hernia(elaborate)
Reading File
Finding Sources
Searching PubMed
"hernia"[MeSH Terms] AND "repair"[MeSH Terms]
Searching Images
inguinal hernia anatomy types diagram
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full elaborated response.
Hernia — Comprehensive Overview
Definition
A hernia is the protrusion of a viscus, or part of a viscus, through the wall of the cavity that normally contains it. The hernial contents pass through a defect in the containing wall (the hernial orifice), traverse a passage (the hernial canal if present), and emerge as a hernial sac covered by whatever layers the abdominal wall provides at that point.
Anatomy of a Hernia
Every hernia has three structural components:
- The sac — a pouch of peritoneum lined with serous membrane; has a neck, body, and fundus
- The sac contents — typically omentum, small bowel, or large bowel; occasionally bladder, ovary, or Meckel's diverticulum
- The coverings — layers of the abdominal wall that cover the sac as it protrudes
Classification
By Reducibility
| Status | Description |
|---|---|
| Reducible | Contents can spontaneously or manually return to the cavity |
| Irreducible / Incarcerated | Contents cannot be returned; does not necessarily imply ischemia |
| Obstructed | Bowel lumen inside the sac is occluded, causing intestinal obstruction |
| Strangulated | Blood supply to the hernial contents is compromised — a surgical emergency |
| Richter's hernia | Only the antimesenteric wall of the bowel is caught; partial lumen obstruction; can strangulate without complete bowel obstruction |
Strangulation occurs when any degree of ischemia results from compression of bowel within the neck of a hernia. The risk is inversely related to neck size — femoral hernias have the smallest neck and strangulate in up to 45% of cases, whereas incisional hernias strangulate in only ~2%. — Sleisenger & Fordtran's GI and Liver Disease
