Myocardial infarction pathology from robbins heading wise long answer for exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have all the content I need from the massive read of block6.md (lines 1077-1577). Let me now compile the comprehensive exam answer from all the rich content already retrieved. I have the full Robbins text covering:
- Epidemiology
- Pathogenesis/Etiology
- Types of MI (STEMI/NSTEMI, transmural/subendocardial)
- Gross and microscopic morphology with time sequence
- Clinical features and diagnosis
- Complications
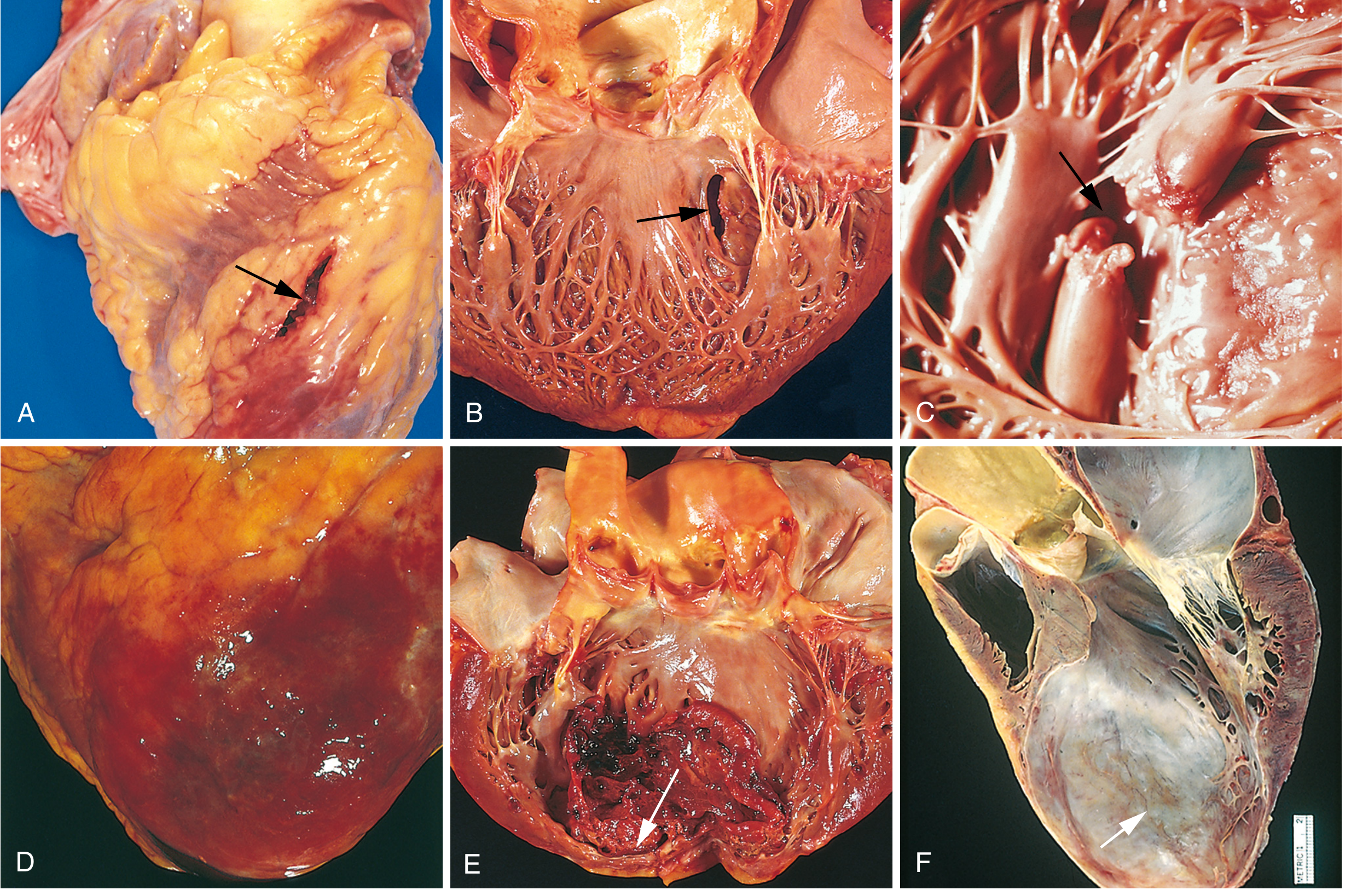
- The complications image
Let me now write the complete answer.
