI,VII,VIII)
|
Cystic artery (to GB)
- Portal vein (80% of blood flow, 40-50% of oxygen): formed by confluence of splenic + superior mesenteric veins behind the neck of pancreas. Left branch has ~2 cm extrahepatic course.
- Hepatic artery (20% of blood flow, 50-60% of oxygen)
- Variants: Right hepatic artery may arise from SMA (passes behind bile duct, common in ~20%); left hepatic artery from left gastric (~20%)
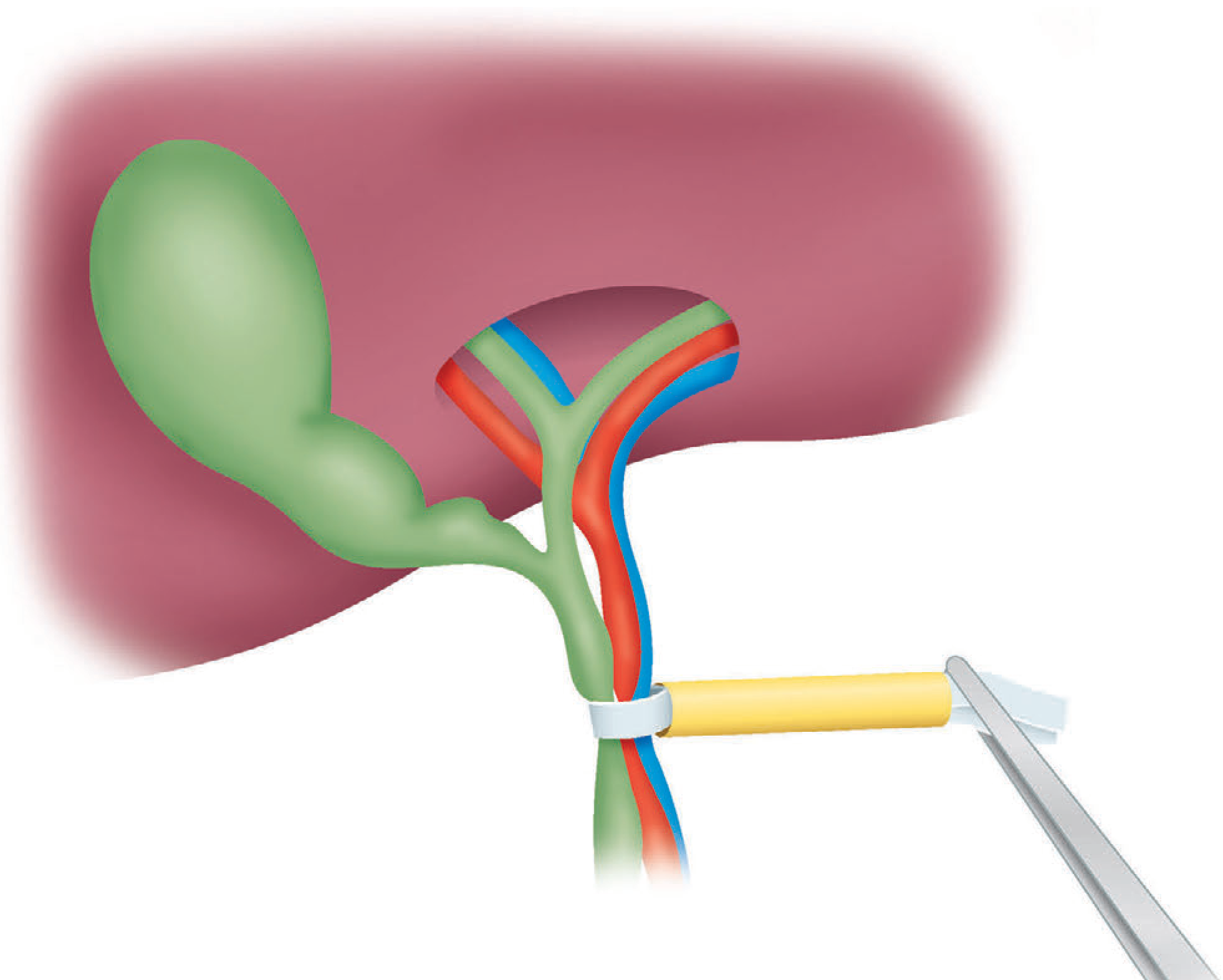
5. The Hilum (Porta Hepatis)
ANTERIOR VIEW OF PORTA HEPATIS
┌────────────────────────────────┐
│ BILE DUCT (right/anterolateral)│
│ HEPATIC ARTERY (left/medial) │
│ PORTAL VEIN (posterior) │
└────────────────────────────────┘
"Lady between two pillars"
(CBD lateral, HA medial, PV posterior)
6. Venous Drainage
- Right hepatic vein (Segs VI, VII)
- Middle hepatic vein (Segs IV, V, VIII) - runs in Cantlie's plane
- Left hepatic vein (Segs II, III)
7. Lymphatics and Nerve Supply
- Lymph drains to hepatic nodes at the porta hepatis, then to coeliac nodes and the thoracic duct
- Nerve supply: Sympathetic (T7-T10 via coeliac plexus) and parasympathetic (vagus nerve); hepatic stretching causes referred pain to the right shoulder (C4 dermatome via phrenic nerve)
PART B: LIVER TRAUMA
Classification (AAST Grading - American Association for Surgery of Trauma)
| Grade | Haematoma | Laceration/Vascular | Mortality |
|---|---|---|---|
| I | Subcapsular, <10% surface area | Capsular tear, <1 cm depth | <1% |
| II | Subcapsular 10-50%; intraparenchymal <10 cm | 1-3 cm depth, <10 cm length | 3-5% |
| III | Subcapsular >50%/ruptured; intraparenchymal >10 cm | >3 cm depth; bleeding contained | 10-15% |
| IV | — | 25-75% lobe disruption (1-3 Couinaud segs) | 25-50% |
| V | — | >75% lobe; juxtahepatic venous injury (IVC/major HV) | >50% |
Pathophysiology of Liver Trauma
MECHANISM OF INJURY
|
┌────┴────┐
BLUNT PENETRATING
(70-80%) (20-30%)
| |
RTA, falls, Stab, GSW
crush injury (lower chest/
upper abdomen)
|
▼
PARENCHYMAL DISRUPTION
┌─────────────────────────────────┐
│ Subcapsular haematoma │
│ Intraparenchymal haematoma │
│ Laceration (portal/hepatic veins)│
│ Biliary injury (bile leak) │
