Carcinoma of tongue anatomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a comprehensive anatomical overview of the tongue relevant to carcinoma, drawn from K.J. Lee's Essential Otolaryngology and Scott-Brown's Otorhinolaryngology Head & Neck Surgery.
Carcinoma of the Tongue - Anatomy
1. Divisions of the Tongue
The tongue is divided into two distinct anatomical and oncological regions:
| Region | Extent | Site Classification |
|---|---|---|
| Oral tongue (anterior 2/3) | Tip, dorsum, lateral borders, ventral surface - all anterior to the circumvallate papillae | Oral cavity (ICD-10 C02) |
| Base of tongue (posterior 1/3) | From circumvallate papillae to epiglottis | Oropharynx |
The sulcus terminalis marks the anterior boundary of the circumvallate papillae. The foramen cecum lies at its apex - the embryologic origin of the thyroid (source of lingual thyroid and thyroglossal duct cysts).
2. Mucosal Lining
- Lateral borders and ventral surface: lining (non-keratinizing stratified squamous epithelium) - continuous with floor of mouth. This is where most carcinomas arise.
- Dorsum and tip: specialized gustatory mucosa with thick, keratinized epithelium.
- Only 4-5% of tongue carcinomas occur on the dorsum; the majority arise on the lateral border of the middle third.
3. Papillae of the Tongue
| Papilla | Location | Function |
|---|---|---|
| Filiform | Bulk of anterior 2/3 | Tactile (no taste) - CN V endings |
| Fungiform | Diffuse, majority at anterior 2 cm | Taste buds on superior surface |
| Foliate | Lateral tongue | Taste buds on lateral surface |
| Circumvallate | V-shaped row at oral/base junction | Taste buds on lateral surface |
4. Muscles
Extrinsic Muscles (all CN XII except palatoglossus)
| Muscle | Origin | Insertion | Function | Nerve |
|---|---|---|---|---|
| Genioglossus | Mental spine of mandible | Hyoid + undersurface of tongue | Depress + protrude | CN XII |
| Hyoglossus | Body + greater cornu of hyoid | Side of tongue | Depress + retract | CN XII |
| Styloglossus | Styloid process | Tip + side of tongue | Retract + elevate | CN XII |
| Palatoglossus | Palatine aponeurosis | Side + dorsum of tongue | Elevate posterior tongue, close oropharyngeal isthmus | CN X (vagus) |
Intrinsic Muscles (CN XII)
Superior/inferior longitudinal, vertical, and transverse fibers - alter the shape of the tongue.
A fibrous midline septum (septum linguae) contains a triangular fat pad visible on axial CT - clinically important for assessing midline tumor extension.
Surgical relevance: Sacrifice of both hypoglossal nerves results in a non-functioning tongue tip with very poor functional outcome.
5. Vascular Supply
- Arterial: Lingual artery - the second branch of the external carotid artery (paired, one on each side).
- Venous: Lingual vein and the ranine vein (vena comitans of the hypoglossal nerve).
Surgical relevance: During resection of posterior tongue lesions, the contralateral vascular pedicle must be preserved if the tongue tip is to be maintained.
6. Innervation
Sensory Innervation
| Region | Modality | Nerve |
|---|---|---|
| Anterior 2/3 (oral tongue) | Touch, pain, temperature | Lingual nerve (CN V3) |
| Posterior 1/3 (tongue base) | Touch, gag (visceral afferent) | Glossopharyngeal nerve (CN IX) |
Taste Innervation
| Region | Pathway |
|---|---|
| Anterior 2/3 | Fungiform/foliate papillae → lingual nerve → chorda tympani (CN VII) → geniculate ganglion → nucleus solitarius |
| Posterior 1/3 | Foliate/circumvallate papillae → CN IX → inferior petrosal ganglion → nucleus solitarius |
Clinical relevance: Tongue base carcinoma invading CN IX causes referred otalgia (via Jacobson's nerve, tympanic branch of CN IX) - a key presenting symptom.
