Myopia
Reading File
Finding Sources
Searching PubMed
myopia pathogenesis management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of myopia drawn from multiple medical textbooks.
Myopia (Nearsightedness)
Definition & Optics
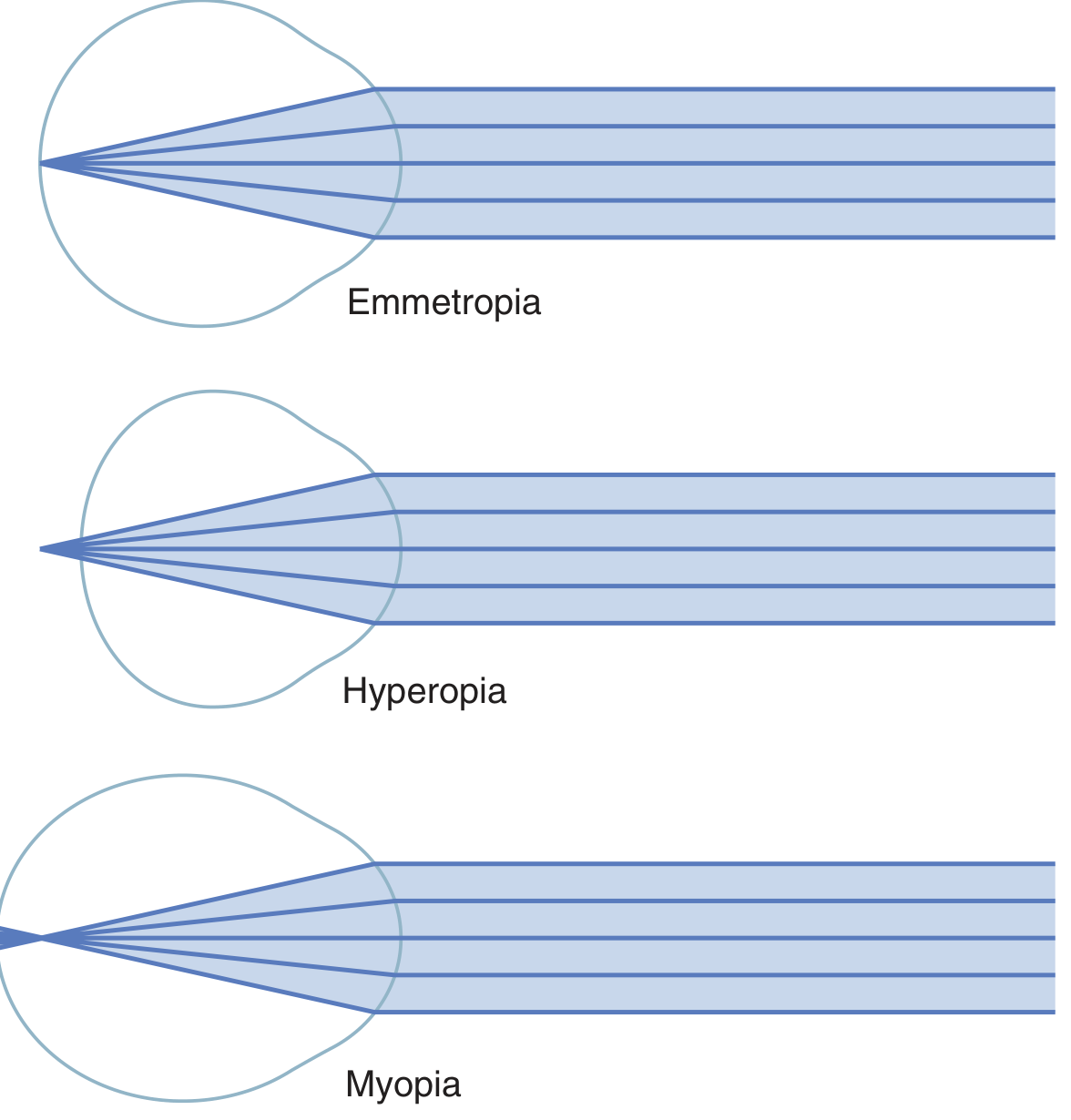
Myopia is a refractive error in which parallel light rays from distant objects converge to a focal point in front of the retina (rather than on it), resulting in blurred distance vision with relatively preserved near vision. It most commonly results from an excessively long axial length of the eyeball, but can also be caused by excessive refractive power in the lens system.