└─────────────────────────────────┘
|
▼
HAEMOPERITONEUM (most common → shock)
+ Bile peritonitis (if biliary)
+ Risk of secondary infection → abscess
Clinical Features
- Stab/gunshot wound to lower chest or upper abdomen
- Crush injury with multiple lower rib fractures (right 7-11)
- High-speed RTA (deceleration injury)
- Fall from height
- Right upper quadrant/epigastric pain, referred to right shoulder
- Abdominal distension (haemoperitoneum)
- Signs of shock: tachycardia, hypotension, pallor, cold extremities
- Peritonism if bile peritonitis
- Bruising/abrasion over right lower ribs/flank
- Tenderness in RUQ
- Guarding and rigidity (with peritoneal soiling)
- Shock (Hb may be normal initially due to haemoconcentration)
Investigations
- Bloods: FBC (Hb, platelets), cross-match 10 units, U&E, LFTs, clotting screen, glucose, amylase, ABG
- FAST (Focused Assessment with Sonography in Trauma): Rapid bedside USS to detect free fluid (haemoperitoneum); quick, non-invasive
- CT Abdomen + Chest with contrast (gold standard for stable patients): dual arterial/portal venous phase; grades injury, identifies active bleeding, biliary injury, associated injuries
- Diagnostic peritoneal lavage (DPL): used when CT not available; >100,000 RBC/mm³ = positive
- Angiography: for embolisation in active arterial bleeding identified on CT
- Laparoscopy: increasingly used for stable penetrating injuries
Management
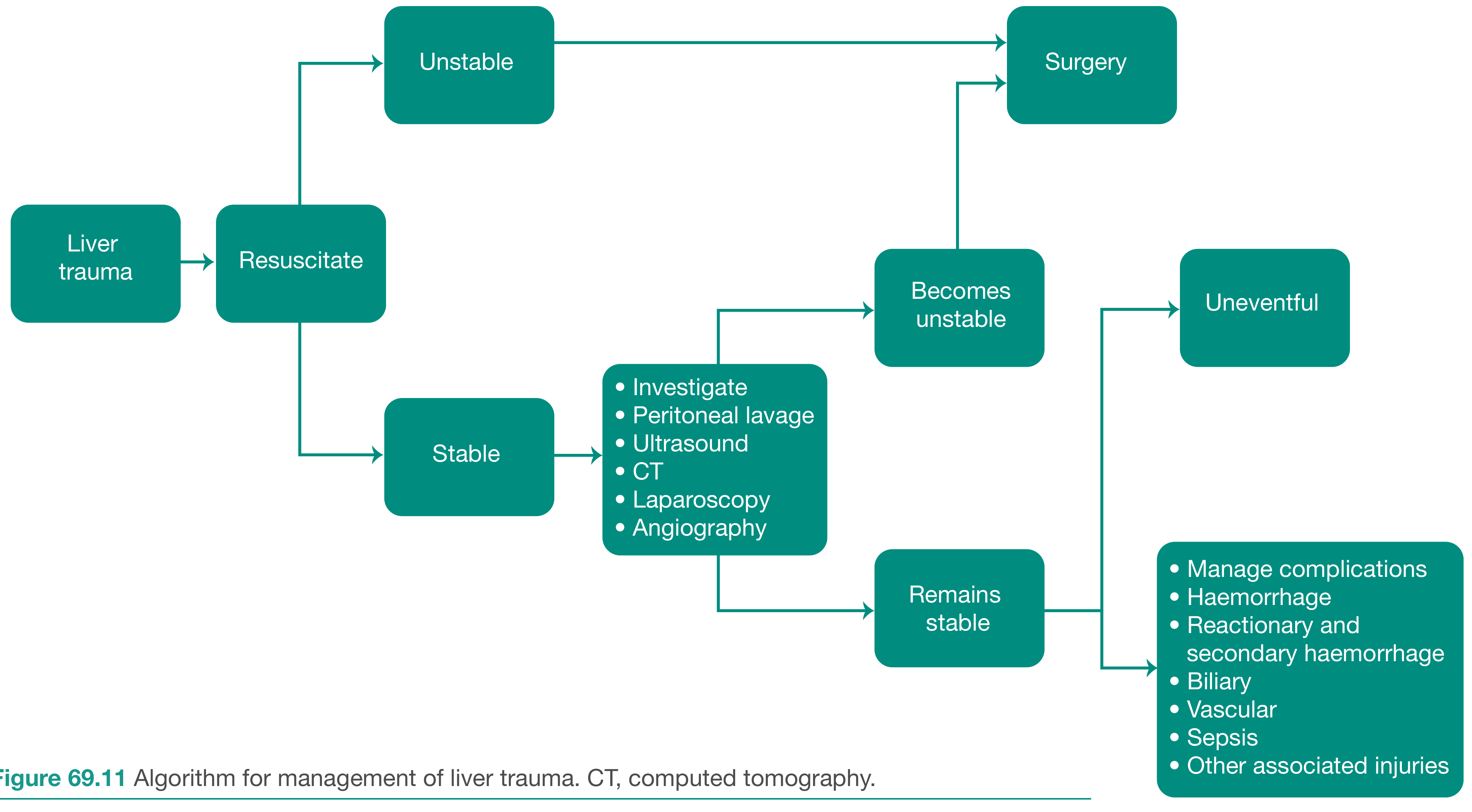
A. Initial Resuscitation (All Grades)
- Airway + oxygen
- Two large-bore IV cannulae; blood transfusion (not crystalloid as first choice)
- Intubate + ventilate if gas exchange inadequate
- Chest drain if haemothorax/pneumothorax
B. Non-operative Management (NOM) - Grades I-III, selected IV
- Haemodynamically stable, no peritonism, no other abdominal injury requiring surgery
- CT-confirmed injury grade
- Close monitoring in HDU/ICU with serial Hb
- Angioembolisation: indicated for CT evidence of active arterial bleeding in stable patient; highly effective for Grades II-IV
- Discharge after 8-10 days; avoid trauma; rescan at 6-8 weeks
- Prompt re-admission for fever, pain, or re-bleeding
C. Operative Management