By Origin
- Congenital — e.g., indirect inguinal hernia from patent processus vaginalis, congenital diaphragmatic hernia
- Acquired — due to weakness of the abdominal wall from aging, obesity, pregnancy, chronic cough, ascites, prior surgery
Sites of Abdominal Wall Hernias
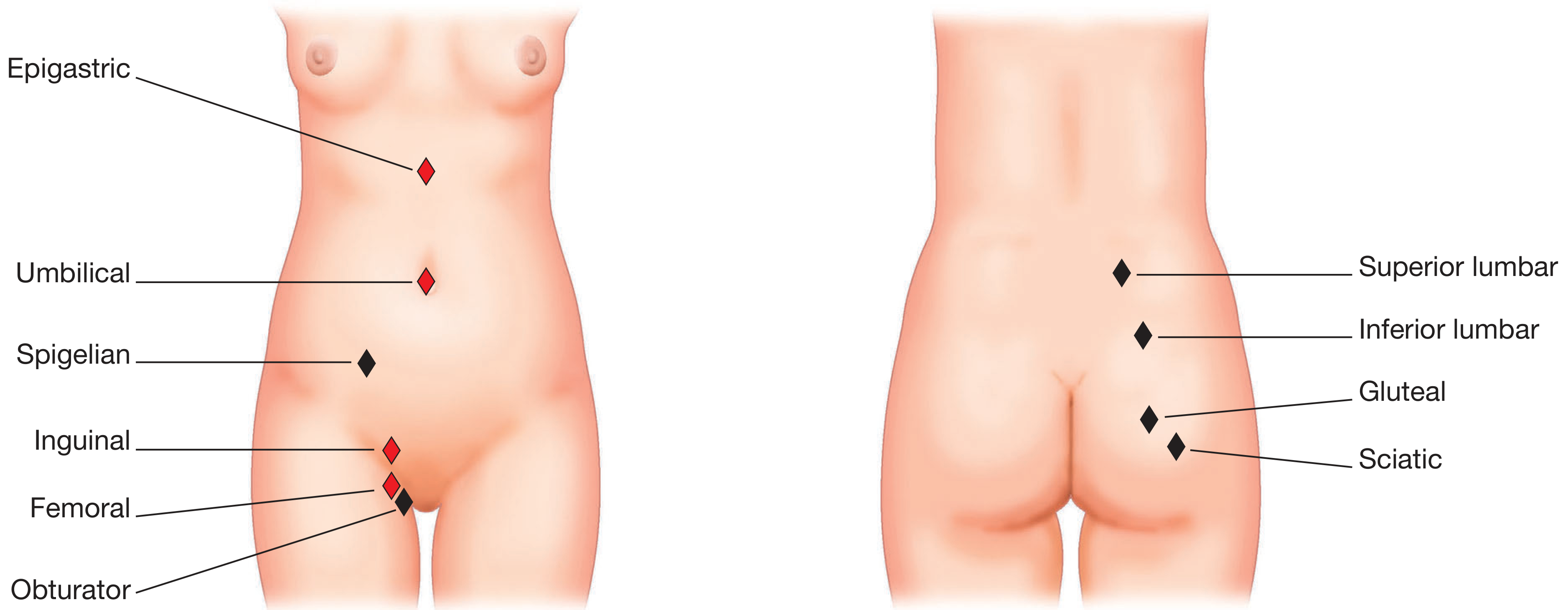
Sites of abdominal wall hernias (red = common, black = rare). Posterior view shows superior lumbar, inferior lumbar, gluteal, and sciatic hernias. — Bailey & Love's Surgery
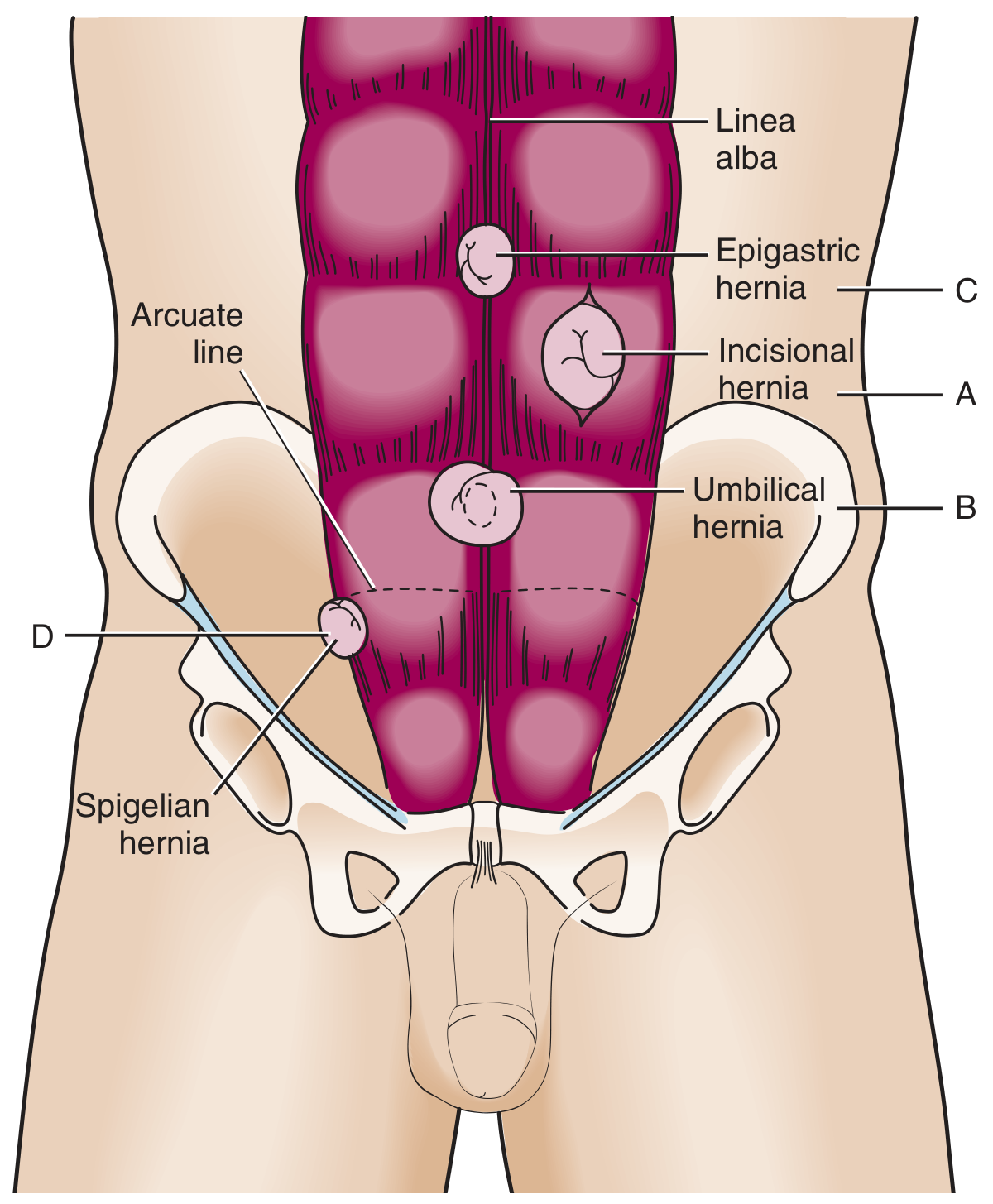
Ventral hernias: incisional (A), umbilical (B), epigastric (C), spigelian (D) — Roberts & Hedges' Clinical Procedures
1. Inguinal Hernia
The most common hernia overall; ~10× more common in males than females.
Anatomy of the Inguinal Canal
The inguinal canal runs 4 cm superomedially from the deep inguinal ring (a defect in transversalis fascia, located midway between the ASIS and pubic tubercle, just lateral to the inferior epigastric vessels) to the superficial inguinal ring (a V-shaped defect in the external oblique aponeurosis above the pubic tubercle).
- Anterior wall: external oblique aponeurosis
- Posterior wall: transversalis fascia (medially reinforced by the conjoint tendon)
- Roof: arching fibres of internal oblique and transversus abdominis (forming the conjoint tendon medially)
- Floor: inguinal ligament (Poupart's) and lacunar ligament (Gimbernat's) medially
The inferior epigastric vessels run just medial to the deep ring — this relationship distinguishes indirect from direct hernias. — Bailey & Love's Short Practice of Surgery, 28th ed.