Classification
| Type | Definition |
|---|---|
| Low myopia | < −3 D |
| Moderate myopia | −3 D to −6 D |
| High myopia | > −6 D (axial length usually > 26 mm) |
| Pathologic/Degenerative myopia | Progressive axial elongation with secondary ocular structural changes |
High myopia (WHO defines it as > −5.00 D) affects >2% of Western/American adults and up to 10% of East Asians. Global prevalence is expected to reach 5 billion by 2050, with 1 billion having high myopia.
Aetiology & Risk Factors
Myopia arises from complex hereditary and environmental factors:
- Strong association with prolonged near visual work (reading, screen use)
- Reduced outdoor time — sunlight exposure appears protective
- Genetics — multiple loci identified; family history is a major risk factor
Systemic associations of high myopia (Table 14.4, Kanski's):
- Down syndrome
- Stickler syndrome
- Marfan syndrome
- Prematurity
- Noonan syndrome
- Ehlers–Danlos syndrome
- Pierre–Robin syndrome
Pathology of Degenerative (Pathologic) Myopia
Pathologic myopia involves progressive weakening and elongation of the posterior sclera, mechanically stretching all posterior ocular tissues. Key fundus findings include:
| Finding | Description |
|---|---|
| Tessellated (tigroid) fundus | Diffuse RPE attenuation → large choroidal vessels visible |
| Focal chorioretinal atrophy | Patchy RPE and choroidal loss |
| Tilted optic disc | Anomalous optic nerve head appearance |