DAMAGE CONTROL SEQUENCE
|
Step 1: PACKING
- Perihepatic packs around natural contour
- Manual compression
- Pringle manoeuvre if packing fails
|
Step 2: HAEMOSTASIS
- Suture lacerations (chromic catgut/PDS)
- Topical haemostatic agents (Surgicel, fibrin glue)
- Resectional debridement of necrotic tissue
- Hepatic artery ligation (if accessible)
|
Step 3: TEMPORARY ABDOMINAL CLOSURE
- Pack in situ, close abdomen
- Transfer to ICU; correct coagulopathy, hypothermia, acidosis
|
Step 4: RELOOK LAPAROTOMY (24-48 hours)
- Remove packs
- Definitive repair
- Anatomical resection if required
Complications of Liver Trauma
┌─────────────────────────────────────────────────┐
│ EARLY COMPLICATIONS │
│ │
│ • Recurrent haemorrhage (most common early) │
│ • Coagulopathy (dilutional, consumption) │
│ • Abdominal compartment syndrome (over-packing) │
│ • Sepsis / liver abscess │
│ • Bile peritonitis / biloma │
└─────────────────────────────────────────────────┘
┌─────────────────────────────────────────────────┐
│ LATE COMPLICATIONS │
│ │
│ • Haemobilia (arterio-biliary fistula) │
│ → Quincke's triad: RUQ pain + jaundice + │
│ melaena/haematemesis │
│ → Treat by angioembolisation │
│ │
│ • Hepatic artery aneurysm → rupture │
│ • Arterioportal fistula → portal hypertension │
│ • Arteriohepatic vein fistula → heart failure │
│ • Biliary stricture → obstructive jaundice │
│ (may require Roux-en-Y hepaticojejunostomy) │
│ • Hepatic insufficiency / liver failure │
└─────────────────────────────────────────────────┘
PART C: AMOEBIC LIVER ABSCESS (ALA)
Introduction
- Caused by Entamoeba histolytica (most pathogenic amoeba in humans)
- Common in Indian subcontinent, Africa, Central/South America - incidence up to 21/100,000 in South East Asia
- Mode of infection: faecal-oral route (contaminated food/water)
- Majority of infected individuals are asymptomatic carriers
- Commonest extraintestinal manifestation of amoebiasis
Pathogenesis (Flowchart)
INGESTION OF E. histolytica CYSTS
(contaminated food/water — faecal-oral route)
↓
SMALL INTESTINE → Excystation → Trophozoites
↓
COLON (caecum/ascending most affected)
→ Trophozoites invade submucosa