7. Lymphatic Drainage - Most Critical for Carcinoma
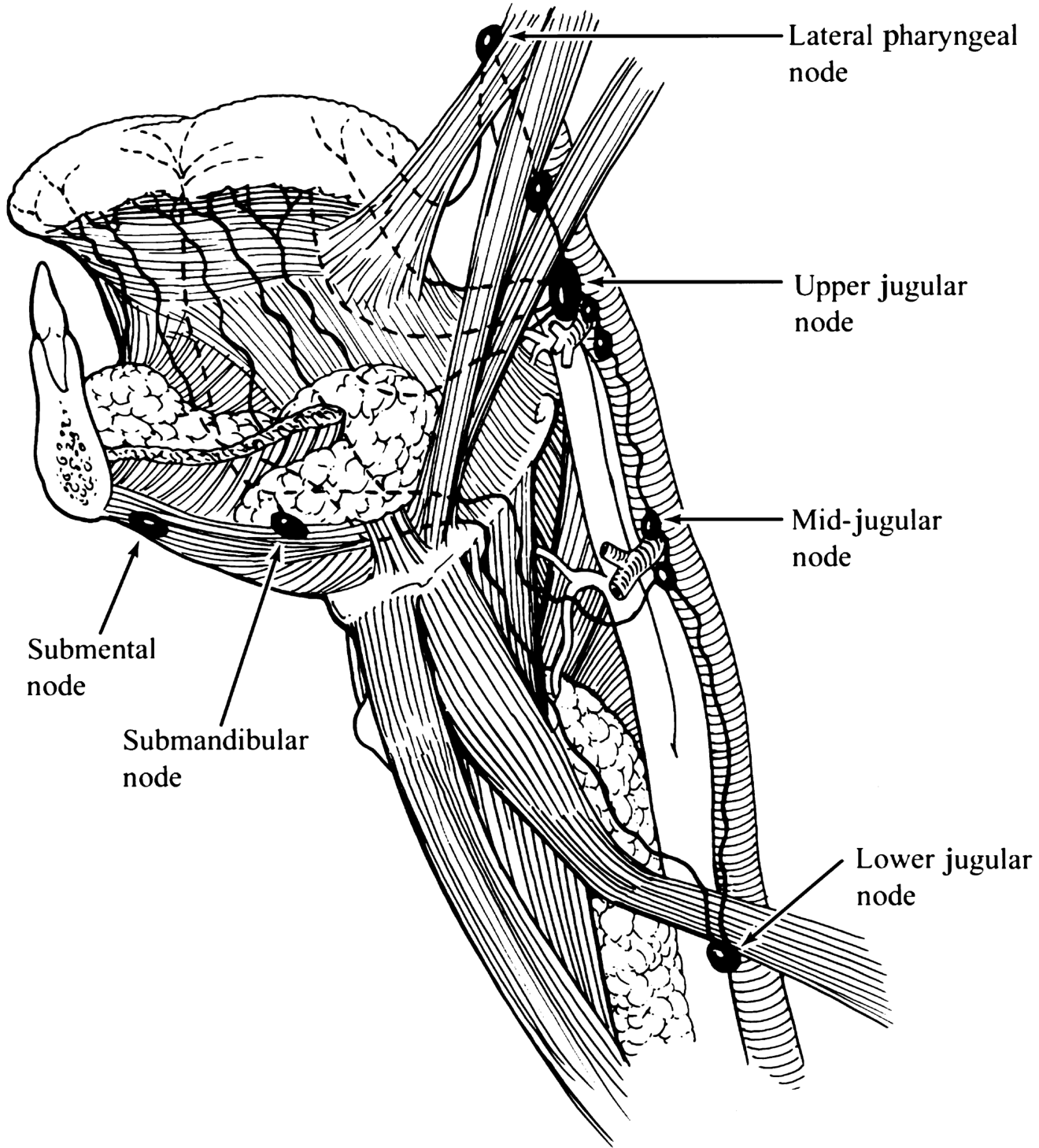
Lymphatic drainage of the oral tongue and oropharynx (K.J. Lee's Essential Otolaryngology)
| Site | Primary Drainage |
|---|---|
| Tip of tongue | Submental nodes (level IA) - bilaterally |
| Central tongue | Bilateral deep cervical nodes |
| Lateral border | Ipsilateral levels I-III (submental, submandibular, upper jugular); can have skip metastasis to level IV |
| Tongue base (posterior 1/3) | Bilaterally to levels II-IV (jugulodigastric and deep cervical) |
Key Clinical Points:
- Oral tongue: 25-33% of nodal metastases are clinically detectable; 20-25% are occult (hence elective neck dissection is often recommended even in N0 disease).