Indirect Inguinal Hernia (Lateral / Oblique)
- Sac enters the deep inguinal ring lateral to the inferior epigastric vessels, passes through the entire inguinal canal, and may descend into the scrotum
- In children: always indirect, caused by failure of closure of the processus vaginalis (a peritoneal finger-like projection accompanying the descending testis)
- High incidence in premature infants; spontaneous resolution does not occur in children — surgical repair is always indicated
- In adults: may be congenital (persistent PPV) or acquired
All congenital hernias in children are by definition indirect inguinal hernias. — Schwartz's Principles of Surgery, 11th ed.
Direct Inguinal Hernia (Medial)
- Sac protrudes directly forward through the posterior wall of the inguinal canal (Hesselbach's triangle) medial to the inferior epigastric vessels
- Always acquired — results from weakening of the transversalis fascia / conjoint tendon
- Rarely enters the scrotum; typically a wide-necked reducible bulge
- Lower strangulation risk than indirect
Hesselbach's Triangle boundaries:
- Medially: lateral edge of rectus abdominis
- Laterally: inferior epigastric vessels
- Inferiorly: inguinal ligament
Pantaloon Hernia
A simultaneous combination of direct and indirect components, straddling the inferior epigastric vessels like a trouser leg. Difficult to diagnose clinically; often discovered at operation. — Roberts & Hedges' Clinical Procedures in Emergency Medicine
2. Femoral Hernia
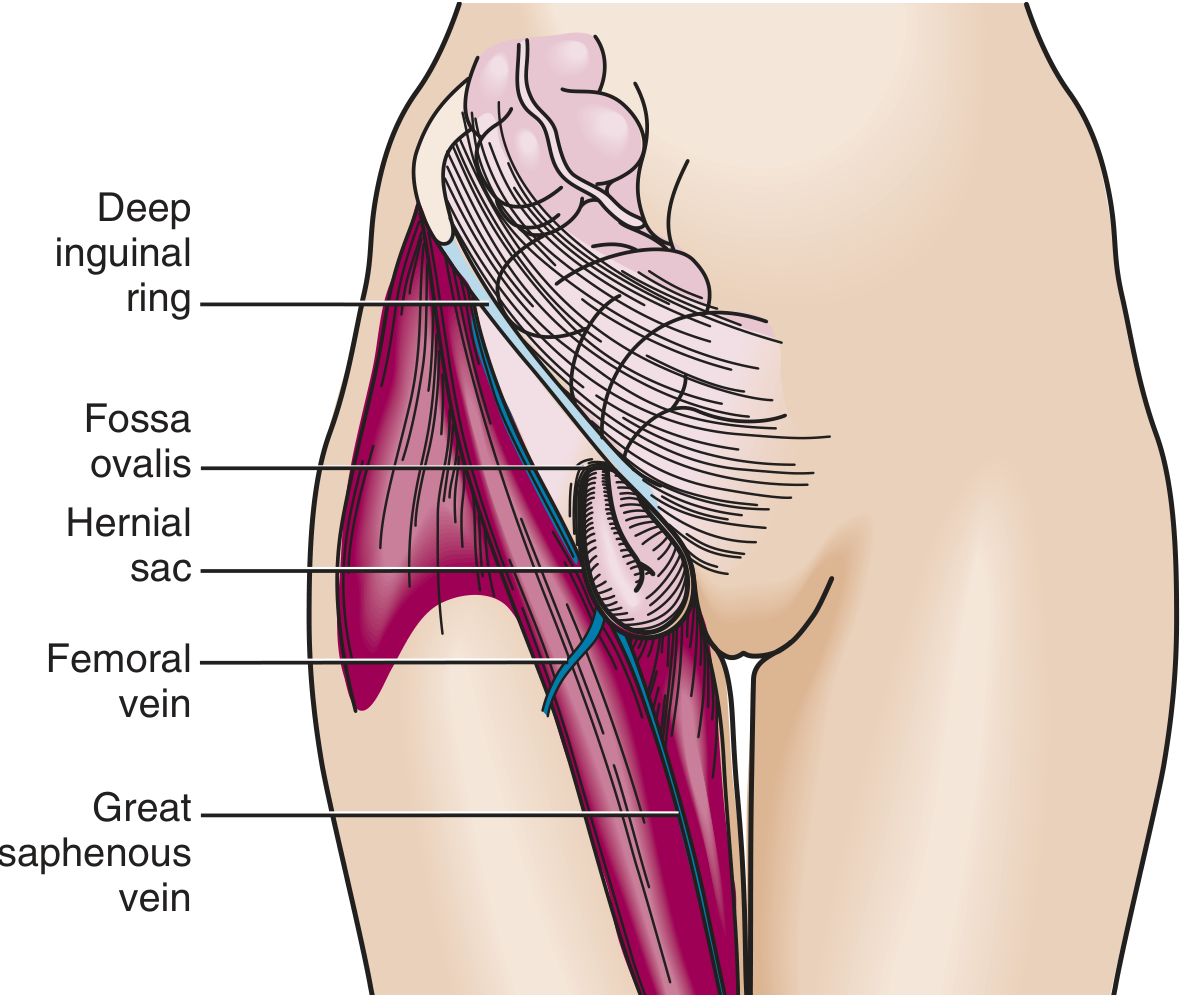
Femoral hernia: sac protrudes through the femoral canal, medial to the femoral vein, and emerges at the fossa ovalis. — Roberts & Hedges' Clinical Procedures
- Protrusion through a defect in the transversalis fascia below the inguinal ligament, medial to the femoral vein and lateral to the lacunar ligament (Gimbernat's), into the femoral canal
- Presents as a mass in the medial thigh / femoral triangle, below and lateral to the pubic tubercle
- More common in women (though inguinal is still the commonest hernia overall in women)
- Very high strangulation risk (up to 45%) due to the narrow, rigid femoral ring — unyielding lacunar ligament medially
- Management: elective repair is urgently recommended due to strangulation risk
3. Umbilical & Para-umbilical Hernia
- Traverses the fibromuscular umbilical ring
- In children: mostly congenital; often resolves spontaneously by age 5 if <2 cm. Surgical repair if persistent past age 5, >2 cm, or incarcerated
- In adults: acquired; associated with obesity, ascites, multiparity, large intra-abdominal masses
- More prone to incarceration and strangulation in adults than children
- Para-umbilical hernias (through linea alba adjacent to umbilicus) are more common in overweight multiparous women
4. Epigastric Hernia
- Occurs through the linea alba, between xiphoid and umbilicus
- Usually small, containing preperitoneal fat; may cause disproportionate pain relative to size
- Found in ~4% of children evaluated for hernias; in adults, typically discovered incidentally or due to pain
5. Incisional Hernia
- Occurs at a prior surgical incision site in up to 20% of patients following abdominal surgery
- Risk factors: wound infection, poor closure technique, obesity, malnutrition, immunosuppression, chronic cough