→ Flask-shaped ulcers
→ Bloody diarrhoea (only ~30% of ALA patients)
↓
PORTAL VEIN (via submucosal venules)
→ Trophozoites travel to LIVER
[SMV runs straight into Right portal vein
→ explains predilection for RIGHT LOBE: 70-80%]
↓
LIQUEFACTIVE NECROSIS of hepatocytes
(proteolytic enzymes + contact-mediated killing)
↓
ABSCESS CAVITY formed:
"Anchovy sauce" / chocolate-coloured pus
Odourless (sterile unless 2° infection)
Necrotic liver tissue + blood
Trophozoites in abscess WALL (minority of cases)
↓
If UNTREATED → RUPTURE
(peritoneum / right pleura / pericardium)
- Right lobe in 70-80% (streamlining of blood from SMV through portal vein into right lobe)
- Abscess location: high on diaphragmatic surface of right lobe (explains pulmonary symptoms)
- Single large abscess is more common than multiple abscesses
- Amoeboma: chronic granuloma in large bowel (usually caecum) from long-standing infection; can mimic carcinoma
Clinical Features
CLINICAL FEATURES OF ALA
┌──────────────────────────────────────────────────┐
│ EARLY (Non-specific): │
│ • Fever (high, swinging, with chills) │
│ • Anorexia, malaise, weight loss │
│ • Night sweats │
│ • Non-productive cough │
│ │
│ LATE (Specific): │
│ • Right upper quadrant pain │
│ • Right shoulder tip pain (diaphragmatic irrit.) │
│ • Hiccoughs (diaphragm irritation) │
│ │
│ EXAMINATION: │
│ • Toxic-looking, anaemic patient │
│ • Tender hepatomegaly │
│ • Tender/bulging intercostal spaces │
│ • Overlying skin oedema │
│ • Basal right pleural effusion + pneumonitis │
│ • Rarely: jaundice, ascites │
│ • Emergency presentation: abscess rupture │
└──────────────────────────────────────────────────┘
Investigations
- Anaemia (normochromic/normocytic)
- Leukocytosis (neutrophilia)
- Raised ESR, CRP
- Hypoalbuminaemia
- Deranged LFTs (especially elevated alkaline phosphatase)
| Test | Notes |
|---|---|
| IHA (Indirect Haemagglutination) | Very high sensitivity in non-endemic regions; remains elevated post-infection |
| ELISA | Most widely used; good sensitivity/specificity |
| Complement fixation | Older test |
| Counter-immunoelectrophoresis | Rapid but less sensitive |