| Peripapillary atrophy | Temporal crescent of thinned/absent RPE |
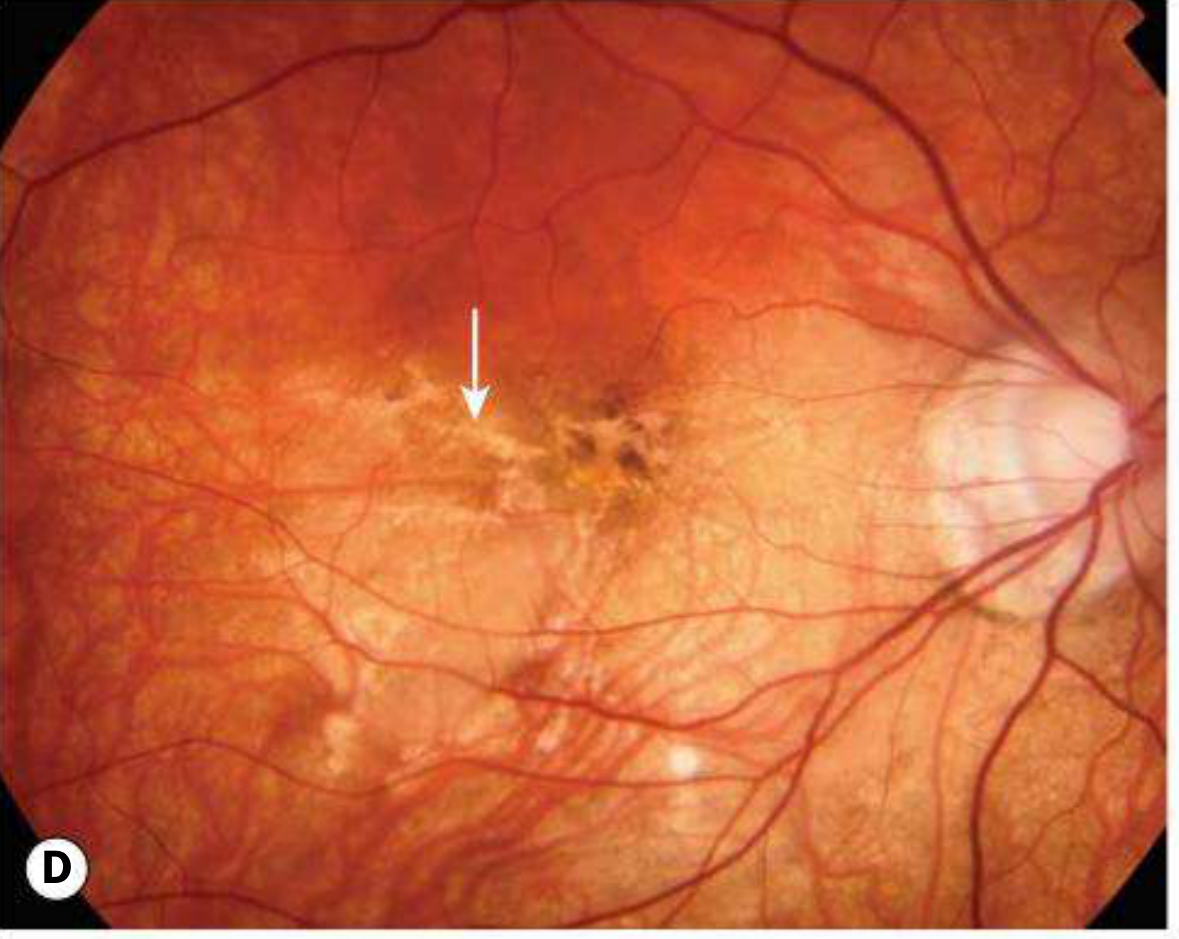
| Lacquer cracks | Ruptures in RPE–Bruch membrane complex (~5% of highly myopic eyes); fine yellow irregular lines at posterior pole |
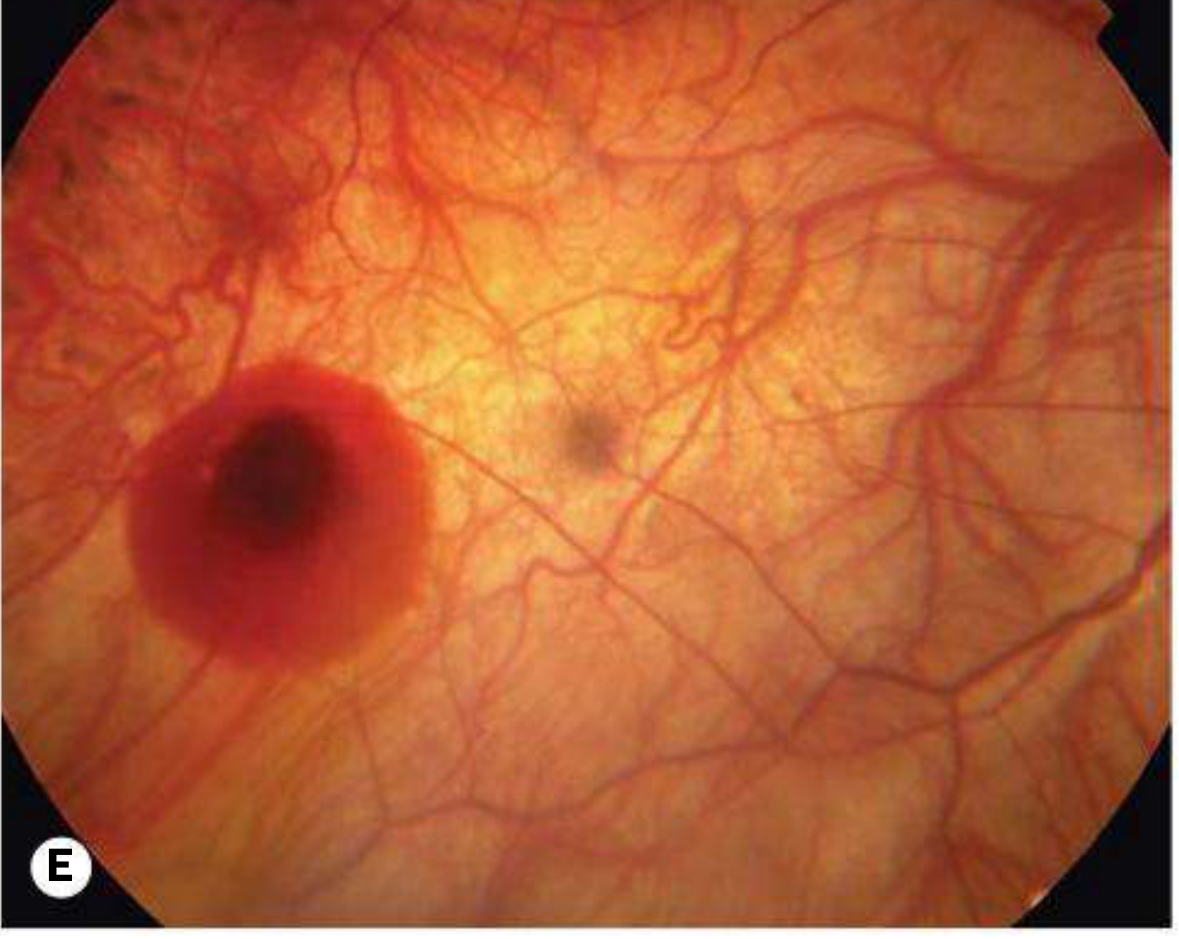
| Subretinal "coin" haemorrhage | From lacquer cracks without MNV |
| Fuchs spot | Raised pigmented macular lesion after subretinal haemorrhage absorbs |
| Posterior staphyloma | Focal peripapillary or macular scleral ectasia (~1/3 of pathologic myopia eyes) |
| Lattice degeneration | Peripheral retinal thinning |
| Macular neovascularization (MNV) | ~10% of highly myopic eyes; treated with anti-VEGF |
| Rhegmatogenous retinal detachment | Increased risk due to PVD, lattice degeneration, atrophic holes |
| Macular retinoschisis / foveoschisis | From vitreous traction in high myopia with staphyloma |
Maculopathy is the most common cause of visual loss in pathological myopia and a significant cause of legal blindness.
Correction of Myopia
Optical
- Spectacles with concave (diverging) lenses — diverge rays before they enter the eye, shifting the focal point posteriorly onto the retina
- Contact lenses — same optical principle
Surgical (from Kanski's Clinical Ophthalmology)
| Procedure | Notes |
|---|---|
| Surface ablation (PRK/LASEK) | Low–moderate myopia |
| LASIK | Moderate–high myopia; limited by initial corneal thickness |
