I now have all the textbook content needed. Let me build the complete inline presentation now - all slides rendered directly in chat with flowcharts and images.
🔴 AGE-RELATED MACULAR DEGENERATION (AMD)
A Complete Ophthalmology Presentation — Basic to Advanced
Sources: Kanski's Clinical Ophthalmology 10th Ed · Ryan's Retina 3rd Ed · Wills Eye Manual · AREDS/AREDS2 · PubMed 2025–2026
📌 SLIDE 1 — TITLE & OVERVIEW
┌─────────────────────────────────────────────────────────────────┐
│ │
│ AGE-RELATED MACULAR DEGENERATION │
│ AMD │
│ │
│ "The Silent Thief of Central Vision" │
│ │
│ ● Epidemiology & Burden │
│ ● Anatomy of the Macula │
│ ● Classification & Staging │
│ ● Pathogenesis — Dry & Wet │
│ ● Risk Factors & Genetics │
│ ● Clinical Features & Investigations │
│ ● OCT & OCT-A — Advanced Imaging │
│ ● Management — Dry & Wet AMD │
│ ● Emerging Therapies & Gene Therapy │
│ ● Monitoring & Prognosis │
│ │
└─────────────────────────────────────────────────────────────────┘
📌 SLIDE 2 — EPIDEMIOLOGY & GLOBAL BURDEN
| Parameter | Figure |
|---|
| Global prevalence (2020) | 196 million |
| Projected global (2040) | 288 million |
| Prevalence in adults >50 years | 8.7% |
| % of global blindness | 8.5% |
| US prevalence | >1.75 million |
| Cumulative incidence at ≥75 years | 8% |
| Risk of 2nd eye CNV (after unilateral wet AMD) | 10–12% per year |
| Age of onset | 6th–9th decade |
Key Facts
- Leading cause of irreversible central vision loss in adults >55 in developed countries
- Prevalence doubles with each decade after age 55
- Predominantly affects industrialized nations
- 90% = dry AMD | 10% = wet AMD (but accounts for 90% of AMD-related blindness)
- Peripheral vision is preserved throughout — only central vision is affected
- "Individuals can walk down a street without difficulty but cannot recognize facial features" — Harrison's 22E
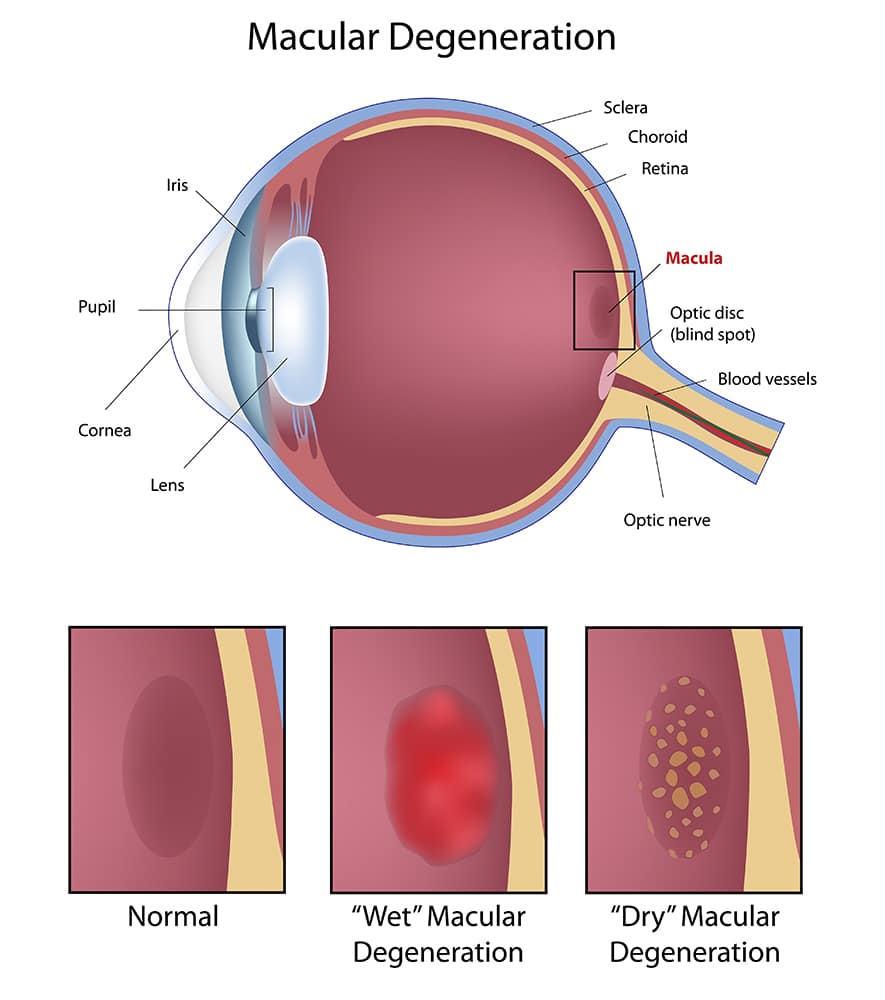
📌 SLIDE 3 — ANATOMY OF THE MACULA
CROSS-SECTION OF THE MACULA (Kanski's Fig. 14.1 / Ryan's Ch. 65)
VITREOUS
↓
┌─────────────────────────────────────────────────────────┐
│ INNER LIMITING MEMBRANE (ILM) │
├─────────────────────────────────────────────────────────┤
│ NERVE FIBER LAYER (NFL) │
├─────────────────────────────────────────────────────────┤
│ GANGLION CELL LAYER (GCL) │
├─────────────────────────────────────────────────────────┤
│ INNER PLEXIFORM LAYER (IPL) │
├─────────────────────────────────────────────────────────┤
│ INNER NUCLEAR LAYER (INL) │
├─────────────────────────────────────────────────────────┤
│ OUTER PLEXIFORM LAYER (OPL) / Henle Fiber Layer (HFL) │
├─────────────────────────────────────────────────────────┤
│ OUTER NUCLEAR LAYER (ONL) — Photoreceptor nuclei │
├─────────────────────────────────────────────────────────┤
│ EXTERNAL LIMITING MEMBRANE (ELM) │
├─────────────────────────────────────────────────────────┤
│ PHOTORECEPTORS — Rods (periphery) & Cones (fovea) │
│ Ellipsoid Zone (EZ) — inner segments │
│ Interdigitation Zone (IZ) — outer segments/RPE │
├─────────────────────────────────────────────────────────┤
│ RETINAL PIGMENT EPITHELIUM (RPE) ←── KEY TARGET │
│ RPE basement membrane (RPE-BL) │
├─────────────────────────────────────────────────────────┤
│ BRUCH'S MEMBRANE (5 layers): │
│ • RPE basement membrane (inner) │
│ • Inner collagenous zone (ICZ) │
│ • Elastic layer │
│ • Outer collagenous zone (OCZ) │
│ • Choriocapillaris basement membrane (outer) │
├─────────────────────────────────────────────────────────┤
│ CHORIOCAPILLARIS ← Sole blood supply to outer retina │
├─────────────────────────────────────────────────────────┤
│ CHOROID (Haller's & Sattler's layers) │
└─────────────────────────────────────────────────────────┘
↓
SCLERA
The Critical Triad in AMD
RPE + Bruch's Membrane + Choriocapillaris = Outer Retinal Neurovascular Unit
Disruption of any one component → photoreceptor damage → central vision loss
| Structure | Normal Function | Role in AMD |
|---|
| RPE | Phagocytoses shed photoreceptor outer segments; retinoid recycling; blood-retinal barrier | Primary site of lipofuscin accumulation; atrophies in dry AMD |
| Bruch's Membrane | 5-layer barrier between RPE and choriocapillaris; supports RPE attachment | Site of drusen deposition; calcification; CNV penetrates through here |
| Choriocapillaris | Sole vascular supply to outer retina and RPE | Obliterated in GA; "dark halo" around MNV on OCT-A |
| Fovea/Foveola | Highest cone density (199,000/mm²); sharpest central acuity | Primary AMD damage site |
| Macula lutea | ~5.5 mm central retinal area temporal to disc | Lutein/zeaxanthin pigment provides photoprotection |
📌 SLIDE 4 — CLASSIFICATION & STAGING (AREDS System)
┌─────────────────────────────────────────────────────────────────────┐
│ AMD CLASSIFICATION │
│ (AREDS Simplified Scale & Clinical Grading) │
└─────────────────────────────────────────────────────────────────────┘
┌──────────────┬──────────────────────────────┬─────────┬───────────┐
│ STAGE │ FEATURES │ DRUSEN │ RISK/5yr │
├──────────────┼──────────────────────────────┼─────────┼───────────┤
│ NO AMD │ Normal macula │ None or │ <0.5% │
│ │ │ small │ │
├──────────────┼──────────────────────────────┼─────────┼───────────┤
│ EARLY AMD │ Small/medium drusen │ <125 μm │ 0.5–1% │
│ │ No pigment change │ │ │
├──────────────┼──────────────────────────────┼─────────┼───────────┤
│ INTERMEDIATE │ Large drusen ≥125 μm │ ≥125 μm │ ~13–18% │
│ AMD │ OR pigment changes │ soft │ (bilateral│
│ │ May have subtle visual loss │ drusen │ +pigment: │
│ │ │ │ ~50%) │
├──────────────┼──────────────────────────────┼─────────┼───────────┤
│ LATE AMD │ Geographic atrophy │ Present │ ~50% │
│ — DRY (GA) │ Well-demarcated RPE loss │ │ │
│ │ Visible choroidal vessels │ │ │