- Midline/ventral/base tumors carry a greater risk of bilateral nodal spread.
- Tongue base: >60% have clinically detectable cervical nodes at presentation; 20% are bilateral.
- Depth of invasion >2-4 mm correlates with higher rates of regional metastasis - this is why depth of invasion is now incorporated into the AJCC 8th edition T-staging (pT1 vs pT2 reclassification).
8. Anatomical Basis of Common Presentations
| Symptom | Anatomical Explanation |
|---|---|
| Tongue fixation | Invasion of intrinsic/extrinsic muscles or CN XII |
| Referred otalgia | CN IX involvement (base of tongue) or CN V3 (oral tongue) via auriculotemporal nerve |
| Dysphagia/dysarthria | Loss of tongue mobility, muscle invasion |
| Odynophagia | Base of tongue invasion with CN IX involvement |
| Bilateral nodal disease | Midline tumors draining bilaterally |
9. Site-Specific Oncological Points
- Oral tongue is the second most common site of oral cancer (~30%), after the buccal mucosa in tobacco-chewing populations.
- Most tumors arise on the lateral border of the middle third.
- The incidence of SCC in young patients without risk factors has risen significantly (4% in 1971 to 18% by 1993), with a postulated genetic susceptibility.
- Base of tongue SCC has a strong association with HPV (especially HPV-16); these patients often present with cervical lymphadenopathy and a small, occult primary - early detection is rare because the tongue base is poorly visualized.
Sources:
- K.J. Lee's Essential Otolaryngology, Chapter 45 (Carcinoma of the Oral Tongue, Base of Tongue, Anatomy of the Tongue)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Tongue Carcinoma - Surgical Anatomy section)
For mbbs 1st yesr
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is the MBBS 1st Year level anatomy of the tongue, focused on what is tested in exams - structured simply and clearly, sourced from Gray's Anatomy for Students.
Anatomy of the Tongue - MBBS 1st Year
Parts of the Tongue
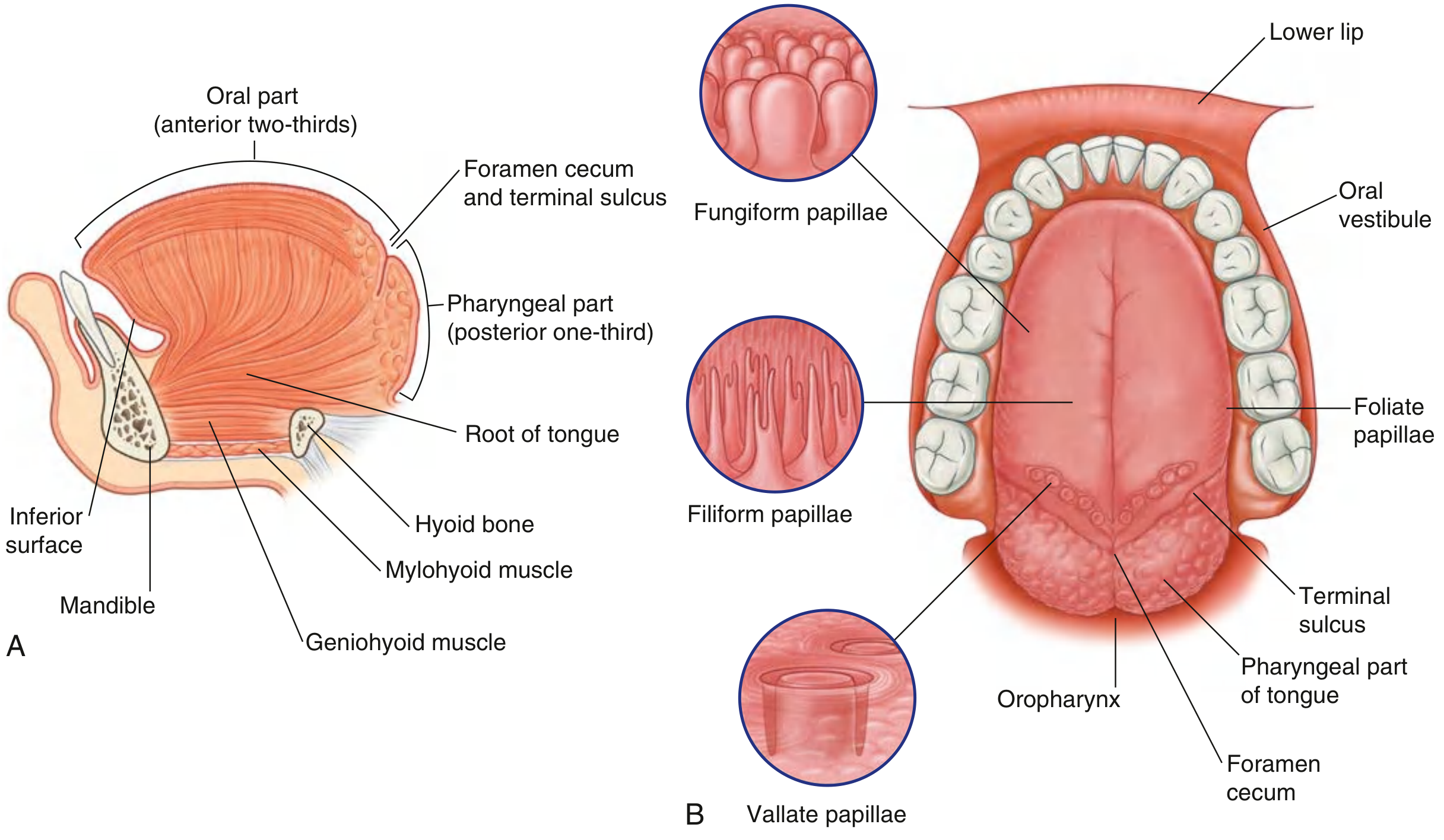
The tongue is divided into two parts by the terminal sulcus (a V-shaped groove):