- Recurrence rate after primary repair: 20–50% (significantly reduced with mesh)
- Larger defects paradoxically have lower incarceration risk (wider neck)
- Contents may include omentum, small bowel, or colon
6. Spigelian Hernia
- Occurs through a defect at the lateral edge of the rectus muscle at the level of the arcuate line (semilunar line)
- Located in the lower abdomen; often interparietal (between muscle layers) so may not be visible externally
- Relatively rare; can be difficult to diagnose — ultrasound or CT often required
7. Hiatal Hernia
A fundamentally different entity — protrusion of intra-abdominal contents (usually the stomach) through the diaphragmatic hiatus into the thorax.
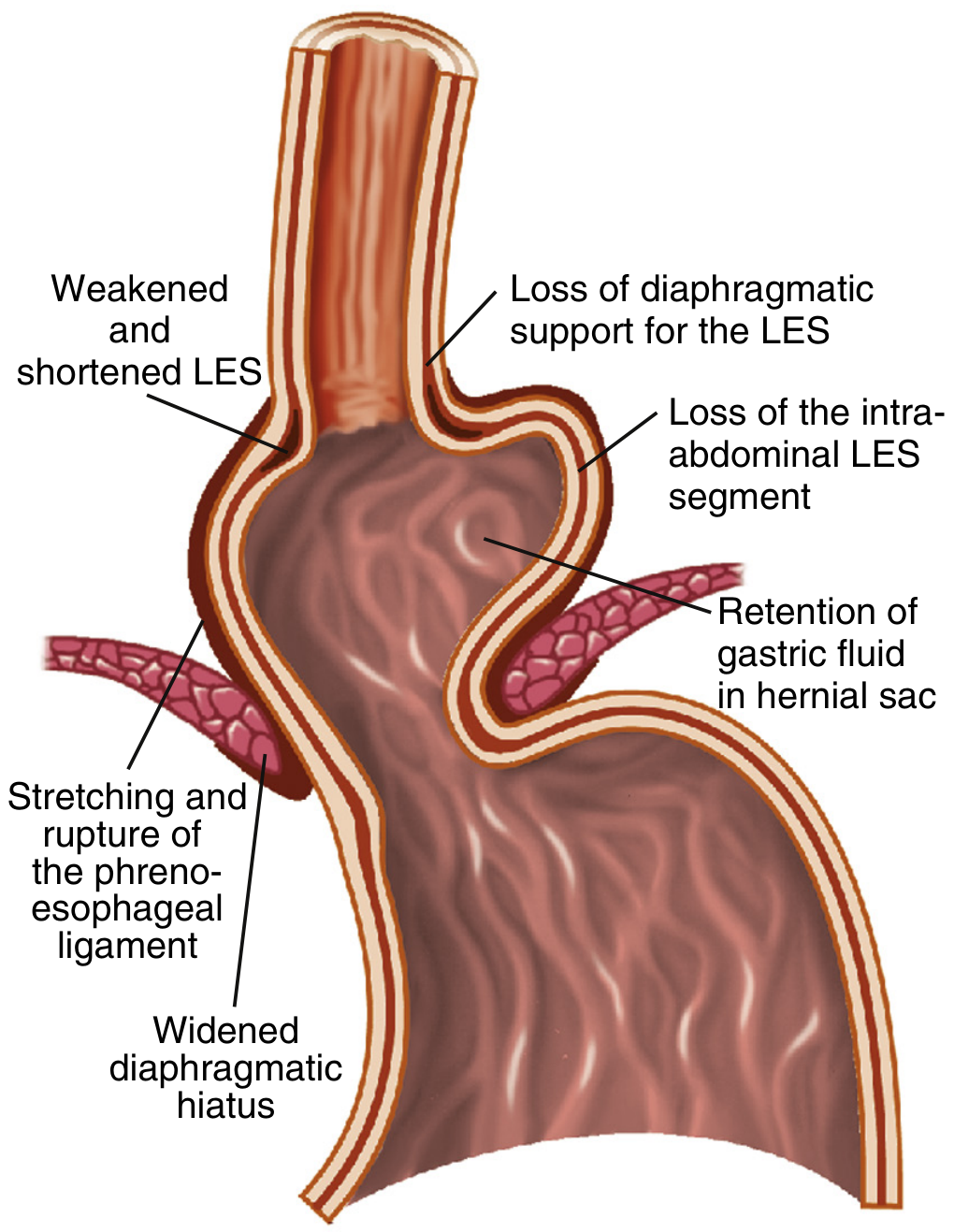
Hiatal hernia antireflux barrier disruption: weakened/shortened LES, lost crural support, retained gastric acid in the hernial sac. — Sleisenger & Fordtran's GI and Liver Disease
Types:
- Type I (Sliding) — GEJ slides upward into the thorax; most common (95%). LES separated from crural diaphragm → promotes GERD
- Type II (Rolling / Para-oesophageal) — gastric fundus rolls up alongside the oesophagus while GEJ remains below diaphragm; rare
- Types III & IV — mixed or with additional organs (colon, spleen, small bowel)
Mechanisms promoting GERD in hiatal hernia:
- Reduced basal LES pressure (loss of intra-abdominal LES segment)
- Increased frequency of transient LES relaxations during gastric distention
- "Acid pocket" retained in the hernial sac — acts as a reservoir for acidic refluxate
- Large (≥3 cm) non-reducible hernias are especially prone to reflux
Hiatal hernia occurs in 54%–94% of patients with reflux oesophagitis — a rate strikingly higher than in the healthy population. — Sleisenger & Fordtran's
8. Internal Hernias
- Herniation through an opening in the peritoneum, mesentery, or omentum rather than through the abdominal wall
- Congenital: most commonly paraduodenal (through the foramen of Winslow)
- Iatrogenic (most common type): following Roux-en-Y gastric bypass, colectomy, pancreaticoduodenectomy — bowel herniates through the mesenteric defect
- Obturator hernia: through the obturator canal; rare but classically presents with medial thigh pain (Howship–Romberg sign); more common in thin elderly women
- Sciatic hernia: through the greater or lesser sciatic foramen; extremely rare
Complications
| Complication | Key Points |
|---|---|
| Incarceration | Contents irreducible; does not by itself imply ischemia |
| Obstruction | Bowel lumen occluded → SBO symptoms (nausea, vomiting, distension, absolute constipation) |
| Strangulation | Vascular compromise → ischemia → necrosis; bowel resection required in >25% of strangulated hernias causing SBO |
| Richter's hernia | Partial wall strangulation; can perforate without complete obstruction |
| Maydl's hernia | Two loops of bowel in the sac with the intervening segment (the "W loop") becoming ischemic intra-abdominally |
Among all patients undergoing surgery for SBO, incarcerated hernia is associated with intestinal ischemia in up to 75% and intestinal necrosis in more than 25%. — Sleisenger & Fordtran's
Clinical Features & Diagnosis
History:
- Dragging, aching groin / abdominal pain; worse on standing, coughing, straining