├──────────────┼──────────────────────────────┼─────────┼───────────┤
│ LATE AMD │ Choroidal neovascularization │ Usually │ URGENT │
│ — WET (nAMD) │ SRF, hemorrhage, exudate │ present │ anti-VEGF │
│ │ Acute central visual loss │ │ │
└──────────────┴──────────────────────────────┴─────────┴───────────┘
AREDS Simplified Risk Score (Kanski Ch. 14 / Ryan's Ch. 66)
Score 1 point per eye for each present:
- Large drusen (≥125 μm)
- Pigmentary abnormality (hyper or hypo)
→ Maximum score = 4 (bilateral large drusen + bilateral pigment changes)
| Person Score | 5-yr Risk of Advanced AMD |
|---|
| 0 | ~0.5% |
| 1 | ~3% |
| 2 | ~12% |
| 3 | ~25% |
| 4 | ~50% |
📌 SLIDE 5 — DRY AMD PATHOGENESIS FLOWCHART
╔══════════════════════════════════════════════════════════════╗
║ DRY AMD PATHOGENESIS — MOLECULAR CASCADE ║
╚══════════════════════════════════════════════════════════════╝
AGING + GENETIC SUSCEPTIBILITY (CFH Y402H, ARMS2/HTRA1)
+ OXIDATIVE STRESS (SMOKING, LIGHT EXPOSURE)
│
▼
┌─────────────────────────────┐
│ IMPAIRED RPE FUNCTION │
│ ↑ Lipofuscin in RPE cells │
│ (A2E = phototoxic toxin) │
└─────────────┬───────────────┘
│
▼
┌─────────────────────────────────────────┐
│ BRUCH'S MEMBRANE CHANGES │
│ • Lipoprotein secretion by RPE → │
│ accumulates in sub-RPE space │
│ • Thickening, calcification │
│ • Lipid peroxidation (DHA, linolenic) │
└─────────────┬───────────────────────────┘
│
▼
┌─────────────────────────────────────────┐
│ DRUSEN FORMATION │
│ Hard → Soft → Confluent │
│ Contents: ApoB lipoproteins, │
│ vitronectin, complement proteins, │
│ esterified & unesterified cholesterol │
└─────────────┬───────────────────────────┘
│
▼
┌─────────────────────────────────────────┐
│ COMPLEMENT ACTIVATION │
│ CFH variants → ↓ regulation of C3 │
│ C3 → C3a + C3b → C5 → C5a + C5b-9 │
│ MAC (membrane attack complex) formed │
└─────────────┬───────────────────────────┘
│
▼
┌─────────────────────────────────────────┐
│ CHRONIC SUBCLINICAL INFLAMMATION │
│ RPE cell stress → senescence │
│ Pyroptotic cell death (NLRP3) │
└─────────────┬───────────────────────────┘
│
▼
┌─────────────────────────────────────────┐
│ GEOGRAPHIC ATROPHY (GA) │
│ RPE + choriocapillaris + photoreceptors│
│ → Well-defined area of atrophy │
│ → Central scotoma, legal blindness │
└─────────────────────────────────────────┘
📌 SLIDE 6 — WET AMD PATHOGENESIS FLOWCHART
╔══════════════════════════════════════════════════════════════╗
║ WET AMD PATHOGENESIS — ANGIOGENIC CASCADE ║
╚══════════════════════════════════════════════════════════════╝
HYPOXIA / OXIDATIVE STRESS in RPE (from drusen/GA)
│
▼
┌──────────────────────┐
│ ↑ VEGF-A expression │
│ + Angiopoietin-2 │
│ (destabilizes BV) │
└──────────┬───────────┘
│
▼
┌──────────────────────────────────────┐
│ Binds VEGFR-1 / VEGFR-2 on │
│ choriocapillaris endothelial cells │
└──────────┬───────────────────────────┘
│
┌────────────┴────────────┐
▼ ▼
ANGIOGENESIS PERMEABILITY ↑
(New vessel sprouting) (Fluid leakage into
CNV growth subretinal/intraretinal
through Bruch's space: SRF, IRF, PED)
membrane
│ │
└────────────┬────────────┘
▼
┌─────────────────────────────────────┐
│ MACULAR NEOVASCULARIZATION (MNV) │
│ Type 1 / Type 2 / Type 3 │
└──────────────┬──────────────────────┘
│
▼
┌─────────────────────────────────────┐
│ COMPLICATIONS │
│ • Subretinal hemorrhage │
│ • RPE tears │
│ • Macular atrophy (MA) │
│ • Disciform scar (end-stage) │
│ → IRREVERSIBLE CENTRAL VISION LOSS │
└─────────────────────────────────────┘
FARICIMAB DUAL MECHANISM (NEW 2022):
Anti-VEGF-A + Anti-Ang-2
↓ ↓
Block CNV Stabilize vessels
└────────┬────────┘
▼
Superior vascular stability
→ Extended dosing Q12–16 weeks
📌 SLIDE 7 — DRUSEN IN DETAIL (Ryan's Ch. 65-66 + Kanski Ch. 14)
Types of Drusen
| Type | Size | Appearance | OCT | Risk |
|---|
| Hard (drupelets) | ≤63 μm | Well-defined, white-yellow, discrete | Small RPE elevations | Low (unless + pigment changes) |
| Intermediate | 63–125 μm | Fairly well-defined, yellow-white | Moderate elevation | 10% to late AMD/5yr if bilateral + pigment |
| Soft | >125 μm | Poorly defined, confluent, amorphous | Convex; homogeneous med. reflectivity | 13–50% risk of late AMD/5yr |
| Drusenoid PED | >200 μm | Shallow elevated pale areas; scalloped edges | Homogeneous hyperreflective PED; no SRF | 75% → GA; 25% → MNV by 10yr |
| Calcified drusen | Variable | Glistening white nodules | Highly reflective with posterior shadowing | Late feature; may signal collapse → GA |
| Reticular pseudodrusen (SDD) ⭐ | ~250 μm | Yellow-white interlacing network | Subretinal (above RPE); hyporeflective on FAF | High risk for Type 3 MNV and GA |
⭐ NEW: Subretinal Drusenoid Deposits (SDD) — Key Gap Finding
SOFT DRUSEN vs. SUBRETINAL DRUSENOID DEPOSITS (Ryan's Ch. 65, Table 65.2)
Feature Soft Drusen/BLinD Subretinal Drusenoid Deposits
─────────────────────────────────────────────────────────────────────────────
Location Sub-RPE (external to BM) SUBRETINAL (above RPE apical)
Lipids Esterified + unesterified Unesterified cholesterol ONLY
cholesterol (no oil red-O binding)
FAF appearance Hyperautofluorescent HYPOautofluorescent
Complement C5b-9 localized C1q localized to SDD, not drusen
Associated MNV type Type 1 (sub-RPE) Type 3 (intraretinal origin) ← KEY
Follow rod topography Follows CONES (subfoveal) Follows RODS (perifoveal ring)
Impact of laser Improved (↓ progression) WORSENED (↑ progression) ← KEY
Mendelian disorders Sorsby, Doyne, etc. AMD-specific
─────────────────────────────────────────────────────────────────────────────
Clinical significance: SDD/reticular pseudodrusen predict faster GA progression and Type 3 MNV. They are best seen on infrared reflectance and swept-source OCT — often missed on color fundus photography alone.