| Antigen detection / PCR | Best specificity; limited by cost in endemic areas |
- Ultrasound (first-line): Hypoechoic/anechoic lesion with ill-defined borders; internal echoes suggest necrosis/debris
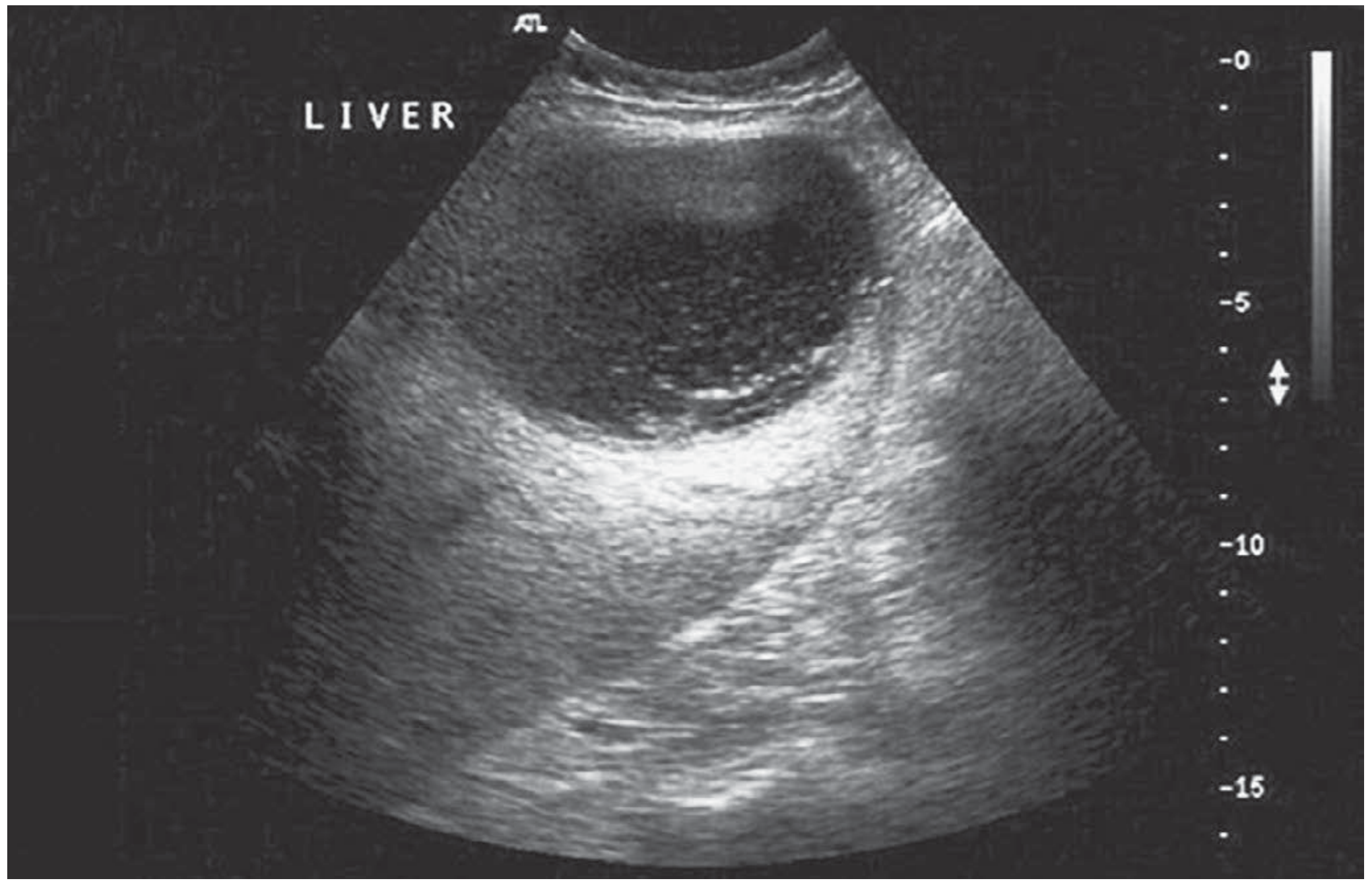
- CT scan (confirmatory + complications): Well-defined hypodense lesion with peripheral rim enhancement; can show chest extension
Complications of ALA
COMPLICATIONS OF AMOEBIC LIVER ABSCESS
┌──────────────────────────────┐
│ RUPTURE │
└──────┬─────────┬────────────┘
│ │ │
┌───────▼──┐ ┌────▼───┐ ┌───▼──────────┐
│PERITONEAL│ │PLEURAL │ │PERICARDIAL │
│ RUPTURE │ │RUPTURE │ │RUPTURE │
│(peritonitis│(empyema,│ │(MOST SERIOUS)│
│+ ascites)│ │hepato- │ │Tamponade │
│ │ │bronchial│ │→ mortality │
│ │ │fistula) │ │~30% │
└──────────┘ └─────────┘ └──────────────┘
Other complications:
• Secondary bacterial infection of abscess
• Inferior vena cava thrombosis
• Cerebral amoebic abscess (haematogenous spread)
• Amoeboma in large bowel
• Septicaemia
- Left lobe abscesses have a lower threshold for drainage due to propensity for pericardial rupture
- Right lobe abscesses may erode through diaphragm → empyema thoracis or hepatobronchial fistula (patient coughs up "chocolate sauce" sputum)
Management of Amoebic Liver Abscess
1. Medical Treatment (First-Line - Mainstay of Treatment)
- Metronidazole 800 mg TDS (three times daily) orally × 10 days - drug of choice
- OR Tinidazole 2 g once daily × 3-5 days (higher patient compliance)
- IV metronidazole if patient cannot tolerate oral
- Diloxanide furoate 500 mg TDS × 10 days (not effective against hepatic disease but prevents reinfection/relapse)
2. Aspiration / Drainage (Indications)
- Abscess not responding to IV metronidazole within 48-72 hours
- Risk of imminent rupture (large abscess, tense)
- Left lobe abscess (low threshold - risk of pericardial rupture)
- Abscess >10 cm diameter
- Secondary bacterial infection suspected
3. Surgical Treatment (Reserved for Complications)
INDICATIONS FOR SURGERY
• Rupture into peritoneal cavity → peritonitis
• Rupture into pleural cavity → empyema
• Rupture into pericardium → cardiac tamponade
• Severe colonic haemorrhage
• Toxic megacolon (rare)