| Part | Extent | Lies in |
|---|---|---|
| Oral part (anterior 2/3) | Tip → terminal sulcus | Oral cavity |
| Pharyngeal part (posterior 1/3) | Terminal sulcus → epiglottis | Oropharynx |
- At the apex of the terminal sulcus is the foramen cecum - the embryological origin of the thyroid gland (important for MCQs!)
- The root of the tongue is attached to the mandible and hyoid bone
- A median fibrous septum divides the tongue into right and left halves - all muscles are therefore paired
Papillae (on Dorsum of Oral Tongue)
| Papilla | Shape | Taste Buds? | Note |
|---|---|---|---|
| Filiform | Cone-shaped, pointed | ❌ No | Most numerous; give rough texture |
| Fungiform | Mushroom-shaped | ✅ Yes | On margins and tip |
| Vallate (Circumvallate) | Large, blunt cylinders in a moat | ✅ Yes | 8-12 in a V-row just in front of terminal sulcus |
| Foliate | Mucosal folds | ✅ Yes | On lateral sides near terminal sulcus |
Memory tip: "Filiform has False taste (no buds), all others have taste buds"
Muscles of the Tongue
All muscles supplied by CN XII (Hypoglossal) EXCEPT palatoglossus → CN X (Vagus)
Extrinsic Muscles (move the tongue as a whole)
| Muscle | Origin | Insertion | Action |
|---|---|---|---|
| Genioglossus | Superior mental spines of mandible | Hyoid + full length of tongue | Protrudes tongue (most important!) |
| Hyoglossus | Body + greater horn of hyoid | Lateral tongue | Depresses tongue |
| Styloglossus | Styloid process | Lateral tongue | Retracts + elevates tongue |
| Palatoglossus | Palatine aponeurosis | Lateral tongue | Elevates posterior tongue; closes oropharyngeal isthmus |
Exam point: Palatoglossus is supplied by vagus (CN X) - the only tongue muscle NOT supplied by CN XII
Intrinsic Muscles (change tongue shape - all CN XII)
| Muscle | Action |
|---|---|
| Superior longitudinal | Shortens tongue, curls tip upward |
| Inferior longitudinal | Shortens tongue, turns tip downward |
| Transverse | Narrows + elongates tongue |
| Vertical | Flattens + widens tongue |
Nerve Supply - The Most Important Topic for Exams!