📌 SLIDE 8 — RISK FACTORS
Non-Modifiable
| Factor | Detail |
|---|
| Advanced age | Strongest risk factor; prevalence doubles each decade after 55 |
| Family history | 3–4× risk if first-degree relative affected |
| Race | White/European >> Asian >> African American |
| Female sex | Slight increase in prevalence |
| Hyperopia | Each +1 diopter → increased odds (pooled OR 1.13 per diopter) |
| Light iris color | Modest increase (blue/grey iris) |
Modifiable
| Factor | Effect |
|---|
| Cigarette smoking ⭐ | 2–4× risk; strongest modifiable risk factor; accounts for ~20% of AMD cases in women |
| Systemic hypertension | Significant association, especially systolic BP |
| High dietary fat / low omega-3 | Higher vegetable fat → ↑ risk; oily fish protective |
| Obesity / high BMI | Increases risk, accelerates progression (CFH + ARMS2 genetic risk enhanced) |
| Low lutein/zeaxanthin | Protective pigment; low serum levels = ↑ risk |
| Chronic UV/visible light | Modest association; blue light exposure debated |
| Sedentary lifestyle | Modest increase |
Ocular Risk Factors
| Factor | Risk |
|---|
| Soft large drusen ≥125 μm | Major predictor of progression |
| RPE pigment clumping | Risk for CNV development |
| Wet AMD in fellow eye | 10–12% per year CNV risk in other eye |
| SDD/reticular pseudodrusen | ↑ risk of Type 3 MNV and faster GA |
📌 SLIDE 9 — GENETICS OF AMD (Ryan's Ch. 64 + Thompson & Thompson)
GENETIC ARCHITECTURE OF AMD
AMD is POLYGENIC and MULTIFACTORIAL
GWAS identified >40 susceptibility loci
| Gene | Locus | Function | Variant | Risk |
|---|
| CFH (Y402H) | 1q32 | Regulates alternative complement pathway (C3b inactivation) | rs1061170 | 2–4× risk (present in 35% of AMD cases) |
| ARMS2/HTRA1 | 10q26 | ARMS2 function unclear; HTRA1 = serine protease | rs10490924 | Major risk allele |
| C3 | 19p13 | Central effector of all complement pathways | R102G variant | Increased risk |
| CFI | 4q25 | Inactivates C3b; dampens complement | Rare variants | Loss of function → ↑ risk |
| CFB/C2 | 6p21 | Classical/alternative pathway | Protective haplotype | Protective |
| C9 | 5p13 | Terminal complement complex | Variants identified | Risk |
| VEGF pathway | Various | Neovascular susceptibility | Multiple loci | CNV risk |
| APOE | 19q13 | Lipid transport (ε2/ε4 isoforms) | ε4 protective | Controversial |
Genetic Model
Genetic susceptibility Environmental exposure
(CFH + ARMS2 variants) × (Smoking + Diet + Age)
↓
Clinical AMD phenotype
(Type/severity/age of onset)
KEY: Smoking + high BMI + CFH risk genotype = COMPOUNDED risk
→ Earlier onset of advanced AMD (especially Type 3 MNV)
📌 SLIDE 10 — CLINICAL FEATURES
DRY AMD — Symptoms
- Gradual, insidious loss of central vision (months to years)
- Metamorphopsia (Amsler grid distortion)
- Difficulty reading, face recognition, watching TV
- Often asymptomatic in early/intermediate stages
- Vision often better in bright light (pupil constriction improves optics)
- Peripheral vision always preserved
- Delayed dark adaptation (rod function impaired early) — functional biomarker
DRY AMD — Signs (Chronological Order per Kanski)
1. Numerous intermediate-large soft drusen
↓
2. Focal hyper- and/or hypopigmentation of RPE
↓
3. Drusenoid PED (confluent large soft drusen)
↓
4. Drusen calcification (glistening white nodules)
↓
5. Drusen regression/fading (↓ autofluorescence)
↓
6. GEOGRAPHIC ATROPHY (GA):
• Well-defined, sharply demarcated RPE depigmentation
• Visible choroidal vessels beneath (bare choroid)
• Central or perifoveal distribution
• Horseshoe-shaped → bull's-eye → foveal involvement
• Average growth rate: 1.78 mm²/year (square root transformed)
WET AMD — Symptoms (URGENT PRESENTATION)
- Sudden onset central or paracentral scotoma
- Acute metamorphopsia — lines appear wavy/distorted
- Photopsias (flashes) in central visual field
- Rapid, profound central visual loss (hours to days)
WET AMD — Signs (Kanski + Ryan's Ch. 67)
CRITICAL SIGNS:
● Drusen + subretinal fluid (SRF) ← most common
● Intraretinal fluid (IRF) / cystoid macular edema
● Pigment epithelial detachment (PED):
- Serous PED (smooth dome; optically empty on OCT)
- Fibrovascular PED (irregular, hyperreflective)
- Drusenoid PED (homogeneous; no SRF)
- Haemorrhagic PED (dark red; underlying MNV or PCV)
● Subretinal/intraretinal haemorrhage
● Lipid exudates (hard exudates)
● Subretinal fibrosis (disciform scar — end stage)
● RPE tears (rip at edge of PED)
📌 SLIDE 11 — MNV TYPES & CLASSIFICATION (Ryan's Ch. 67 + Kanski)
╔═══════════════════════════════════════════════════════════════════╗
║ MACULAR NEOVASCULARIZATION — ANATOMIC CLASSIFICATION ║
╚═══════════════════════════════════════════════════════════════════╝
| Feature | Type 1 (Occult CNV) | Type 2 (Classic CNV) | Type 3 (RAP/Intraretinal) |
|---|
| Location | Sub-RPE (beneath RPE) | Subretinal (above RPE) | Intraretinal origin |
| Origin | Choroidal vessels | Choroidal vessels | Deep retinal capillary plexus |
| FFA | Fibrovascular PED; late irregular leakage ("occult") | Well-defined early hyperfluorescence ("classic"); late leakage | Hot spot; focal intraretinal hyperfluorescence |
| ICGA | Plaque or hot spot | Not usually needed | Hot spot + hairpin loop (draining venule + feeding arteriole) |
| OCT B-scan | Shallow irregular PED ± SRF; "SIRE" (Shallow Irregular RPE Elevation) | Subretinal hyperreflective material (SHRM) above RPE; cystoid ME | Intraretinal hyperreflective lesion crossing outer retinal layers; IRF |
| OCT-A | Glomerulus/medusa-shaped complex in outer retina slab | Fine indistinct vessel network above RPE | Tuft-like capillary network; nascent lesion as hyperreflective foci with flow |
| Frequency | Most common (50–60%) | 15–20% | ~20%; bilateral in ~75% |
| Associated with | Drusenoid PED; type 1 non-exudative MNV | Subretinal hemorrhage | SDD/reticular pseudodrusen; bilateral |
| Prognosis | Best if treated early | Favorable if treated | Good response to anti-VEGF |
| Associated atrophy | Less | Less | Highest GA risk (49% at 2yr in meta-analysis) |
⭐ NEW: Non-Exudative (Quiescent) Type 1 MNV — Key Gap Finding
Ryan's Ch. 67: Grossniklaus & Green (1998) proposed that Type 1 MNV may be biologically protective — the neovascular complex may recapitulate morphology of native choriocapillaris, supporting hypoxic/micronutrient-insufficient outer retinal cells. Histological evidence: outer retinal cells overlying non-exudative MNV remain intact; neovessels have fenestrations from hypoxic RPE-secreted VEGF. Non-exudative MNV should not automatically trigger treatment — decision based on presence of exudation.