- Visible or palpable reducible bulge; disappears on lying down
- In strangulation: severe pain, tenderness, skin erythema, systemic toxicity
Examination:
- Cough impulse — the hallmark of a hernia; expansile impulse on coughing
- In inguinal hernia: relation of the bulge to the pubic tubercle
- Indirect: sac lies superomedial to pubic tubercle, may descend into scrotum
- Direct: bulge directly anterior, medial
- Femoral: mass lies inferolateral to pubic tubercle
- Transillumination helps distinguish hydrocele (lights up) from hernia (does not)
- "Getting above" the swelling: if you cannot get above a scrotal swelling, it has originated from the inguinal canal
Imaging:
- Clinical diagnosis is usually sufficient
- Ultrasound: useful for dynamic assessment, especially occult hernias
- CT abdomen/pelvis: required for obese patients, suspected internal hernias, or complex incisional hernias
- MRI groin: for chronic/occult groin pain with equivocal imaging
Management
Conservative / Non-operative
- Watchful waiting appropriate for asymptomatic inguinal hernias in men with minimal symptoms (risk of strangulation ~0.2%/year)
- Trusses/supports: generally not recommended; do not prevent strangulation
- Contraindicated as sole management in femoral hernias (high strangulation risk)
Reduction of Incarcerated Hernia
- Gentle manual pressure directed toward the internal ring; more successful for groin and umbilical hernias
- Light sedation / Trendelenburg positioning may facilitate reduction
- Contraindications: skin erythema, tenderness, suspected strangulation
- After successful reduction: expeditious surgical repair
Surgical Repair — Open Approaches
Pediatric Herniorrhaphy
- High ligation of the sac at the internal ring — repair of the inguinal floor is not required in children
- Recurrence <1%; typically from missed sac, direct component, or femoral hernia
Adult Hernioplasty (Inguinal)
| Technique | Description |
|---|---|
| Shouldice | Multilayer imbrication of transversalis fascia; preferred tension-free tissue repair; <2% recurrence in specialized centres |
| Bassini | Classic posterior wall repair; higher recurrence than mesh-based methods |
| Lichtenstein (tension-free mesh) | Gold standard open repair; flat polypropylene mesh secured over the posterior inguinal wall; <1% recurrence |
| Plug and patch | Mesh cone plugs the internal ring + flat mesh overlay |
Femoral Hernia
- Lockwood (low) approach: below inguinal ligament through femoral canal — simplest
- Lotheissen (high) approach: through inguinal canal
- McEvedy (extraperitoneal): superior incision; best access for emergency/strangulated cases
Surgical Repair — Laparoscopic / Minimally Invasive
| Technique | Description |
|---|---|
| TAPP (Transabdominal Preperitoneal) | Intraperitoneal approach; peritoneal flap raised; mesh placed in preperitoneal space then covered with peritoneum |
| TEP (Totally Extraperitoneal) | Entirely extraperitoneal; avoids peritoneal entry; no risk of intra-abdominal organ injury |
| RARP (Robot-assisted) | Increasingly used for rTAPP; improved dexterity in deep pelvic dissection |
Laparoscopic advantages: less post-operative pain, faster recovery, better for bilateral hernias and recurrent hernias after previous anterior repair.