• Amoeboma not responding to medical treatment
(to exclude malignancy)
SURGICAL PRINCIPLES:
Resuscitation → Drainage of cavity → Lavage
+ Vigorous IV metronidazole
(All managed in ICU if toxic megacolon/pericardial)
Summary: ALA vs Pyogenic Liver Abscess
| Feature | Amoebic (ALA) | Pyogenic (PLA) |
|---|---|---|
| Age/Sex | Young adult male | Middle-aged/elderly, either sex |
| Geography | Tropical/endemic | Worldwide |
| Organism | E. histolytica | E. coli, Klebsiella, Streptococcus milleri |
| Number | Usually single, large | Often multiple |
| Lobe | Right lobe 70-80% | Right lobe (biliary source) |
| Pus | "Anchovy sauce", sterile | Foul-smelling, creamy yellow |
| Source | Portal (gut amoebiasis) | Biliary (35%), portal (20%), cryptogenic (10%) |
| Serology | IHA/ELISA positive | Negative |
| Treatment | Metronidazole (medical) | Antibiotics + drainage |
| Prognosis | Excellent with Rx | Depends on underlying cause |
Quick-Reference Flowcharts (Visual Diagrams)
diagrams
HTML File · HTML
KEY EXAM POINTS (Marked with ★)
Create image with hand writing notes like above topics
Handwritten medical student notes on ruled paper with a slightly yellow tint, blue and black ink, titled "SURGICAL ANATOMY OF THE LIVER" at the top underlined twice in blue. Content includes: heading "Embryology" - liver bud from foregut diverticulum at 3-4 weeks gestation, hepatoblasts invade septum transversum. Heading "Ligaments" with a small hand-drawn table listing: Falciform (umbilical vein remnant, anterior wall), Left triangular (divides to expose IVC), Right triangular (fixes right lobe to diaphragm), Lesser omentum (right free edge = hepatoduodenal lig). Heading "Blood Supply" with a hand-drawn branching diagram: Coeliac trunk → Common hepatic artery → Proper hepatic → splits into Left HA and Right HA. Note: Portal vein = 80% flow, Hepatic artery = 20% flow. Small labeled sketch of porta hepatis cross-section showing CBD (right), HA (medial), PV (posterior) with label "Lady between two pillars". Messy authentic student handwriting with some words underlined, arrows, and small stars next to important points. Slight paper texture.