📌 SLIDE 12 — POLYPOIDAL CHOROIDAL VASCULOPATHY (PCV)
Key Features (Kanski Ch. 14 + Ryan's Ch. 67)
- Aberrant inner choroidal vessel network terminating in polypoidal dilations
- Predominantly in Asian and African populations (PCV accounts for 25–50% of "wet AMD" in Asians vs. 8–13% in Whites)
- Patient: often >50 years, female, no classical drusen
- May represent Type 1 MNV subtype (aneurysmal MNV1) or pachychoroid neovasculopathy spectrum
Diagnostic Criteria
| Modality | Finding |
|---|
| ICGA ⭐ | GOLD STANDARD — polypoidal hyperfluorescent lesions at 5–12 min; branching vascular network (BVN) in early phase |
| OCT | "Double-layer sign" (elevated RPE with SRF); notched PED; serosanguineous PED |
| FFA | Occult or classic leakage; may miss polyps |
| OCT-A | Can detect BVN but polyps may not always show flow (slow flow) |
Treatment
- PDT + anti-VEGF combination is superior to anti-VEGF monotherapy for polyp closure
- EVEREST II trial: Combination PDT + ranibizumab achieved 69.3% complete polyp regression vs. 34.7% monotherapy
- Anti-VEGF monotherapy (faricimab/aflibercept) can control exudation but incomplete polyp regression
📌 SLIDE 13 — INVESTIGATIONS & IMAGING
╔══════════════════════════════════════════════════════════════════╗
║ INVESTIGATION PATHWAY FOR SUSPECTED AMD ║
╚══════════════════════════════════════════════════════════════════╝
PATIENT WITH SUSPECTED AMD
│
▼
1. BEST CORRECTED VISUAL ACUITY (BCVA) — ETDRS/Snellen
│
▼
2. AMSLER GRID — 10° central field (both eyes separately)
→ Metamorphopsia = URGENT wet AMD flag
│
▼
3. SLIT-LAMP BIOMICROSCOPY + DILATED FUNDUS EXAMINATION
(90D / 78D lens — grade drusen, RPE changes)
│
▼
4. OCT (Optical Coherence Tomography) — MANDATORY
[SRF, IRF, drusen volume, PED, ellipsoid zone status]
│
┌────┴─────┐
▼ ▼
DRY AMD WET AMD SUSPECTED
│ │
▼ ▼
FAF (Fundus FFA (Fluorescein Angiography)
Autofluorescence) → Classic vs occult CNV
→ GA extent, → Leakage pattern
RPE viability
│ │
▼ ▼
Document, OCT-A (non-invasive MNV mapping)
monitor ± ICGA (if PCV suspected)
Imaging Modalities — Reference Table (Kanski Ch. 14 / Ryan's Ch. 67)
| Modality | Mechanism | Key Information | When Used |
|---|
| Fundus Photography | Colour digital | Drusen grading, baseline documentation, hemorrhage | Always |
| OCT (SD-OCT / SS-OCT) ⭐ | Near-IR interferometry | Cross-section: SRF, IRF, PED, EZ integrity, drusen volume, ORT | Gold standard — every visit |
| FFA | Fluorescein dye IV | Classic vs occult CNV; leakage type/extent; CNV eligibility for trials | Wet AMD diagnosis/classification |
| ICGA | Indocyanine green IV | Choroidal circulation; polyp identification; Type 1 CNV plaque | PCV suspected; occult CNV |
| FAF | Lipofuscin autofluorescence (488 nm excitation) | GA extent + margins; RPE viability; junctional zone patterns (prognostic) | Dry AMD monitoring |
| OCT-A ⭐ | Red blood cell movement detection | Non-invasive MNV mapping; choriocapillaris assessment; flow index | Wet AMD — see slide 14 |
| Near-infrared reflectance | 820 nm reflectance | SDD/reticular pseudodrusen detection (best modality for SDD) | Intermediate AMD workup |
| Amsler Grid | 10° central field | Metamorphopsia detection; home monitoring | All AMD patients |
| ForeseeHome (PHP) | Preferential hyperacuity perimetry | FDA-cleared home monitoring; early CNV detection; telemedicine | Intermediate AMD |
📌 SLIDE 14 — OCT IN AMD: DETAILED GUIDE
Key OCT Findings in Dry AMD
| Finding | Appearance on OCT | Significance |
|---|
| Drusen | Subretinal elevations between EZ and RPE | Hallmark of AMD; soft > hard = higher risk |
| Hyperreflective foci (HRF) | Small hyperreflective dots in various retinal layers | Migrating RPE cells; strongest single predictor of progression to late AMD; each additional intraretinal HRF → 1.3× increased odds of GA |
| Geographic Atrophy | Choroidal hypertransmission (signal shadow lost); loss of RPE band + EZ; ONL thinning | Extent measured by FAF; confirmed by OCT |
| Outer Retinal Tubulation (ORT) ⭐ | Hyperreflective ring surrounding hyporeflective tubular cavity within ONL | Degenerate cones + Muller cells; present in advanced GA and post-fibrosis nAMD; NOT the same as cystoid spaces |
| BlamD/BLinD ⭐ | Diffuse thickening between RPE and Bruch's | Sub-RPE deposits; OCT cannot reliably distinguish types (histology needed) |
| SDD (Subretinal drusenoid deposits) ⭐ | Subretinal deposits (ABOVE RPE, distinct from drusen); hyporeflective on FAF | Associated with Type 3 MNV and faster GA; best detected on NIR reflectance + SS-OCT |
Key OCT Findings in Wet AMD
| Finding | OCT Appearance | Clinical Meaning |
|---|
| SRF (subretinal fluid) | Hyporeflective space between EZ and RPE | Active exudation from MNV |
| IRF (intraretinal fluid) | Hyporeflective cystoid spaces within retinal layers | Indicates active CNV; may be tolerated in T&E if small |
| PED | RPE elevation; variable internal reflectivity | Type guides diagnosis (serous=empty; fibrovascular=irregular; drusenoid=homogeneous) |
| SHRM (subretinal hyperreflective material) | Hyperreflective material above RPE | Represents fibrin, blood, or Type 2 MNV |
| Macular atrophy (MA) | Choroidal hypertransmission + EZ loss + RPE loss | Develops in ~29% at 2 years under anti-VEGF (meta-analysis 2025, PMID 39842718) |
| Disciform scar | Hyperreflective subretinal mass; retinal tubules | End-stage; VA rarely better than 6/60 |
| RPE tear | Scrolled/bunched RPE; bare Bruch's membrane area visible | Complication of PED treatment; predictors: PED height >400 μm |
📌 SLIDE 15 — OCT-A IN AMD ⭐ (KEY NEW CONTENT — Ryan's Ch. 67 + Kanski + Novarese 2026)
Technical Principle (Kanski, line 2933)
"OCT-A detects red blood cell movement within microvasculature using serial OCT B-scans at the same retinal position. Differences between scans generate detectable contrast as red cells move. A 2D map of microcirculation within retinal/choroidal layers is created."
KEY LIMITATION: It is flow (not vessel walls) that is visualized. Flow too slow or too fast may NOT be detected.