| SMILE (refractive lenticule extraction) | Small-incision technique for myopia and myopic astigmatism |
| Iris clip implant ("lobster claw")** | Anterior chamber phakic IOL; complications include subluxation, endothelial cell loss, cataract, pupillary-block glaucoma, retinal detachment |
| Phakic posterior chamber implant (ICL) | Implanted behind iris, in front of lens; power −3 D to −20.5 D; material = Collamer (collagen-derived) |
| Clear lens exchange | Good visual results; risk of RD (higher in high myopia) |
| Radial keratotomy | Now predominantly historical |
Myopia Control (Slowing Progression in Children)
| Intervention | Evidence |
|---|---|
| Low-dose atropine 0.01% (bedtime) | Significantly slows myopia progression; reasonable to offer ages 5–15 if progressing > 1 D/year; mechanism unclear; side effects dose-dependent (mydriasis, loss of accommodation) |
| High-add (+2.50 D) multifocal contact lenses | For ages 7–11 with < 5 D myopia; BLINK trial shows dose-dependent slowing of progression |
| Increased outdoor time in sunshine | Protective; encouraged alongside pharmacological treatment |
High Myopia Complication: MNV Treatment
Anti-VEGF therapy is the treatment of choice for myopia-related MNV. Injection frequency is generally less than that needed for AMD, but retinal detachment risk is higher. Prognosis is better in younger patients compared to AMD-related MNV.