Special Scenarios
Paediatric Inguinal Hernia
- 10:1 male:female ratio; more common on right
- Incarceration risk is high in infants due to narrow internal ring
- Urgent manual reduction under sedation; herniorrhaphy within 24 hours
- Laparoscopic approach increasingly favoured in children <2 years
Hernia and Small Bowel Obstruction
- Hernia is the second most common cause of SBO after adhesions
- However, operative intervention rate is higher for hernia-related SBO
- CT confirms diagnosis in obese patients or unclear cases
Hernia in Pregnancy
- Umbilical and inguinal hernias may enlarge due to raised intra-abdominal pressure
- Surgical repair generally deferred until post-partum unless emergency
Rare Hernias
| Hernia | Location | Note |
|---|---|---|
| Obturator | Obturator canal | Thin elderly women; Howship–Romberg sign (medial thigh pain on hip extension) |
| Sciatic | Greater/lesser sciatic foramen | Buttock mass; rare; may compress sciatic nerve |
| Lumbar | Superior (Grynfeltt) or inferior (Petit) lumbar triangle | Spontaneous or post-surgical |
| Gluteal | Through gluteal fascia | Extremely rare |
| Parastomal | Adjacent to stoma site | Occurs in 10–50% of stoma patients |
| Perineal | Through pelvic floor | Post-abdominoperineal resection |
| Spigelian | Semilunar line at arcuate line level | Interparietal; clinically occult |
Summary
| Type | Location | Common in | Strangulation Risk | Key Feature |
|---|---|---|---|---|
| Indirect inguinal | Deep ring → inguinal canal | Males; all ages | Moderate (high in infants) | Congenital (PPV); can enter scrotum |
| Direct inguinal | Hesselbach's triangle | Older males | Low | Acquired; medial to epigastric vessels |
| Femoral | Femoral canal | Women > men | Very high (~45%) | Below inguinal ligament; narrow neck |
| Umbilical | Umbilical ring | Infants; obese adults | Moderate (high in adults) | Resolves spontaneously in children |
| Incisional | Prior scar | Any post-surgical patient | Low (size-dependent) | 20% of laparotomies; 20–50% recurrence |
| Epigastric | Linea alba | Adults | Low | Small, often fat-containing |
| Spigelian | Lateral rectus edge | Middle-aged adults | Moderate | Interparietal; occult |
| Hiatal | Diaphragmatic hiatus | Elderly, obese | (volvulus risk in large types) | GERD; Types I–IV |
| Paraduodenal | Mesenteric fossa | Any | High | Most common congenital internal hernia |
Sources: Schwartz's Principles of Surgery 11th ed. · Bailey & Love's Short Practice of Surgery 28th ed. · Sleisenger & Fordtran's GI and Liver Disease · Roberts & Hedges' Clinical Procedures in Emergency Medicine · Gray's Anatomy for Students
causes and risk factors
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have rich, authoritative content. Here is the comprehensive answer:
Hernia — Causes & Risk Factors
The development of a hernia is multifactorial, arising from an interplay of congenital structural defects, biochemical/molecular weakness of connective tissue, and mechanical forces that raise intra-abdominal pressure against a vulnerable wall.
I. Fundamental Mechanism: The Two Requirements
Every hernia requires two conditions to coexist:
- A weakness or defect in the containing wall (congenital opening, fascial degradation, or a surgical scar)
- A force driving contents through that weakness (intra-abdominal pressure)
Either alone is rarely sufficient — it is their combination that precipitates herniation. — Mulholland & Greenfield's Surgery, 7th ed.
II. Congenital Causes
1. Patent Processus Vaginalis (PPV)
The single most important cause of indirect inguinal hernia in all age groups.
- During fetal development, the testis descends from the abdomen to the scrotum, dragging with it a peritoneal finger-like extension called the processus vaginalis
- Normally, the processus vaginalis obliterates a few months before birth
- If it remains patent, a communication persists between the peritoneal cavity and the groin → indirect inguinal hernia
- Partial obliteration → trapped fluid → hydrocele (communicating hydrocele behaves effectively as a hernia)
- Premature infants are at especially high risk because obliteration hasn't yet occurred; incidence of inguinal hernia in premature infants is 9–11% vs. 1–5% in full-term newborns
Closure of the processus vaginalis normally occurs a few months prior to birth. This explains the high incidence of inguinal hernias in premature infants. — Schwartz's Principles of Surgery, 11th ed.