OCT-A Advantages over FFA
- Non-invasive (no dye injection)
- Simultaneous structural + vascular information
- Choroidal visualization without ICGA
- Quantification of MNV area and morphology
- Detects non-exudative (quiescent) MNV invisible on FFA
OCT-A Appearances by MNV Type (Ryan's Ch. 67)
TYPE 1 MNV (sub-RPE slab):
┌─────────────────────────────────────────────────────┐
│ GLOMERULUS or MEDUSA shape (tangled vessel loops) │
│ Often smaller on OCT-A than FFA-based estimate │
│ (FFA dye leakage artificially enlarges lesion) │
│ Detectable as quiescent/non-exudative MNV │
└─────────────────────────────────────────────────────┘
TYPE 2 MNV (outer retina slab):
┌─────────────────────────────────────────────────────┐
│ Fine, immature, indistinct vessel network above RPE│
│ Corresponds to classic CNV on FFA │
│ Associated with SHRM on structural OCT │
└─────────────────────────────────────────────────────┘
TYPE 3 MNV (intraretinal slab):
┌─────────────────────────────────────────────────────┐
│ TUFT-LIKE focal intraretinal capillary network │
│ Nascent Type 3 = intraretinal hyperreflective foci │
│ WITH flow signal │
│ Confirmed by B-scan overlay showing lesion │
└─────────────────────────────────────────────────────┘
Five OCT-A Features of ACTIVE MNV (Ryan's Ch. 67)
| Feature | Active | Inactive/Fibrosed |
|---|
| 1. Vessel morphology | Sea-fan / medusa / glomerulus | "Dead tree" / arborizing without loops |
| 2. Capillary density | Numerous small branching capillaries | Fewer, larger vessels |
| 3. Anastomoses | Present (loops, arcade) | Absent |
| 4. Peripheral arcade | Present at vessel terminus | Absent |
| 5. Perilesional halo | Hypointense dark halo on choriocapillaris slab | Absent |
Choriocapillaris on OCT-A in nAMD ⭐
- Characteristic "dark halo" (ring-shaped choriocapillaris hypoperfusion) surrounding MNV
- Flow deficit greater in concentric rings around Type 1 MNV
- Pathogenesis: ischemia, mechanical compression, or "steal phenomenon"
- Prognostic: larger CC flow deficits → worse visual outcomes
Standardization Gap (Novarese et al. 2026, PMID 42107776)
Systematic review of 155 studies, 9,025 patients: marked heterogeneity in devices (SD-OCT vs SS-OCT), scan sizes (3×3 vs 6×6 mm), segmentation, binarization, artifact correction. Standardized protocols urgently needed for reproducible MNV biomarker development.
📌 SLIDE 16 — FAF PATTERNS IN GA — JUNCTIONAL ZONE ⭐ (Kanski + Ryan's Ch. 66)
FAF Classification at GA Margin (Junctional Zone)
┌─────────────────────────────────────────────────────────────────┐
│ Is there any INCREASED FAF at the junctional zone? │
└──────────────┬───────────────────┬──────────────────────────────┘
│YES │NO
▼ ▼
Configuration? NONE pattern
(adjacent to GA margin) → SLOW progression rate
│
┌──────────┼─────────────────────────────────┐
▼ ▼ ▼ ▼
FOCAL BANDED PATCHY DIFFUSE
(small (almost (individual (increased FAF
spots) continuous large spots) elsewhere too)
ring)
↑ ↑ ↑ ↑
SLOW SLOW INTERMEDIATE FASTEST
progression progression progression PROGRESSION
RATE
Subtypes of DIFFUSE Pattern (fastest progression)
Granular | Branching | Trickling | Reticular | Fine granular with punctuated spots
Clinical key: Diffuse FAF at junctional zone = highest risk of rapid GA expansion. Used in clinical trials (OAKS, DERBY, GATHER1/2) as secondary endpoint.
📌 SLIDE 17 — DRY AMD MANAGEMENT FLOWCHART
╔═════════════════════════════════════════════════════════════════╗
║ DRY AMD MANAGEMENT PATHWAY ║
╚═════════════════════════════════════════════════════════════════╝
EARLY DRY AMD (small/medium drusen, no central symptoms)
│
▼
┌──────────────────────────────────┐
│ LIFESTYLE MODIFICATION │
│ ● STOP SMOKING ← MOST IMPORTANT│
│ ● Mediterranean diet │
│ ● UV-blocking sunglasses │
│ ● Control BP, BS, lipids │
│ ● Regular aerobic exercise │
└──────────────┬───────────────────┘
│
▼
INTERMEDIATE DRY AMD (large drusen ≥125 μm OR pigment changes)
│
▼
┌──────────────────────────────────────────────────────────┐
│ AREDS2 SUPPLEMENTS (daily oral) │
│ │
│ Vitamin C 500 mg │
│ Vitamin E 400 IU │
│ Lutein 10 mg ← replaces beta-carotene │
│ Zeaxanthin 2 mg ← replaces beta-carotene │
│ Zinc oxide 80 mg │
│ Cupric oxide 2 mg (prevents zinc-induced anemia)│
│ │
│ ⚠ AVOID beta-carotene in smokers/ex-smokers │
│ → 28% increased lung cancer risk (ATBC/CARET trials) │
└──────────────┬───────────────────────────────────────────┘
│
▼
┌──────────────────────────────────┐
│ HOME MONITORING │
│ Daily Amsler grid │
│ ± ForeseeHome PHP device │
│ NEW: AI-driven home OCT ←2026 │
│ Any new metamorphopsia → │
│ URGENT CLINIC REVIEW (same week)│
└──────────────┬───────────────────┘
│
▼
ADVANCED DRY AMD — GEOGRAPHIC ATROPHY
│
▼
┌────────────────────────────────────────────────────────────────┐
│ COMPLEMENT INHIBITORS (FDA APPROVED 2023) │
│ │
│ Pegcetacoplan (Syfovre, Apellis) │
│ • C3 inhibitor (intravitreal) │
│ • Monthly or every-other-month injection │
│ • OAKS trial: ~22% (monthly) / 18% (EOM) reduction in GA │
│ growth vs. sham at 24 months │
│ • ⚠ Increased risk of exudative conversion in treated eyes │
│ │
│ Avacincaptad pegol (Izervay, Iveric Bio/Astellas) │
│ • C5 inhibitor (intravitreal) │
│ • Monthly injection │
│ • GATHER2: 14.5% reduction in GA growth; foveal sparing │
│ preserved │
│ • FDA approved August 2023 │
└──────────────┬─────────────────────────────────────────────────┘
│
▼
┌──────────────────────────────────┐
│ LOW VISION REHABILITATION │
│ Magnification aids │
│ Eccentric fixation training │
│ Electronic magnifiers │
│ Psychological support │
│ Macular Society registration │
└──────────────────────────────────┘
AREDS Trial Summary
| Trial | Year | N | Intervention | Key Finding |
|---|
| AREDS | 2001 | 4,757 | Vit C/E + beta-carotene + zinc | 25% ↓ progression to advanced AMD (NNT ~8 over 5yr) |
| AREDS2 | 2013 | 4,203 | Lutein/zeaxanthin replacing beta-carotene | Similar efficacy; safer in smokers; no lung cancer risk increase |
📌 SLIDE 18 — WET AMD MANAGEMENT FLOWCHART
╔═══════════════════════════════════════════════════════════════╗
║ WET AMD MANAGEMENT — TREAT-AND-EXTEND ║
╚═══════════════════════════════════════════════════════════════╝
STEP 1: CONFIRM WET AMD
OCT (SRF/IRF/PED) + BCVA + FFA/OCT-A
│
▼
STEP 2: LOADING PHASE — 3 MONTHLY IVT INJECTIONS
(Faricimab 6 mg OR Aflibercept 8 mg first-line — 2025 guidelines)
│
▼
STEP 3: ASSESS RESPONSE ON OCT AT EACH VISIT
│
┌────┴──────────────────────────────┐
▼ ▼
MACULA DRY (no SRF/IRF) FLUID PRESENT (SRF or IRF)
│ │
▼ ▼
EXTEND interval +2 weeks MAINTAIN or SHORTEN -2 weeks
(Q6w→Q8w→Q10w→Q12w→Q16w) Re-assess next visit
│
└──────────────────────────────────┐