The tongue has four different nerve supplies. Learn this table cold:
| Nerve | Region | Modality |
|---|---|---|
| Lingual nerve (CN V3) | Anterior 2/3 | General sensation (touch, pain, temperature) |
| Chorda tympani (CN VII) | Anterior 2/3 | Taste |
| Glossopharyngeal (CN IX) | Posterior 1/3 | Both general sensation AND taste |
| Vagus (CN X) | Near epiglottis (valleculae) | Taste only |
| Hypoglossal (CN XII) | All of tongue | Motor (muscles) |
Memory aid: "Very Fine Girls Vote Hard" = V3 (sensation ant 2/3), Facial/VII (taste ant 2/3), Glossopharyngeal/IX (post 1/3), Vagus/X (near epiglottis), Hypoglossal/XII (motor)
Blood Supply
Arterial: Lingual artery - a branch of the external carotid artery (loops deep to hyoglossus muscle to enter the tongue)
Venous: Lingual vein → internal jugular vein (the ranine vein on the undersurface is easily visible)
Hyoglossus as a landmark: The lingual artery passes deep to hyoglossus; the lingual nerve and hypoglossal nerve pass superficial to hyoglossus - this is a classic surgical anatomy question!
Lymphatic Drainage - KEY for Carcinoma
| Part of Tongue | Drains to | Side |
|---|---|---|
| Tip | Submental nodes → jugulo-omohyoid node | Bilateral |
| Central oral tongue | Submandibular nodes → deep cervical nodes | Bilateral |
| Lateral oral tongue | Submandibular nodes → deep cervical chain (Levels I-III) | Ipsilateral |
| Posterior 1/3 (base) | Direct to jugulodigastric (tonsillar) node | Bilateral |
Why this matters in carcinoma:
- Lateral border carcinoma - ipsilateral neck dissection is sufficient
- Tip or midline carcinoma - risk of bilateral nodal spread, so both sides of the neck must be assessed
- Base of tongue carcinoma - almost always bilateral nodal drainage, high rate of occult nodes
Clinical Correlations for MBBS Exams
| Condition | Anatomy Involved | Consequence |
|---|---|---|
| Hypoglossal nerve palsy | CN XII | Tongue deviates to the affected/paralysed side on protrusion (genioglossus of normal side pushes it over) |
| Carcinoma lateral tongue | Lateral border mucosa | Spreads to ipsilateral levels I-III; midline tumors spread bilaterally |
| Lingual thyroid | Foramen cecum | Failed descent of thyroid during embryogenesis |
| Tongue tie (ankyloglossia) | Short lingual frenulum | Difficulty protrusion + speech |
| Referred otalgia in tongue cancer | CN IX (posterior 1/3) → tympanic branch to middle ear | Ear pain with no ear disease |
| Taste loss after middle ear surgery | Chorda tympani damage | Loss of taste in anterior 2/3 of tongue |
Quick Revision Summary
TONGUE
├── Oral 2/3 (oral cavity) ──── Pharyngeal 1/3 (oropharynx)
├── Divided by terminal sulcus
├── Foramen cecum = thyroid origin
│
├── MUSCLES: All CN XII except Palatoglossus (CN X)
├── SENSATION: Ant 2/3 = V3 (lingual n.) | Post 1/3 = IX
├── TASTE: Ant 2/3 = VII (chorda tympani) | Post 1/3 = IX
├── MOTOR: All CN XII (except palatoglossus = CN X)
│
├── BLOOD: Lingual a. (branch of external carotid)
└── LYMPH: Lateral → ipsilateral; Tip/midline/base → bilateral
Sources: Gray's Anatomy for Students, Chapter 8; K.J. Lee's Essential Otolaryngology, Chapter 45
This is a shared conversation. Sign in to Orris to start your own chat.