Risk factors for PPV/congenital inguinal hernia:
| Factor | Detail |
|---|---|
| Prematurity | Processus not yet closed |
| Male sex | 6–10× higher incidence than females; testicular descent creates the pathway |
| Right-sided predominance | Right testis descends later; right PPV closes later (~60% right, 30% left, 10% bilateral) |
| Cryptorchidism | ~90% of boys with undescended testis have a patent PPV |
| Female gender | Higher risk of bilaterality when hernia does occur |
| Family history | Increases risk up to 8-fold |
| Connective tissue disorders | See below |
2. Congenital Diaphragmatic Hernia (CDH)
- Caused by failure of closure of the pleuroperitoneal folds during fetal development
- Bochdalek hernia (posterolateral defect) — ~95% of CDH; left-sided predominance
- Morgagni hernia (anterior retrosternal) — ~5% of CDH
- Prevalence ~1–4 per 10,000 live births
- Results in pulmonary hypoplasia and pulmonary hypertension from visceral compression of the developing lungs
3. Umbilical Hernia in Infants
- Due to failure of complete closure of the umbilical ring after cord separation
- Physiologic herniation of the midgut occurs during development (weeks 6–10); failure of return or ring closure → persistent defect
III. Molecular & Biochemical Causes — Connective Tissue Pathology
This is now understood to be the core underlying mechanism of most acquired hernias, particularly direct inguinal and incisional hernias.
Collagen Imbalance: Type I / Type III Ratio
The abdominal wall's structural integrity depends on a balance of collagen types:
- Type I collagen → thick fibres, high tensile strength
- Type III collagen → thinner fibres, temporary scaffolding during tissue remodelling
In patients with hernias, a decreased ratio of Type I to Type III collagen is consistently found in fascial and skin biopsies. This reflects weakened load-bearing capacity of the abdominal wall fascia. — Mulholland & Greenfield's Surgery, 7th ed.
Matrix Metalloproteinase (MMP) Overexpression
MMPs are zinc-dependent enzymes that degrade extracellular matrix (ECM) components, including collagen. Overexpression of MMPs (particularly MMP-1 and MMP-2) in the transversalis fascia leads to accelerated collagen breakdown → weakening of the posterior inguinal wall.
The association between MMP overexpression and abdominal wall hernia was first demonstrated in the transversalis fascia of patients with direct and indirect inguinal hernias.
Smoking — "Metastatic Emphysema"
A landmark observation by Cannon and Read: biopsies of the rectus sheaths from adult smokers with inguinal hernias showed:
- Decreased Type I : Type III collagen ratio
- Significantly elevated circulating serum elastolytic activity (systemic connective tissue degradation beyond the lungs)
This led to the concept of "metastatic emphysema" — that the same enzymatic tissue destruction responsible for pulmonary emphysema acts systemically on abdominal wall fascia, predisposing to hernia formation. — Mulholland & Greenfield's Surgery, 7th ed.
Connective Tissue / Collagen Vascular Diseases
Systemic disorders of connective tissue are strongly associated with hernia:
| Disorder | Hernia Association |
|---|---|
| Ehlers-Danlos syndrome | Diaphragmatic hernia (classical EDS); abdominal wall hernias; vascular rupture risk |
| Marfan syndrome | Inguinal hernia; increased fascial laxity |
| Osteogenesis imperfecta | Inguinal hernia due to type I collagen mutations |
| Congenital hip dislocation | Associated with inguinal hernia |
Various connective tissue disorders, such as osteogenesis imperfecta, Marfan syndrome, and Ehlers-Danlos syndrome, are associated with hernias. — Mulholland & Greenfield's Surgery
IV. Factors That Raise Intra-Abdominal Pressure (Mechanical Causes)
These forces act on an already vulnerable wall to precipitate herniation or worsen an existing hernia.
1. Obesity
- Central obesity raises resting and dynamic intra-abdominal pressure chronically
- Strongly linked to umbilical, para-umbilical, incisional, and hiatal hernias
- Raised intra-abdominal pressure is the likely mechanism for hiatal hernia and the marked increase in prevalence of reflux oesophagitis / Barrett's oesophagus in obese patients
- Also impairs wound healing → greater incisional hernia risk post-surgery
2. Chronic Cough / COPD / Smoking
- Repeated Valsalva-like surges in intra-abdominal pressure
- COPD is listed as a major independent risk factor for abdominal wall hernia development
- Smoking acts via two pathways: (a) MMP-mediated collagen destruction; (b) chronic cough-induced pressure surges
3. Straining at Stool / Constipation
- Chronic straining generates repeated episodes of raised intra-abdominal pressure
- Important contributing factor to inguinal and femoral hernia, especially in older patients
4. Prostatism / Bladder Outflow Obstruction
- Straining to void → chronic intra-abdominal pressure elevation
- Recognised risk factor for inguinal hernia
5. Ascites
- Sustained, markedly elevated intra-abdominal pressure
- Predisposes to umbilical hernia (often large and tense in cirrhotic patients with ascites)
- High complication risk (skin ulceration, spontaneous rupture)
6. Pregnancy
- Raised intra-abdominal pressure + hormonal-mediated connective tissue laxity
- Predisposes to umbilical, inguinal, and hiatal hernias
- May cause worsening GERD via hiatal hernia mechanism
7. Heavy Lifting / Occupational Factors
The role is nuanced and medico-legally contested:
- A systematic review found no definitive causal relationship between single strenuous mechanical events and hernia formation
- However, a large Danish register-based cohort study showed that cumulative daily lifting and prolonged standing/walking at work was associated with increased risk of indirect inguinal hernia repair
- Hypothesis: patent processus vaginalis is more susceptible to cumulative pressure changes; direct hernias may involve connective tissue degradation through separate mechanisms
There is minimal evidence that vigorous abdominal wall activity is an independent risk factor for hernia development despite the overwhelming opinion to the contrary in the lay literature. — Mulholland & Greenfield's Surgery, 7th ed.