Handwritten medical student notes on lined paper, blue and black pen, heading "COUINAUD'S SEGMENTAL ANATOMY" underlined in red. Contains a hand-drawn diagram of the liver from front view, divided into 8 segments labeled with Roman numerals I through VIII. The liver is roughly oval shaped, divided by dotted lines. Left hemiliver labeled (I, II, III, IV) and right hemiliver (V, VI, VII, VIII) with a vertical dashed line labeled "Cantlie's line / Principal plane (IVC to GB fossa)". Small box on side: "Seg I = Caudate lobe (posterior), II = L.lat.sup, III = L.lat.inf, IV = Quadrate (L.medial), V = Ant.inf right, VI = Post.inf right, VII = Post.sup right, VIII = Ant.sup right". Arrow labeled "Falciform lig (surface only - NOT true lobar division)". Below: "Each segment = independent portal triad + hepatic vein branch → Safe anatomical resection". Star symbol next to key facts. Authentic messy student handwriting, slight paper yellowing.
Handwritten medical student surgery notes on ruled paper with blue and black ink. Page title "LIVER TRAUMA" double underlined in red. Section "AAST GRADING" with a hand-drawn table with 3 columns (Grade, Haematoma, Laceration/Vascular). Rows: Grade I - subcapsular less than 10%, capsular tear less than 1cm; Grade II - subcapsular 10-50%, intraparenchymal less than 10cm, 1-3cm depth; Grade III - greater than 50% ruptured, intraparenchymal greater than 10cm, more than 3cm depth; Grade IV - 25-75% lobe disruption, 1-3 Couinaud segments; Grade V - greater than 75% lobe, juxtahepatic venous/IVC injury. Star next to Grade V: "highest mortality greater than 50%". Below: "Clinical features" list: RUQ pain, shoulder tip pain, haemoperitoneum signs, shock (tachy + hypotension). "Investigations" list: FAST USS (rapid), CT abdomen+chest with contrast (GOLD STANDARD), DPL if CT unavailable, Angiography for embolisation. Messy authentic handwriting, underlining, boxes around key terms.
Handwritten medical notes on slightly yellowed lined paper, blue and black pen. Page title "LIVER TRAUMA - MANAGEMENT" underlined. Contains a hand-drawn flowchart: Top box "LIVER TRAUMA" → arrow down → "RESUSCITATE (ATLS) - ABC, 2 large bore IV, cross-match 10 units". Diamond shape "Haemodynamic Status?" with two branches: LEFT branch labeled "UNSTABLE" in red → box "EMERGENCY LAPAROTOMY - Damage Control Surgery" → list "1. Packing, 2. Pringle manoeuvre, 3. Temporary closure → ICU, 4. Relook 24-48h". RIGHT branch labeled "STABLE" in green → box "Investigate: CT, USS, Angiography" → two sub-boxes "Remains stable: Non-operative management (NOM), discharge 8-10d, rescan 6-8wk" and "Becomes unstable → Surgery". Bottom section "PRINGLE MANOEUVRE" with tiny sketch: finger+thumb compressing hepatoduodenal ligament, note "Safe up to 60 min normal liver - occludes HA + PV". Star: "Complications - Haemobilia (Quincke's triad: RUQ pain + jaundice + GI bleed) → embolise". Authentic messy student handwriting.