High Myopia & Lens Changes
High myopia can cause:
- Posterior subcapsular lens opacity
- Early-onset nuclear sclerosis — paradoxically may increase the myopic refractive error
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 299, 631–632
- Guyton & Hall Textbook of Medical Physiology, p. 625
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
- Goldman-Cecil Medicine
Fundus picture
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
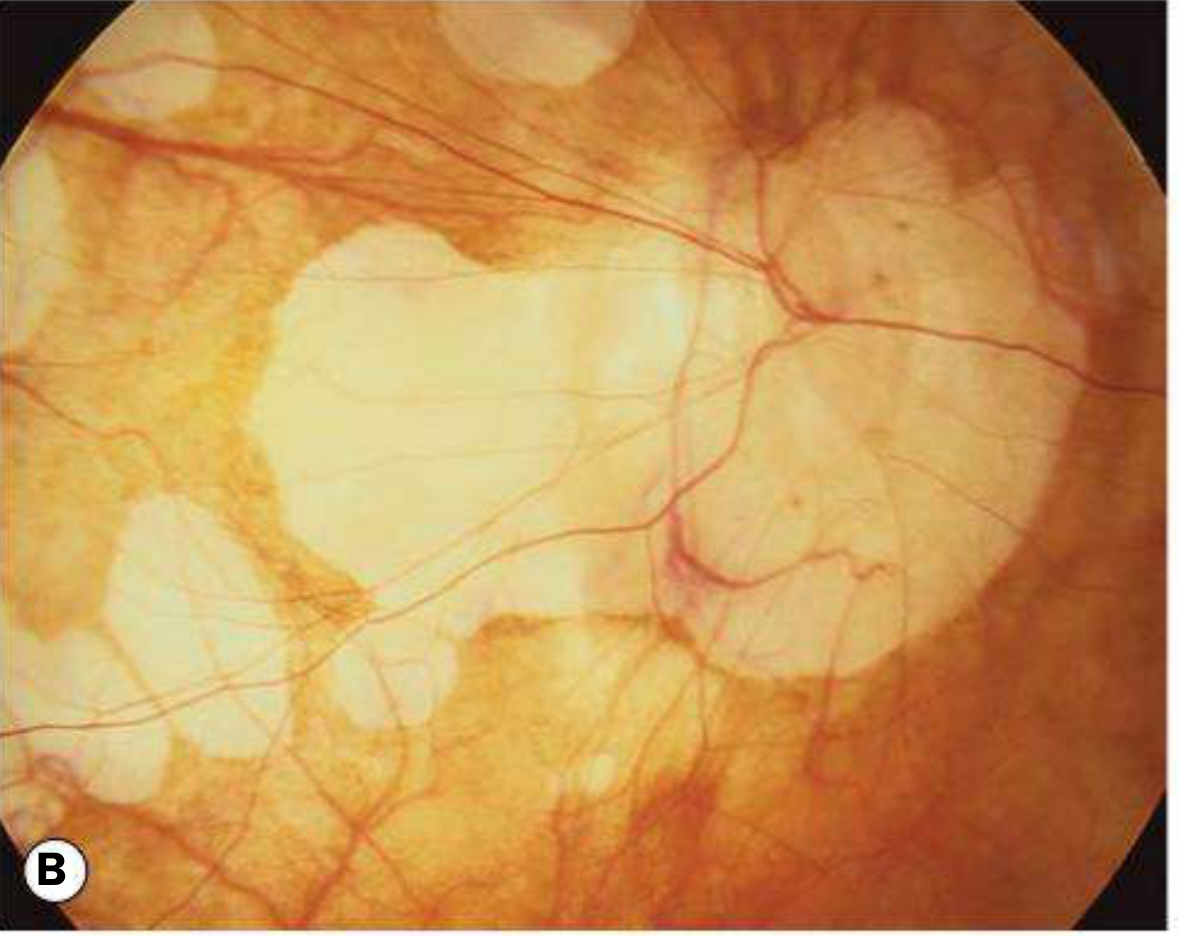
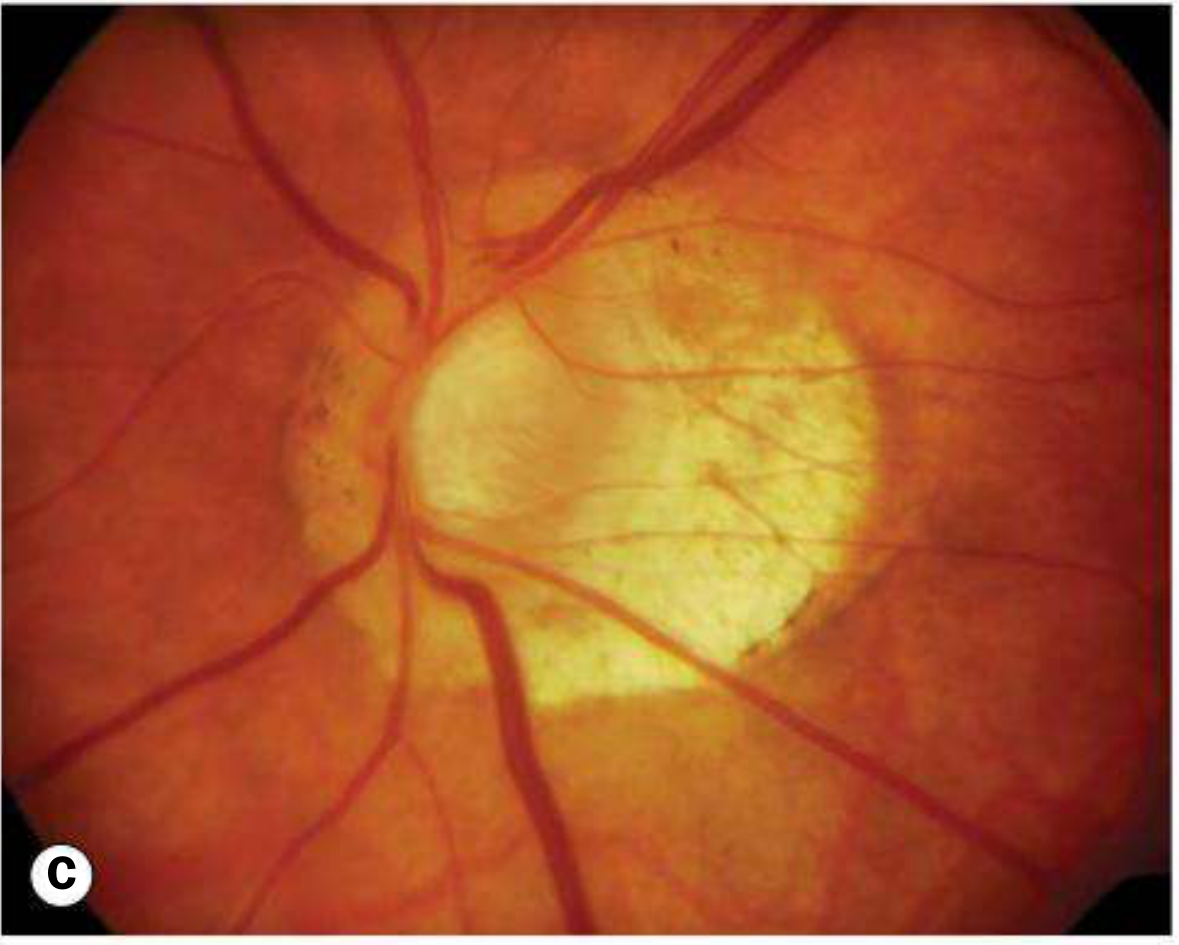
