Give me answer on Pre operation evaluation of lung resection for md exam answer 10 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material from multiple authoritative textbooks. Let me compile the complete MD exam answer.
Pre-operative Evaluation of Lung Resection
(10-mark MD Exam Answer)
Introduction
Pre-operative evaluation before lung resection aims to identify whether a patient with "resectable" disease is also "operable" - i.e., can tolerate the proposed resection with acceptable risk. The evaluation follows a structured three-domain approach often called the "three-legged stool" of respiratory assessment:
- Lung mechanical function (spirometry)
- Pulmonary parenchymal function (gas exchange / DLCO)
- Cardiopulmonary reserve (exercise testing)
- Miller's Anesthesia, 10e (KEY POINTS)
I. History and Clinical Assessment
- Detailed history of quality of life gives the best functional assessment of respiratory reserve
- Establish smoking history - cessation >8 weeks pre-op reduces secretions and reactive airways
- Symptoms of dyspnea, exercise intolerance, hemoptysis, weight loss
- Comorbidities: COPD, IHD, hypertension, diabetes, renal disease
- Current medications (especially anticoagulants, beta-blockers, inhalers)
- Prior thoracic surgery, radiotherapy, chemotherapy
II. Cardiac Evaluation
Cardiac complications occur in 10-15% of thoracic patients. The Thoracic Revised Cardiac Risk Index (ThRCRI) is used, incorporating:
| Risk Factor | Score |
|---|---|
| Pneumonectomy planned | +1.5 |
| Prior ischemic heart disease | +1.5 |
| Prior stroke or TIA | +1.5 |
| Serum creatinine >2 mg/dL | +1 |
-
Patients with major cardiac risk factors require formal cardiology evaluation per ACC/AHA guidelines
-
ECG, echocardiogram where indicated
-
Coronary angiography/revascularization if significant CAD identified
-
Beta-blockers should be continued perioperatively if already prescribed
-
Mulholland and Greenfield's Surgery, 7e, p. 917-919
III. Respiratory Mechanical Function - Spirometry
All patients undergoing pulmonary resection must have baseline spirometry.
Key parameter: FEV1 (Forced Expiratory Volume in 1 second)
The predicted postoperative FEV1 (ppoFEV1) is calculated as:
ppoFEV1 = preoperative FEV1 × (1 - fraction of functional lung tissue removed)
- For lobectomy: segment counting method - ppoFEV1 = preop FEV1 × (1 - y/z) where y = functional segments removed, z = total functional segments
- For pneumonectomy: use V/Q scan - ppoFEV1 = preop FEV1 × (1 - fraction of total perfusion in resected lung)
Risk thresholds:
-
ppoFEV1 >60% predicted → Low risk
-
ppoFEV1 30-60% predicted → Moderate risk - proceed to exercise testing
-
ppoFEV1 <30% predicted → High risk - proceed to CPET; mortality risk >10%
-
Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 1039
IV. Gas Exchange - Diffusing Capacity (DLCO)
- DLCO (Diffusion Lung Capacity for Carbon Monoxide) reflects total functioning alveolar-capillary surface area
- ppoDLCO calculated the same way as ppoFEV1
Risk thresholds mirror FEV1:
-
ppoDLCO >60% → Low risk
-
ppoDLCO 30-60% → Moderate risk - exercise testing
-
ppoDLCO <30% → High risk - CPET mandatory
-
If both ppoFEV1 and ppoDLCO >60% - patient is at low risk and can proceed directly to surgery
-
Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 1039-1040
V. Cardiopulmonary Exercise Testing (CPET)
This is the gold standard for assessing cardiopulmonary interaction. It is indicated when ppoFEV1 or ppoDLCO is <60%.