Handwritten medical student notes on lined paper, blue and black ink with some red underlines. Title "AMOEBIC LIVER ABSCESS (ALA)" double underlined. Section "Pathogenesis" with a vertical flowchart drawn in hand: "Ingestion of E. histolytica cysts (faecal-oral route, endemic areas)" → arrow → "Small intestine: excystation → trophozoites" → arrow → "Colon: penetrate submucosa → flask-shaped ulcers → bloody diarrhoea (only 30%)" → arrow → "Portal vein → LIVER (SMV streamlines into RIGHT lobe)" → arrow → "Liquefactive necrosis → ABSCESS" → arrow → "ANCHOVY SAUCE pus: chocolate-coloured, odourless, sterile". Annotation bubble: "RIGHT lobe 70-80% (SMV streamlining)". Note in box: "Trophozoites in abscess WALL not in pus". Below: "Clinical Features" two columns Early (fever, night sweats, anorexia, malaise, cough) and Late (RUQ pain, right shoulder tip pain, hiccoughs, tender hepatomegaly, bulging intercostals, basal effusion). Star: "Typical = young adult male from endemic area". Authentic student handwriting.
Handwritten medical student notes on ruled paper, blue black and red pen. Title "ALA - INVESTIGATIONS & MANAGEMENT" underlined in red. Section "INVESTIGATIONS": list with small boxes - Bloods: anaemia, leukocytosis, raised ALP, ESR, CRP, hypoalbuminaemia. Serology table: IHA (very high sensitivity non-endemic), ELISA (most widely used), Antigen detection/PCR (best specificity). Imaging: USS = hypoechoic/anechoic lesion ill-defined borders (1st line), CT = hypodense with rim enhancement (confirmatory). Note: "Anchovy sauce pus on aspiration = diagnostic". Section "MANAGEMENT" flowchart: "1st LINE: MEDICAL" → box "Metronidazole 800mg TDS x 10 days (DRUG OF CHOICE) OR Tinidazole 2g OD x 3-5 days" → arrow → "THEN: Diloxanide furoate 500mg TDS x 10 days (luminal amoebicide - eradicates gut cysts)". Diamond "Response in 48-72h?" → YES → "Continue, 90-95% cure" and NO → "US-guided aspiration / pigtail catheter". Indications for aspiration starred: left lobe abscess, larger than 10cm, no response to Rx, risk of rupture. "SURGERY: reserved for RUPTURE - peritoneum/pleura/pericardium → drain+lavage+IV metro". Authentic messy handwriting.
Handwritten medical student notes on lined paper, blue and black ink. Title "ALA - COMPLICATIONS & COMPARISON" underlined. Section "Complications of ALA" with hand-drawn branching diagram: central box "RUPTURE" with three branches: 1. "PERITONEAL → peritonitis, ascites", 2. "PLEURAL (right) → empyema, hepatobronchial fistula (coughs up chocolate sputum)", 3. "PERICARDIAL (left lobe abscess) → cardiac tamponade, MOST SERIOUS mortality ~30%". Other complications listed: secondary bacterial infection, IVC thrombosis, cerebral abscess (haematogenous), septicaemia. Warning star: "Left lobe ALA → LOW threshold for drainage (pericardial risk)". Below: comparison table hand-drawn with columns "Feature | ALA | Pyogenic". Rows: Age (young male | middle-aged), Pus (anchovy sauce sterile | foul creamy yellow), Number (usually single | often multiple), Serology (IHA/ELISA +ve | negative), Treatment (metronidazole | antibiotics + drainage), Prognosis (excellent | depends on cause). Bottom box starred: "AMOEBOMA = chronic granuloma caecum, mimics carcinoma, treat medically then resect if persistent". Authentic student handwriting style.
400, message: Got more than 4194304 bytes when reading: b'data: {"candidates": [{"content": {"role": "model","parts": [{"inlineData": {"mimeType": "image/png"...'.
We encountered an error while processing your request. Please try again or reach out to us for help.