8. Peritoneal Dialysis
- The dialysate fills the peritoneal cavity, producing sustained raised intra-abdominal pressure
- Significantly associated with inguinal and umbilical hernia development
9. Thoracic or Abdominal Aortic Aneurysm
- Strongly associated with inguinal hernia — both conditions share the same underlying defect in ECM/collagen metabolism
- Patients undergoing AAA repair have high rates of concurrent or subsequent hernia
V. Surgical / Iatrogenic Causes — Incisional Hernia
The most preventable hernia type. Up to 20% of laparotomy patients develop incisional hernia.
Risk factors for incisional hernia development:
| Category | Specific Risk Factors |
|---|---|
| Wound-related | Surgical site infection (most important), wound dehiscence, haematoma |
| Surgical technique | Inadequate fascial bites, excessive tension at closure, inappropriate suture material |
| Patient factors | Obesity, malnutrition, hypoalbuminaemia, diabetes mellitus, immunosuppression, jaundice, anaemia |
| Drugs | Corticosteroids, chemotherapy agents, bevacizumab |
| Systemic disease | Chronic renal failure, liver failure/cirrhosis |
| Lifestyle | Smoking, early return to physical activity |
| Prior hernia | Previous incisional hernia repair (recurrence 20–50%) |
Poor wound healing, e.g., because of infection, increases the likelihood of developing an incisional hernia. — Roberts & Hedges' Clinical Procedures in Emergency Medicine
Specific benefit of preventive mesh has been demonstrated in: older adults (>65 years), patients with prior wound infection, obesity, malnutrition, smoking, immunosuppression, and chronic inflammatory disease.
VI. Evolutionary/Anatomical Predisposition
An often-overlooked contributor is the evolutionary transition from quadruped to biped:
- In four-legged animals, the inguinal region bears minimal gravitational load
- In bipeds, the unprotected groin directly faces changes in intra-abdominal pressure with every movement
- The inguinal canal (necessary for testicular descent) represents an inherent structural compromise in the abdominal wall of all males — it is, in essence, a controlled weakness
In the evolution from a quadruped to a biped, the unprotected groin is more vulnerable to changes in intra-abdominal pressure, predisposing to inguinal herniation. — Mulholland & Greenfield's Surgery, 7th ed.
The natural openings of the abdominal wall (inguinal ring, umbilicus, oesophageal hiatus) are the sites of least resistance and account for the vast majority of hernias.
VII. Cause-Specific Summary by Hernia Type
| Hernia Type | Primary Cause | Key Risk Factors |
|---|---|---|
| Indirect inguinal | Patent processus vaginalis | Prematurity, male sex, family history, cryptorchidism |
| Direct inguinal | Fascial / transversalis weakness | Aging, smoking, COPD, obesity, collagen disorders, AAA |
| Femoral | Narrow femoral ring enlargement | Female sex, aging, prior inguinal hernia surgery |
| Umbilical (child) | Failure of ring closure | Prematurity, low birth weight, umbilical infection |
| Umbilical (adult) | Chronic pressure + fascial laxity | Obesity, ascites, multiparity, heavy lifting |
| Incisional | Surgical wound failure | Wound infection, obesity, malnutrition, steroids, smoking |
| Epigastric | Linea alba fibrous defect | Age, male sex, obesity |
| Spigelian | Semilunar line fascial gap | Middle age, COPD, smoking, connective tissue disease |
| Hiatal | Weakening of oesophageal hiatus | Obesity, aging, chronic straining, familial smooth muscle disorder, reflux-induced oesophageal shortening |
| Congenital diaphragmatic | Failure of pleuroperitoneal fold closure | Developmental defect; associated genetic syndromes |
| Internal (iatrogenic) | Mesenteric defect left open | Roux-en-Y bypass, colectomy, Whipple's procedure |
| Parastomal | Fascial weakness around stoma | Obesity, poor stoma siting, high-output stoma |
Sources: Mulholland & Greenfield's Surgery: Scientific Principles and Practice, 7th ed. · Schwartz's Principles of Surgery, 11th ed. · Yamada's Textbook of Gastroenterology, 7th ed. · Roberts & Hedges' Clinical Procedures in Emergency Medicine · Sabiston Textbook of Surgery · Sleisenger & Fordtran's GI and Liver Disease · Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.