Step-test / Stair Climb Test (SCT) - low-technology screening:
- Able to climb >22 metres (≈3 flights) → Low risk → can proceed
- Climb <22 metres → Proceed to formal CPET
Shuttle Walk Test (SWT):
-
400 metres → Low risk
- <400 metres → Formal CPET
Formal CPET - VO2 max (maximal oxygen consumption):
| VO2 max | Risk |
|---|---|
| >20 mL/kg/min (or >75% predicted) | Low risk - proceed |
| 10-20 mL/kg/min (or 35-75%) | Moderate risk - discuss alternatives |
| <10 mL/kg/min (or <35%) | High risk - major resection not recommended |
- Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 1039-1040
VI. ACCP Algorithm - Risk Stratification
The following algorithm (ACCP 2013 guidelines) guides decision-making:
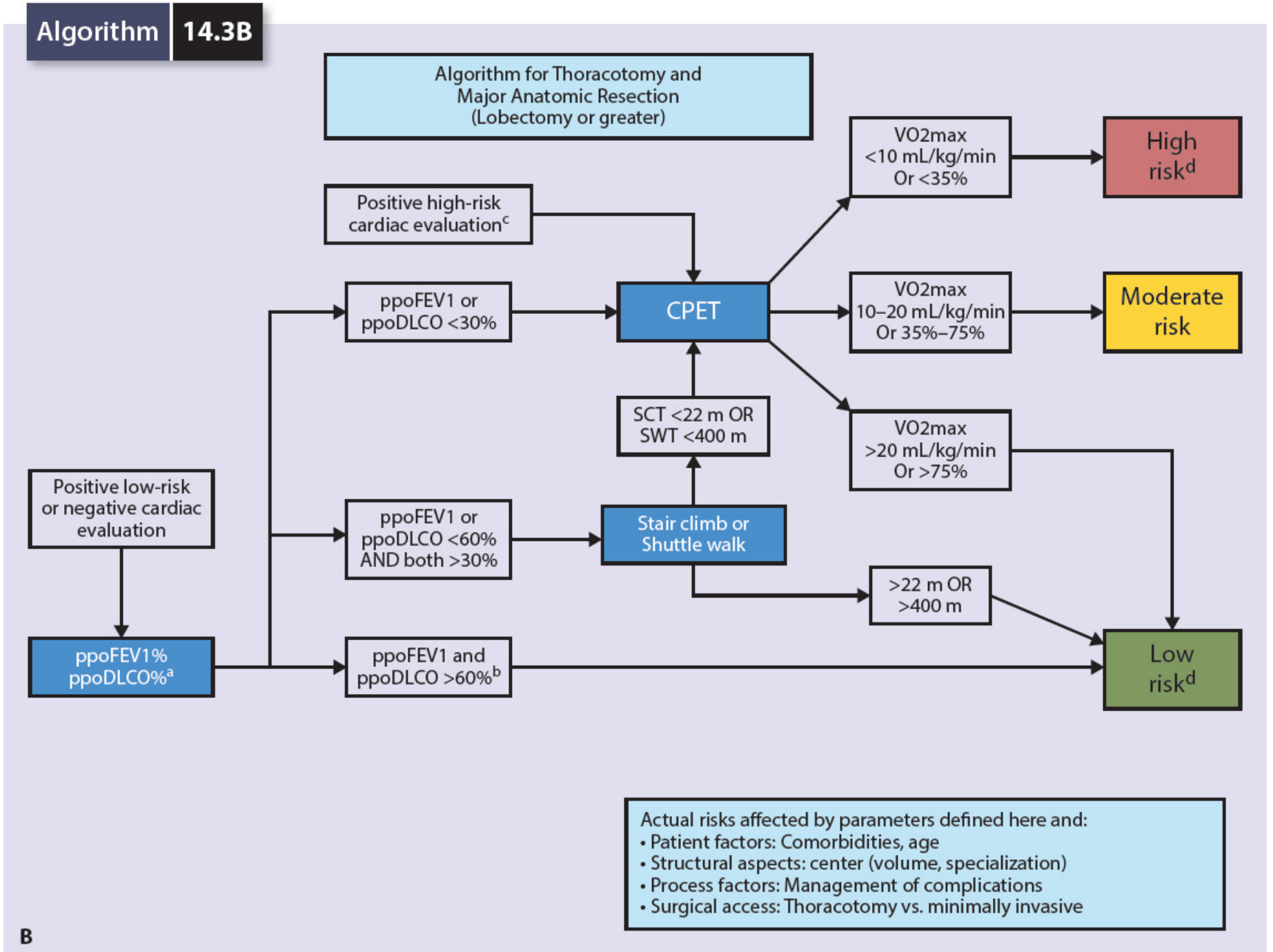
Algorithm 14.3B - Physiologic Evaluation prior to Lung Resection (ACCP guidelines, Mulholland & Greenfield Surgery 7e)
Risk definitions:
-
Low risk: Expected mortality <1%; major anatomic resection safe
-
Moderate risk: Morbidity/mortality variable; risks/benefits discussed with patient
-
High risk: Mortality after standard resection may exceed 10%; counsel for alternative surgical or nonsurgical options
-
Mulholland and Greenfield's Surgery, 7e, p. 917-919
VII. V/Q Scintigraphy
- Indicated particularly for pneumonectomy candidates with borderline function
- Provides the relative contribution of each lobe/lung to overall pulmonary function
- Allows calculation of split lung function to refine ppoFEV1 and ppoDLCO estimates
- Essential when there is doubt about whether a single remaining lung will be adequate
VIII. Additional Investigations
| Investigation | Purpose |
|---|---|
| Chest X-ray / CT Thorax | Staging, anatomy, pleural disease |
| ABG (Arterial Blood Gas) | Baseline PaO2/PaCO2, hypercapnia is a poor sign (PaCO2 >45 = high risk) |
| FBC | Anemia, polycythemia |
| LFT, RFT, Electrolytes | Organ function |
| Coagulation profile | Pre-thoracotomy baseline |
| Echocardiography | Ventricular function, pulmonary hypertension |
| Bronchoscopy | Central airway assessment, tumor involvement |
IX. Specific Risk Factors
Age: Age alone is not a contraindication. Preoperative exercise capacity is the best predictor of outcome in elderly patients. Geriatric patients have high risk for post-thoracotomy arrhythmias (AF occurs in up to 30-50% after major resections, peaking on day 2).
Post-operative Atrial Fibrillation risk factors:
- Male >55 years, resting HR >72 bpm, pneumonectomy (60% AF) > lobectomy (40%)
- Prophylaxis: diltiazem (drug of choice), amiodarone, magnesium, statins
COPD: Bronchodilator therapy should be optimized pre-operatively. VATS approach significantly reduces respiratory complications in patients with underlying lung disease.
- Miller's Anesthesia, 10e, p. 7086
X. Interventions to Reduce Risk
The following are evidence-based pre-operative interventions that reduce respiratory complications:
- Smoking cessation (minimum 8 weeks before surgery)
- Pre-operative physiotherapy and incentive spirometry
- Inspiratory muscle training (Hulzebos et al. - reduces post-op complications)
- Bronchodilator optimization in COPD
- Treatment of respiratory infections before elective surgery
- Nutritional optimization
- Planning for thoracic epidural analgesia (shown to reduce respiratory complications post-operatively)
- Consideration of VATS or minimally invasive approach in high-risk patients
- Miller's Anesthesia, 10e (KEY POINTS); Mulholland & Greenfield's Surgery 7e
Summary Table
| Parameter | Low Risk | Moderate Risk | High Risk |
|---|---|---|---|
| ppoFEV1 | >60% | 30-60% | <30% |
| ppoDLCO | >60% | 30-60% | <30% |
| VO2 max | >20 mL/kg/min | 10-20 | <10 mL/kg/min |
| Stair climb | >22 m | - | <22 m |
| Shuttle walk | >400 m | - | <400 m |
| Expected mortality | <1% | Variable | >10% |
Conclusion
Pre-operative evaluation before lung resection is a stepwise, multidisciplinary process. The three pillars - spirometry (FEV1), gas exchange (DLCO), and exercise capacity (CPET/stair climbing) - together stratify patients into low, moderate, and high risk. Predicted postoperative values (ppoFEV1 and ppoDLCO) are central to decision-making. Cardiac evaluation via the ThRCRI runs in parallel. High-risk patients should be counseled about lung-sparing alternatives (segmentectomy, VATS) or nonsurgical treatment. Preoperative optimization with smoking cessation, physiotherapy, and bronchodilator therapy can shift borderline patients to a safer operative category.
Key Sources:
- Miller's Anesthesia, 10e - Ch. 49 (Thoracic Anesthesia)
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Ch. 25 (Thoracic Anesthesia)
- Mulholland and Greenfield's Surgery, 7e - Algorithm 14.3 (ACCP 2013 Guidelines)
- Fishman's Pulmonary Diseases and Disorders
This is a shared conversation. Sign in to Orris to start your own chat.