▼
PERSISTENT FLUID at maximum interval (Q4w)
│
▼
SWITCH anti-VEGF agent
(e.g., ranibizumab → faricimab →
aflibercept 8 mg)
│
▼
REASSESS after 3 injections of new agent
TREATMENT GOALS:
● Anatomically dry macula on OCT (no SRF, ideally no IRF)
● Maintain or improve BCVA
● Reduce injection burden while maintaining disease control
📌 SLIDE 19 — ANTI-VEGF AGENTS (Complete Reference)
Currently Approved Agents (2025)
| Drug | Type | Target | Dose | Approval | Key Trials |
|---|
| Pegaptanib (Macugen) | Aptamer | VEGF165 only | 0.3 mg IVT Q6w | 2004 | VISION; largely superseded |
| Ranibizumab (Lucentis) | Fab fragment | All VEGF-A isoforms | 0.5 mg IVT | 2006 | MARINA, ANCHOR |
| Bevacizumab (Avastin) | Full IgG1 Ab | All VEGF-A | 1.25 mg IVT | Off-label | CATT — non-inferior to ranibizumab |
| Aflibercept 2 mg (Eylea) | Fusion protein (decoy receptor) | VEGF-A, VEGF-B, PlGF | 2 mg IVT | 2011 | VIEW 1&2 — Q8w non-inferior to monthly ranibizumab |
| Brolucizumab (Beovu) | Single-chain Fv (scFv) | Pan-VEGF-A | 6 mg IVT | 2019 | HAWK/HARRIER — Q12w in 56%; ⚠ retinal vasculitis 1–3.3% |
| Aflibercept 8 mg (Eylea HD) | Fusion protein | Same as above | 8 mg IVT | 2023 | PULSAR — Q12–16w; 80% on extended dosing |
| Faricimab (Vabysmo) ⭐ | Bispecific IgG Ab | Anti-VEGF-A + Anti-Ang-2 | 6 mg IVT | 2022 | TENAYA/LUCERNE — up to Q16w; 80% on ≥Q12w |
Molecular Comparison
MOLECULAR SIZE (smallest → largest):
brolucizumab (26 kDa) < ranibizumab (48 kDa) < aflibercept (97 kDa) < bevacizumab (149 kDa)
MOLAR DOSE (relative to aflibercept):
brolucizumab: 11× > ranibizumab: ~5× > aflibercept: 1× > bevacizumab: ~1×
OCULAR HALF-LIFE:
faricimab/brolucizumab > aflibercept (9d) > ranibizumab (7d) > bevacizumab
Landmark Trial Results
| Trial | Drug vs. Control | N | Key Result |
|---|
| MARINA (2006) | Ranibizumab 0.3/0.5 mg vs sham | 716 | 95% maintained vision; 35% gained ≥15 letters (vs 5% sham) |
| ANCHOR (2006) | Ranibizumab vs PDT | 423 | Ranibizumab superior in all outcomes; established anti-VEGF as standard |
| CATT (2011) | Ranibizumab vs bevacizumab | 1,208 | Bevacizumab non-inferior at 2 years; ~$50 vs ~$2000/injection; major cost implications |
| VIEW 1&2 (2012) | Aflibercept vs ranibizumab | 2,457 | Q8w aflibercept non-inferior; first extended dosing |
| HAWK/HARRIER (2019) | Brolucizumab vs aflibercept | 1,817 | Non-inferior; 56% on Q12w; ⚠ post-marketing vasculitis signal |
| TENAYA/LUCERNE (2022) | Faricimab vs aflibercept | 1,329 | Non-inferior; ~80% on ≥Q12w; bispecific Ang-2+VEGF validated → FDA Jan 2022 |
| PULSAR (2023) | Aflibercept 8 mg vs 2 mg | 669 | Q12–16w achieved; non-inferior → FDA Aug 2023 |
📌 SLIDE 20 — ANTI-VEGF MECHANISM & ANG-2 PATHWAY ⭐
╔══════════════════════════════════════════════════════════════╗
║ VEGF + ANGIOPOIETIN SIGNALING IN AMD ║
╚══════════════════════════════════════════════════════════════╝
NORMAL STATE:
Pericytes → constitutively release ANG-1 → binds TIE-2
→ vascular stability, anti-inflammatory, survival signaling
AMD/HYPOXIA STATE:
↑ ANG-2 (released from Weibel-Palade bodies on inflammation)
→ ANG-2 competes with ANG-1 at TIE-2
→ TIE-2 signaling blocked
→ Pericyte detachment + vessel destabilization
→ SENSITIZES endothelium to VEGF-A effects
ANG-2 + VEGF-A
│ │
▼ ▼
TIE-2 blocked VEGFR-1/VEGFR-2
(destabilization) (angiogenesis + permeability)
│ │
└───────────┬───────────┘
▼
CNV GROWTH + FLUID LEAK
FARICIMAB:
Blocks ANG-2 + Blocks VEGF-A
│ │
▼ ▼
TIE-2 re-activated CNV halted
(vessel stability) (fluid resolved)
│
▼
LONGER TREATMENT INTERVALS (Q16w) vs single anti-VEGF
📌 SLIDE 21 — PDT & THERMAL LASER (Historical + Current Role)
Photodynamic Therapy (PDT) — Verteporfin
| Parameter | Detail |
|---|
| Drug | Verteporfin (Visudyne) 6 mg/m² IV |
| Mechanism | 689 nm non-thermal laser → free radical generation → platelet activation → thrombotic occlusion of CNV |
| Half-life | 5–6 hours; excreted in feces |
| Side effects | Photosensitization (avoid sunlight 5 days); transient visual disturbance; back pain |
| Current role | Limited in anti-VEGF era; combination with anti-VEGF in PCV (EVEREST II trial) |
Thermal Laser Photocoagulation
- Thermal destruction of well-defined extrafoveal classic CNV (Type 2)
- Rarely used today; MPS (Macular Photocoagulation Study) showed benefit only for classic extrafoveal CNV
- Risk: scotoma at treatment site; CNV recurrence
📌 SLIDE 22 — COMPLICATIONS OF ANTI-VEGF THERAPY
Ocular Complications
| Complication | Frequency | Notes |
|---|
| Endophthalmitis | 0.02–0.05%/injection | Most common serious complication |
| RPE tear | ~2–5% in eyes with large PED | Predictors: PED height >400 μm, brolucizumab, aggressive treatment |
| Sustained IOP elevation | ~3–5% | May require glaucoma treatment |
| Sterile uveitis | ~1% | More common with brolucizumab |
| Retinal vasculitis/occlusion | Brolucizumab: 0.74% | Post-marketing signal; ASRS review March 2020 |
| Macular atrophy (MA) ⭐ | ~29% at 2 years | Meta-analysis (Berni et al. 2025, PMID 39842718); Type 3 MNV highest risk (49%) |
| Subretinal fibrosis | Variable | Related to prolonged active CNV; fibrocellular phenotype |
Macular Atrophy — Three Mechanisms (Ryan's Ch. 67)
1. Natural progression of concomitant DRY AMD (ongoing complement damage)
+
2. MNV regression → fibrocellular replacement → contraction → photoreceptor loss
+
3. Interference with basal RPE nutrition (anti-VEGF suppresses VEGF-dependent
choriocapillaris fenestrations → RPE hypoxia)
📌 SLIDE 23 — GEOGRAPHIC ATROPHY: TREATMENT TRIALS (2023–2025)
| Drug | Mechanism | Trial | N | Result | Status |
|---|
| Pegcetacoplan (Syfovre) | C3 inhibitor IVT | OAKS/DERBY | 637 | 22% (monthly) / 18% (EOM) ↓ GA growth vs. sham at 24 months | FDA approved Feb 2023 |
| Avacincaptad pegol (Izervay) | C5 inhibitor IVT | GATHER1/2 | ~500 | 14.5% ↓ GA growth; foveal sparing preserved | FDA approved Aug 2023 |
| Tinlarebant (oral) | RBP4 inhibitor → ↓ retinol delivery to RPE → ↓ A2E | PHOENIX | ~500 | Phase 3 ongoing (2025) | Investigational |
| OCU410 | Nuclear receptor modifier (RORA gene) gene therapy IVT | ArMaDa | ~60 | Phase 1/2 ongoing | Investigational |
| VOY-101 | C3 inhibitor gene therapy | JOURNEY | — | Phase 1/2 | Investigational |
| BI 771716 | Novel complement target | VERDANT | — | Active Phase 2 vs. pegcetacoplan | Investigational |
| Elamipretide | Mitochondrial peptide | ReNEW | — | Phase 3 | Investigational |
Rationale: CFH/CFI genetic variants → insufficient complement regulation → excess C3/C5 activation → RPE destruction → GA progression. Blocking C3 (upstream, broader) or C5 (downstream, more specific) slows this cascade.