Here are the fundus photographs of high/pathologic myopia from Kanski's Clinical Ophthalmology (10th ed.):
A — Tessellated (Tigroid) Fundus
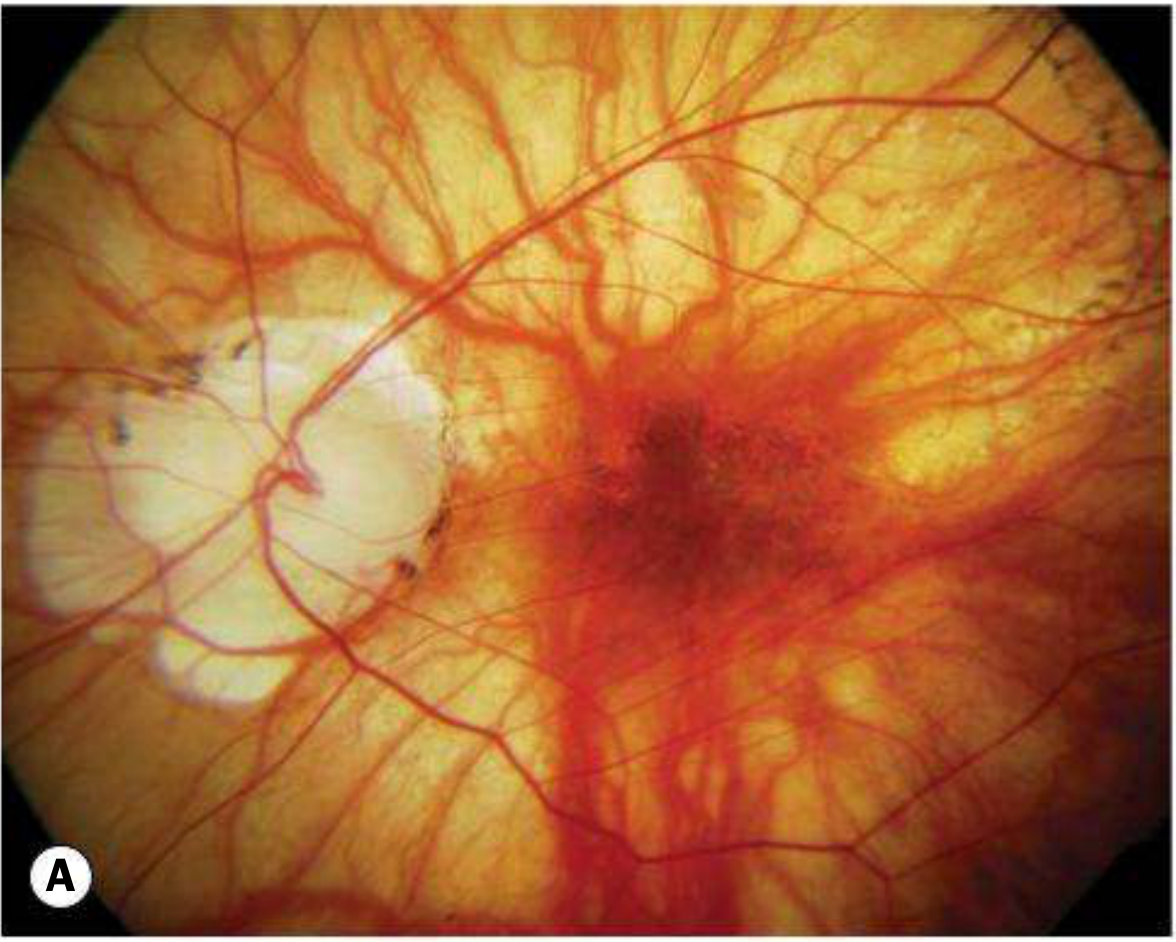
B — Focal Chorioretinal Atrophy & Tilted Disc
C — Tilted Disc with Peripapillary Atrophy