Myocardial Infarction - Robbins Pathology (Long Answer for Exam)
Source: Robbins, Cotran & Kumar - Pathologic Basis of Disease
1. DEFINITION
Myocardial infarction (MI), commonly called a "heart attack," is the death of cardiac muscle due to prolonged ischemia. It represents the most serious manifestation of ischemic heart disease (IHD).
- ~800,000 MIs per year in the United States (nearly one every 40 seconds)
- Causes ~400,000 deaths annually
- 10% occur in people under 40 years; 45% in people under 65 years
2. ETIOLOGY AND PATHOGENESIS
2.1 Coronary Artery Disease (Main Cause - >90% of cases)
The underlying cause is atherosclerosis of epicardial coronary arteries. There is usually a long, silent phase of coronary lesion progression over decades before acute events.
2.2 Sequence of Events Leading to MI
The dominant pathogenic mechanism involves disruption of an atherosclerotic plaque triggering acute thrombosis:
Step 1 - Atherosclerotic plaque formation: Lipid-rich plaques (with a large necrotic core and thin fibrous cap) develop in epicardial coronary arteries over years.
Step 2 - Plaque disruption: Either:
- Plaque rupture - Physical disruption of the thin fibrous cap, exposing the thrombogenic lipid core (most common, accounts for ~75%)
- Plaque erosion - Superficial denudation of endothelium without actual rupture (accounts for ~25%, more common in women, diabetics, smokers)
Step 3 - Thrombosis: Exposed subendothelial collagen and lipid core components trigger platelet aggregation and activation of the coagulation cascade, leading to thrombus formation.
Step 4 - Vessel occlusion: Complete thrombotic occlusion leads to transmural (full-thickness) ischemia. Partial occlusion causes subendocardial ischemia.
Step 5 - Ischemic injury:
- Reversible injury begins within 20-30 seconds (glycogen depletion, ultrastructural changes)
- Irreversible cell death begins after 20-40 minutes of sustained ischemia
- Necrosis progresses from subendocardium to epicardium - the "wavefront" phenomenon
2.3 Other Precipitating Causes
- Coronary artery vasospasm (Prinzmetal angina)
- Coronary artery emboli (infective endocarditis, mural thrombi)
- Coronary arteritis (Kawasaki disease, polyarteritis nodosa)
- Conditions increasing demand: tachycardia, hypertrophy, systemic hypotension, hypoxemia
3. TYPES OF MYOCARDIAL INFARCTION
3.1 Based on Extent of Wall Involvement
| Type | Extent | Cause |
|---|---|---|
| Transmural MI | Full thickness of ventricular wall | Complete coronary occlusion; associated with STEMI |
| Subendocardial MI | Inner 1/3 to 1/2 of myocardium | Partial/transient occlusion or global hypoperfusion; associated with NSTEMI |
The subendocardium is most vulnerable because:
- It is farthest from the epicardial vessels (longest diffusion distance)
- Intramyocardial pressure is highest there, further compressing vessels
3.2 Based on ECG Pattern
- STEMI (ST-Elevation MI): Usually from complete thrombotic occlusion → transmural infarct
- NSTEMI (Non-ST-Elevation MI): Partial occlusion or spontaneous thrombolysis → subendocardial infarct
3.3 Based on Location (Vessel Involved)
| Artery Occluded | Territory Infarcted |
|---|---|
| Left anterior descending (LAD) | Anterior LV wall, anterior septum, apex (most common - ~40-50%) |
| Right coronary artery (RCA) | Posterior LV wall, posterior septum, RV (posterior MI) |
| Left circumflex (LCx) | Lateral LV wall |
4. MORPHOLOGY (GROSS AND MICROSCOPIC)
4.1 Time-Sequence of Morphologic Changes
This is the most important and most commonly tested section.