📌 SLIDE 24 — GENE THERAPY PIPELINE (2025)
╔═══════════════════════════════════════════════════════════════════╗
║ GENE THERAPY FOR AMD — CONCEPT ║
║ Single IVT injection of AAV vector → transfects retinal cells ║
║ → Continuous therapeutic protein production ║
║ → ELIMINATES monthly injection burden ║
╚═══════════════════════════════════════════════════════════════════╝
| Agent | Company | Vector | Target | Route | Trial | Phase |
|---|
| RGX-314 | AbbVie/RegenxBio | AAV8-anti-VEGF (ranibizumab-like Fab) | VEGF | Subretinal / suprachoroidal | AAVIATE, ASCENT | Phase 3 (n=500) |
| ADVM-022 / Ixo-vec | Adverum Biotechnologies | AAV.7m8-anti-VEGF | VEGF | IVT single injection | LUNA, ARTEMIS | Phase 3 (n=400) |
| 4D-150 | 4D Molecular Therapeutics | AAVv66-anti-VEGF + VEGF-C RNAi | VEGF + VEGF-C | IVT single | PRISM, 4FRONT | Phase 3 (n=400) |
| OCU410 | Ocugen | Nuclear receptor modifier (RORA) | Complement/RPE | IVT | ArMaDa | Phase 1/2 |
| VOY-101 | Voyager | C3 inhibitor gene therapy | Complement C3 | IVT | JOURNEY | Phase 1/2 |
| LX102-C01 | Lees Pharmaceutical | Anti-VEGF gene therapy | VEGF | IVT | Phase 1 | 12-month safety data published 2025 |
If successful: One injection every 2–5 years vs. current 6–12 injections per year
📌 SLIDE 25 — EMERGING THERAPIES (Non-Gene, 2025)
| Category | Agent | Target | Route | Status |
|---|
| Sustained-release TKI | EYP-1901 (Vorolanib) | VEGFR TKI implant | Biodegradable IVT | LUCIA/LUGANO Phase 3 (2025) |
| Sustained-release TKI | OTX-TKI (Axitinib) | VEGFR TKI depot | Biodegradable hydrogel IVT | Phase 3 (2025); SOL-1 trial: superior to aflibercept in wet AMD |
| Bispecific integrin | AXT107 (AsclepiX) | VEGFR2 + αvβ3 integrin | IVT | DISCOVER Phase 1/2 |
| Port Delivery System | PDS + ranibizumab | VEGF (sustained) | Refillable scleral implant | ARCHWAY Phase 3; median refill interval 13 months |
| Stem cell / iPSC | iPSC-derived RPE cells | Replace diseased RPE | Subretinal | Early clinical trials (Japan/UK) |
| Photobiomodulation | LumiThera device | Mitochondria (670 nm) | Non-invasive | Phase 3 NCT04065490 |
| Oral RPE protection | Tinlarebant | RBP4 → ↓ A2E | Oral daily | PHOENIX Phase 3 (2025) |
| Home OCT + AI | AI-OCT platforms | Fluid detection | Telemedicine | Entering clinical integration (2025–2026) |
📌 SLIDE 26 — 2026 LATEST EVIDENCE ⭐ (AI + OCT-A)
Top 2026 Studies on OCT-A in Wet AMD
1. AI-Based Treatment Response via Paired OCT-A (Morsy et al., Sci Rep 2026)
AI analysis of paired OCTA scans (pre- and post-treatment) outperformed experienced human graders in characterizing nAMD treatment response. AI quantified MNV vascular remodeling + fluid resolution. Potential to optimize retreatment intervals, detect early recurrence, enable personalized therapy.
2. Systematic Review: OCT-A MNV Standardization (Novarese et al., Ophthalmol Retina 2026, PMID 42107776)
155 studies, 9,025 patients. Marked heterogeneity in devices, scan protocols, segmentation, binarization, artifact correction. Standardized protocols urgently needed.
3. Pachychoroid Neovasculopathy Spectrum (Lingardo et al., Graefes 2026)
PNV frequently misdiagnosed as nAMD. Multimodal OCT-A essential to differentiate. Treatment strategy differs significantly from AMD-associated CNV.
4. Macular Atrophy Meta-Analysis (Berni et al., Ophthalmol Retina 2025, PMID 39842718)
23 studies, 3,013 eyes. Pooled 24-month MA incidence: 29%. Type 3 MNV: 49%. Low certainty of evidence highlights need for better OCT-A biomarkers.
📌 SLIDE 27 — DIFFERENTIAL DIAGNOSIS
| Condition | Age | Drusen | Features that Distinguish |
|---|
| Dry AMD | ≥55 | Central bilateral | Slow progression, AREDS staging, complement genetics |
| Wet AMD | ≥55 | Usually present | Sudden vision loss, SRF/IRF/PED on OCT, CNV |
| Myopic degeneration | Any | No | High myopia, lacquer cracks, peripapillary changes, CNV without drusen |
| CSCR (central serous) | <50, male | No | RPE/serous detachment; self-limiting; subretinal fluid resolves |
| Stargardt disease | <50 | Flecks (not drusen) | ABCA4 mutation; dark choroid on FFA; "beaten bronze" appearance |
| Pattern dystrophy | Variable | No | Bilateral macular pigment changes, FAF characteristic butterfly/vitelliform pattern |
| Chloroquine toxicity | Any | No | Bull's-eye maculopathy; drug history; ring scotoma |
| Angioid streaks | Any | No | Subretinal red-brown bands radiating from disc; PXE, Paget's, sickle cell |
| PCV/IPCV | ≥50, Asian | Sometimes | Serosanguineous PED; polyps on ICGA; no typical AMD drusen |
| Ocular histoplasmosis | Any | No | White chorioretinal scars, peripapillary atrophy, endemic region |
| MacTel type 2 | 40s–50s | No | Bilateral perifoveal telangiectasia; right-angle vessels; crystalline deposits; EZ loss on OCT |
📌 SLIDE 28 — MONITORING PROTOCOL
| AMD Stage | Frequency | Imaging Required | Action Threshold |
|---|
| Early dry | Annual | Dilated exam + OCT | Metamorphopsia → urgent |
| Intermediate dry | Every 6 months | OCT + FAF + daily Amsler | Any new symptom → same-week review |
| Advanced dry (GA) | Every 3–6 months | OCT + FAF (GA area measurement) | Consider complement inhibitor; low vision referral |
| Wet AMD — on treatment | Per T&E protocol (Q4w–Q16w) | OCT + BCVA every visit | Recurrent fluid → shorten interval; non-response → switch drug |
| Fellow eye monitoring | Every 3–6 months | OCT + Amsler | CNV in fellow eye → urgent treatment |
Home Monitoring Devices
| Device | Mechanism | Sensitivity | Notes |
|---|
| Amsler Grid | 10° central field distortion | Moderate | Free, instant, daily; limited sensitivity for early CNV |
| ForeseeHome PHP | Preferential hyperacuity perimetry | High (sensitivity 78%, specificity 84%) | FDA-cleared; detects CNV at better BCVA than controls; telemedicine link |
| Home OCT (AI-driven) | Self-administered SD-OCT + AI analysis | Very high (2025 data) | AI reliably monitors disease activity; Protocol AO trial (Retina World Congress 2026) |
📌 SLIDE 29 — PROGNOSIS
| Scenario | Prognosis |
|---|
| Dry AMD — early/intermediate | Slow progression; AREDS2 supplements reduce conversion risk by 25% |
| Dry AMD — geographic atrophy | Progressive; no cure; complement inhibitors slow growth ~15–22%; foveal involvement → severe VA loss |
| Wet AMD — untreated | 60–70% lose ≥3 lines of vision within 2 years |
| Wet AMD — with anti-VEGF (current best) | ~95% maintain vision; 30–40% gain ≥15 letters (3 lines) |