D — Lacquer Cracks (arrow)
E — Subretinal "Coin" Haemorrhage
F — Fuchs Spot
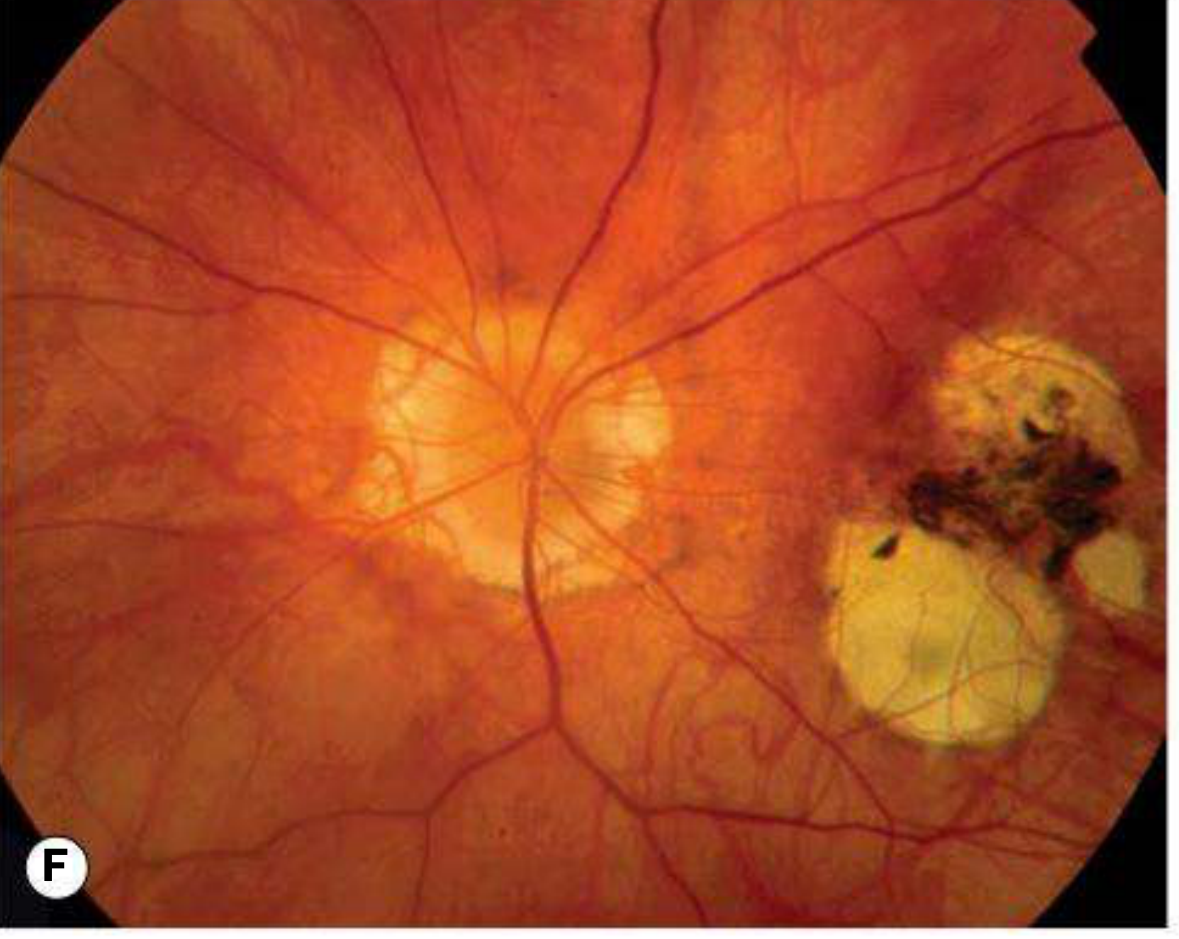
Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., Fig. 14.52
Diabetic retinopathy with fundus picture
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.