A. Gross Changes
| Time After MI | Gross Appearance |
|---|---|
| 0-12 hours | Nothing visible on gross examination (early infarcts are grossly inapparent) |
| 12-24 hours | Pallor (pale, yellow-tan area); can be highlighted by tetrazolium (TTC) staining - normal myocardium turns brick-red; infarcted area remains pale/white |
| 1-3 days | Hyperemia at borders; central yellow-tan necrotic area; mottled appearance |
| 3-7 days | Maximally yellow-tan and soft (liquefactive-like); soft, pale yellow with red-tan rim of hyperemia (most vulnerable period for cardiac rupture) |
| 1-2 weeks | Hyperemic border with gray-white scar formation beginning from periphery; gelatinous appearance |
| 2-8 weeks | Gray-white, firm fibrous scar forming progressively |
| >2 months | Dense white fibrous scar (complete replacement fibrosis) |
B. Microscopic Changes
| Time | Microscopic Findings |
|---|---|
| 0-30 min | Reversible injury - glycogen depletion, mitochondrial swelling, minimal changes visible on H&E |
| 30 min - 4 hours | Vacuolar degeneration; earliest irreversible changes on electron microscopy (mitochondrial amorphous densities, sarcolemmal disruption) |
| 4-12 hours | "Wavy fibers" at infarct margins (from passive stretching of non-contracting dead fibers by adjacent viable myocardium). Coagulation necrosis begins - nuclei become pyknotic, cytoplasm becomes deeply eosinophilic |
| 12-24 hours | Coagulation necrosis well established - loss of nuclei, "ghost cells" with preserved but non-viable cytoplasmic outlines. Early neutrophil infiltration at margins |
| 1-3 days | Prominent neutrophilic infiltration throughout the infarcted area; cytoplasmic cross-striations lost; "mummified" myocytes |
| 3-7 days | Macrophage infiltration begins; neutrophils dying; phagocytosis of necrotic debris begins. Myocyte ghost outlines being removed. This is the weakest period |
| 7-10 days | Prominent macrophages phagocytosing debris; beginning of granulation tissue from edges - proliferating fibroblasts and new capillaries |
| 10-14 days | Granulation tissue (fibroblasts + new vessels) actively replacing dead myocardium; progressively from periphery toward center |
| 2-8 weeks | Progressive collagen deposition; decreasing cellularity; scar maturing |
| >8 weeks | Dense collagenous scar (mature fibrous scar); hyalinized collagen; no residual inflammation |
Key exam mnemonic for microscopy:
- 4-12 h: Wavy fibers + coagulation necrosis begins
- 1-3 days: Neutrophils peak
- 3-7 days: Macrophages replace neutrophils - WEAKEST POINT (rupture risk)
- 1-2 weeks: Granulation tissue
- >2 months: Fibrous scar
4.2 Special Features
Contraction band necrosis (reperfusion injury):
- Seen in reperfused myocardium (after thrombolysis, PCI)
- Hypercontracted sarcomeres form dark transverse bands across myocytes
- Results from massive calcium influx into cells at time of reperfusion
- Indicates reperfusion but also marks irreversibly injured cells
5. CLINICAL FEATURES AND DIAGNOSIS
5.1 Symptoms
- Severe, crushing chest pain (most common) - often radiating to left arm, jaw, neck
- Nausea, vomiting, diaphoresis
- Dyspnea
- ~10-15% of MIs are "silent" (painless), especially in diabetics and elderly
5.2 ECG Changes
- STEMI: ST-segment elevation in leads over infarcted territory; Q waves develop later
- NSTEMI: ST depression or T-wave inversion; no Q waves
5.3 Serum Cardiac Biomarkers (Diagnosis Hallmark)
| Marker | Rises | Peaks | Normalizes | Notes |
|---|---|---|---|---|
| Troponin I / T | 2-4 hours | 24-48 hours | 7-14 days | Most sensitive and specific; gold standard |
| CK-MB | 4-8 hours | 15-20 hours | 2-3 days | Useful for reinfarction detection |
| Myoglobin | 1-3 hours | 6-8 hours | 24-36 hours | Earliest marker but not cardiac-specific |
| LDH | 24-48 hours | 3-6 days | 8-14 days | Older marker, rarely used now |
Troponin I/T are the most sensitive and specific markers; small elevations are clinically significant.
6. CONSEQUENCES AND COMPLICATIONS OF MI
Nearly three-quarters of patients experience one or more complications after acute MI. Overall in-hospital mortality is <7%.