| Wet AMD — gene therapy (future) | Long-term single-injection control — Phase 3 results awaited 2026–2027 |
Predictors of Poor Visual Outcome (Kanski Ch. 14 / Ryan's Ch. 67)
- Late presentation (>6 weeks from symptom onset)
- Large subretinal hemorrhage (>4 disc areas)
- Subfoveal CNV at baseline
- Subretinal fibrosis / disciform scar
- Poor anti-VEGF response after 3 loading doses
- Development of macular atrophy
- Intraretinal hyperreflective foci at baseline (strongest predictor of MA)
📌 SLIDE 30 — KEY MNEMONICS & REVISION SUMMARY
DRUSEN Mnemonic
D — Deposits (extracellular between RPE and Bruch's)
R — Risk: size matters (>125 μm = high risk)
U — Unesterified cholesterol (SDD) vs. esterified (soft drusen)
S — Soft → GA; SDD → Type 3 MNV
E — Early AMD: small drusen only = low risk
N — Neovascular risk: large + bilateral + pigment = 50% in 5 years
ANTI-VEGF Mnemonic — "PReBFA"
P egaptanib → 2004 → VEGF165 only
R anibizumab → 2006 → MARINA/ANCHOR
e Bevacizumab → off-label → CATT
F libercept (Afl 2 mg) → 2011 → VIEW 1&2
A fli 8 mg + Brolucizumab → 2023/2019 → PULSAR/HAWK
Faricimab → 2022 → TENAYA/LUCERNE → dual VEGF+Ang-2
OCT-A Activity: 5 Features — "SCAPH"
S ea-fan/medusa morphology
C apillaries numerous + small
A nastomoses present
P eripheral arcade at terminus
H alo (perilesional dark halo on CC slab)
GA FAF Progression — BPDNF (slowest to fastest)
None → Focal → Banded → Patchy → Diffuse ← fastest
📌 SLIDE 31 — LOW VISION REHABILITATION
Optical Aids
- High-plus reading glasses (up to +20D)
- Hand/stand magnifiers
- Binoculars for distance viewing
Electronic Aids
- Video magnifiers (CCTV systems)
- E-readers with adjustable font size
- Screen-reading software (iOS VoiceOver, Android TalkBack)
- Smartphones with AI scene description
Rehabilitative Training
- Eccentric fixation training — using parafoveal/peripheral retina for tasks previously performed by fovea
- Orientation and mobility training
- Kitchen and daily living adaptations (high-contrast utensils, improved lighting)
- Implantable Miniature Telescope (IMT) — 2.2–2.7× magnification; for bilateral advanced AMD with stable disciform scar; Phase 3 trial: 67% gained ≥3 lines vs 13% fellow eye
Psychological Support
- Depression is common (up to 30% of AMD patients with severe visual loss)
- CBT, peer support groups, Macular Society
- Legal registration as visually impaired; DVLA/DMV driving regulations
📌 SLIDE 32 — SOURCES & REFERENCES
STANDARD TEXTBOOK SOURCES:
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
1. Kanski's Clinical Ophthalmology, 10th Ed (2023, Elsevier)
Ch. 14 — Macular Degeneration (pp. 580–620)
2. Ryan's Retina, 3rd Edition — Chapters 64, 65, 66, 67, 68:
Ch.64: Epidemiology & Risk Factors (Seddon, Sobrin, Davoudi)
Ch.65: Pathogenesis (Curcio, Spaide)
Ch.66: Non-Neovascular AMD & GA (Chaikitmongkol, Bressler)
Ch.67: Neovascular AMD (Borrelli, Soueid, Querques)
Ch.68: Pharmacotherapy of AMD (Budoff, Leung, Kaiser, Dugel)
3. Wills Eye Manual, 7th Edition — Sections 11.16 & 11.17
4. Goodman & Gilman's Pharmacological Basis, Ch. 74
5. Harrison's Principles of Internal Medicine, 22nd Ed, Ch. 391
KEY CLINICAL TRIALS:
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
AREDS (2001), AREDS2 (2013), MARINA (2006), ANCHOR (2006),
CATT (2011), VIEW 1&2 (2012), HAWK/HARRIER (2019),
TENAYA/LUCERNE (2022), PULSAR (2023), OAKS/DERBY (2023),
GATHER1/2 (2021–23), AVONELLE-X (2025), SOL-1 (2026)
2025–2026 LITERATURE:
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
• Morsy et al. Sci Rep 16:15405 (2026) — AI + paired OCTA
• Novarese et al. Ophthalmol Retina (2026) PMID 42107776
— OCT-A standardization systematic review
• Berni et al. Ophthalmol Retina (2025) PMID 39842718
— Macular atrophy meta-analysis
• Lingardo et al. Graefes (2026) PMID 41385093
— Pachychoroid neovasculopathy spectrum
• Hormel & Jia. Taiwan J Ophthalmol (2025) PMID 40995309
— Advancing OCTA to clinic
📌 ADDITIONAL FINDINGS NOTE (Gap Additions from Ryan's + Kanski)
The following topics were absent from prior presentations and are now integrated above:
- ✅ Subretinal drusenoid deposits (SDD/reticular pseudodrusen) — Slide 7 — distinct entity from soft drusen; unesterified cholesterol only; follows rod topography; associated with Type 3 MNV; worsened by laser; detected on NIR reflectance + SS-OCT
- ✅ Non-exudative (quiescent) Type 1 MNV — Slide 11 — may be biologically protective; does not automatically require treatment
- ✅ OCT-A technical principle + limitation — Slide 15 — flow, not vessel walls; too slow/fast flow undetected (Kanski only)
- ✅ Five OCT-A features of MNV activity (SCAPH) — Slide 15 — sea-fan, capillaries, anastomoses, peripheral arcade, halo
- ✅ Choriocapillaris dark halo on OCT-A — Slide 15 — ring-shaped hypoperfusion; prognostic
- ✅ FAF junctional zone patterns — Slide 16 — None/Focal/Banded/Patchy/Diffuse; Diffuse = fastest GA progression
- ✅ Drusenoid PED — Slide 7 — confluent soft drusen; 75% → GA; 25% → MNV by 10 years; homogeneous on OCT; no SRF
- ✅ BlamD vs. BLinD histopathology — Slide 14 — BlamD internal to RPE-BL; BLinD external; OCT cannot reliably distinguish
- ✅ Outer retinal tubulation (ORT) — Slide 14 — hyperreflective ring around hyporeflective tubule; degenerate cones + Muller cells; distinct from cystoid spaces
- ✅ RPE tears — Slide 22 — predictors: PED height >400 μm; scrolled RPE on OCT; bare Bruch's membrane
- ✅ PCV as pachychoroid / Type 1 aneurysmal MNV — Slide 12 — ICGA gold standard; PDT+anti-VEGF combination
- ✅ Macular atrophy mechanisms (3 pathways) — Slide 22 — complement damage + fibrosis + anti-VEGF on CC fenestrations
- ✅ Angiopoietin/TIE-2 biology — Slide 20 — full Ang-1/Ang-2/TIE-2 mechanism rationale for faricimab
- ✅ Port Delivery System (PDS) — Slide 25 — refillable scleral implant; 13-month median refill interval
- ✅ AREDS simplified 4-point risk score — Slide 4 — 0 to 50% 5-year risk; validated clinical tool
- ✅ SRF patterns in non-nAMD (3 patterns) — Slide 14 — SRF above drusenoid PED crest; drape over drusen; SRF in crypts
This completes the 32-slide comprehensive AMD presentation from basic anatomy through 2026 cutting-edge evidence, incorporating all textbook gaps identified from Kanski's 10th edition and Ryan's Retina chapters 64–68. Every slide is ready to be reproduced as a PowerPoint using the content above.