6.1 Arrhythmias
- The most common complication and the most common cause of death (especially out of hospital)
- Occur in 75-95% of MI patients
- Ventricular fibrillation (VF) - most common cause of sudden death within first hour
- Ventricular tachycardia (VT), AV block (especially with inferior MI affecting AV nodal artery), bradyarrhythmias
- Cause: Ischemia-induced electrical instability in border zone between infarcted and viable tissue
6.2 Contractile Dysfunction (Pump Failure)
- LV pump failure proportional to volume of damaged myocardium
- Manifests as: hypotension, pulmonary congestion, pulmonary edema
- Cardiogenic shock: occurs in ~10% of transmural MIs; associated with >40% LV damage; carries very high mortality
6.3 Papillary Muscle Dysfunction/Rupture
- Posteromedial papillary muscle more commonly affected (single blood supply from RCA)
- Ischemic dysfunction leads to mitral regurgitation
- Complete rupture (occurs 2-7 days post-MI) = acute severe mitral regurgitation = hemodynamic emergency
6.4 Cardiac Rupture (Days 3-7 - Peak Risk)
The 3-7 day window is when neutrophils have degraded necrotic tissue and fibrous scar has not yet formed.
Three types:
- Free wall rupture (most common type of rupture): Rupture of LV free wall → hemopericardium → cardiac tamponade → rapidly fatal. Most common in elderly, hypertensive women, first MI, without prior angina (no preconditioning)
- Ventricular septal rupture (VSD): Creates acute left-to-right shunt → sudden biventricular failure; needs urgent surgery
- Papillary muscle rupture: Acute severe mitral regurgitation → pulmonary edema/cardiogenic shock
6.5 Right Ventricular Infarction
- Occurs in 1-3% of isolated cases; more commonly associated with inferior/posterior LV MI from RCA occlusion
- Results in right-sided heart failure, venous pooling, systemic hypotension
- Classic triad: hypotension + JVD + clear lungs (no pulmonary edema)
6.6 Infarct Expansion (Early Remodeling)
- Acute dilatation and thinning of the infarcted region without additional necrosis
- Most common with anterior transmural MIs
- Promotes formation of mural thrombus
- Contributes to LV remodeling and aneurysm formation
6.7 Mural Thrombus
- Overlying the endocardium in infarcted zone - rough, necrotic endocardium + stasis in dyskinetic area promotes thrombus
- Risk of systemic embolism (stroke, mesenteric ischemia, limb ischemia)
- Treatment: anticoagulation
6.8 Ventricular Aneurysm (Late Complication)
- True aneurysm: Thinned, dyskinetic fibrous wall bulging outward during systole; lined by organized mural thrombus
- Most common after large anterior MI
- Complications: heart failure, arrhythmias, thrombus with embolism
- Unlike pseudoaneurysm (contained rupture with pericardial adhesion) - pseudoaneurysm has higher rupture risk
6.9 Pericarditis
- Fibrinous pericarditis: Occurs 1-3 days post-MI, overlying transmural infarct; "bread-and-butter" appearance; causes pericardial friction rub; self-limited
- Dressler Syndrome (Post-MI Syndrome): Delayed fibrinous pericarditis 2-10 weeks post-MI; autoimmune-mediated (antibodies against cardiac antigens released from necrotic myocardium); presents with fever, pleuritis, pericarditis
6.10 Progressive Late Heart Failure (Post-MI Remodeling)
- Long-term ventricular remodeling with hypertrophy of residual myocardium and progressive dilation
- Leads to ischemic cardiomyopathy / chronic IHD with heart failure
7. PROGNOSIS AND OUTCOMES
- In-hospital mortality for MI: <7% overall (STEMI ~9%, NSTEMI ~6%)
- Out-of-hospital STEMI mortality: ~33% (usually VF within 1 hour before treatment)
- Prognosis depends on: infarct size, location, residual LV function, arrhythmia complications
8. SUMMARY TABLE: KEY FACTS AT A GLANCE
| Feature | Details |
|---|---|
| Most common cause | Atherosclerotic plaque rupture + thrombosis (>90%) |
| Most common artery | LAD (anterior MI, most common overall) |
| Most vulnerable layer | Subendocardium (first to die) |
| Earliest gross change | Pallor at 12-24 hrs; TTC stain shows pale zone |
| Earliest microscopic change | Wavy fibers (4-12 hrs) |
| Most diagnostic marker | Troponin I/T (rises at 2-4 hrs, peaks 24-48 hrs) |
| Peak rupture time | 3-7 days (when neutrophils have lysed tissue) |
| Most common complication | Arrhythmias |
| Most common cause of immediate death | Ventricular fibrillation |
| Cardiogenic shock threshold | >40% LV destruction |
| Completed scar formation | By 6-8 weeks |
Robbins, Cotran & Kumar - Pathologic Basis of Disease (10th ed.), Chapter 12: Heart, pp. 492-520
This is a shared conversation. Sign in to Orris to start your own chat.