A cancer patient
Asking for Preferences
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information to compile a thorough answer on breast cancer diagnosis and staging. Here it is:
Breast Cancer: Diagnosis & Staging
Epidemiology
The lifetime risk of developing breast cancer is 1 in 8 for women living to age 90 in the United States. In 2023, approximately 297,790 women in the US were diagnosed with invasive breast cancer, with over 43,000 deaths - second only to lung cancer. Incidence rises rapidly after age 30 and peaks in older age, though triple-negative (TNBC) and HER2-positive cancers plateau around age 40 and are proportionally more common in younger women. - Robbins & Cotran Pathologic Basis of Disease, p. 971
Clinical Presentation & Examination
Most breast cancers present as a painless, palpable mass. Key clinical features that raise suspicion include:
- A firm, irregular, stellate-shaped mass (classic for invasive ductal carcinoma)
- Skin changes: peau d'orange (skin edema/dimpling), erythema, skin ulceration
- Nipple retraction or inversion
- Unilateral erythematous nipple eruption with scaling (Paget disease of the nipple - 1%-4% of breast cancers)
- Axillary lymphadenopathy
- Nipple discharge
Inflammatory Breast Carcinoma (IBC) is a special clinical entity - defined by skin changes (erythema, warmth, peau d'orange) involving at least one-third of the breast skin. It must be distinguished from mastitis or cellulitis; failure to improve with antibiotics should prompt biopsy. - Current Surgical Therapy 14e
Diagnostic Workup
1. Imaging
Mammography is the primary screening and diagnostic modality.
- Principal mammographic signs: densities, architectural distortions, and calcifications (none individually specific for malignancy)
- Average size of mammographically detected invasive carcinoma: ~1 cm (significantly smaller than palpation-detected cancers)
- Sensitivity and specificity increase with age: at 40 years, probability a lesion is cancer is ~10%; rises to >25% after age 50
- ~10% of invasive carcinomas are not visible on standard 2D mammography
- Screening mammography in women ≥50 years reduces breast cancer mortality by approximately 25%
Adjunct imaging modalities:
- Digital breast tomosynthesis - improves detection over standard 2D mammography
- Ultrasonography - differentiates cysts from solid masses; guides biopsy
- MRI - very high sensitivity for invasive breast cancer; uses lesion morphology and gadolinium enhancement kinetics; recommended for local staging of primary breast cancer, treatment monitoring, and screening in women with BRCA mutations or >20%-25% lifetime risk
- Schwartz's Principles of Surgery, 11e; Robbins & Cotran; Grainger & Allison's Diagnostic Radiology
2. Biopsy
Core-needle biopsy (CNB) is the preferred method for both palpable and nonpalpable breast abnormalities. It is preferred over fine-needle aspiration (FNA) because it provides histological architecture rather than cytology alone, allowing receptor testing. - Schwartz's Principles of Surgery, 11e
3. Biomarker Assessment
Once a diagnosis is made, the following should be established before initiating therapy:
- ER (Estrogen Receptor) status
- PR (Progesterone Receptor) status
- HER2 amplification/overexpression
- Tumor grade (I-III based on nuclear grade, mitotic rate, tubule formation)
These biomarkers define the clinical subtypes:
| Subtype | ER | PR | HER2 | Characteristics |
|---|---|---|---|---|
| Luminal A | + | +/- | - | Low proliferation; best prognosis |
| Luminal B | + | +/- | -/+ | Higher proliferation |
| HER2-enriched | - | - | + | More aggressive; targeted therapy available |
| Triple Negative (TNBC) | - | - | - | Most aggressive; no targeted hormonal/HER2 therapy |
- Robbins & Cotran Pathologic Basis of Disease, p. 971
Histopathology
In Situ Carcinomas
Ductal Carcinoma In Situ (DCIS)
- Neoplastic proliferation limited within ducts/lobules by the basement membrane; myoepithelial cells preserved
- Almost always detected by mammography (calcifications or periductal fibrosis)
- Classified by nuclear grade: low-grade DCIS is typically ER+/HER2-; high-grade DCIS may be ER-/HER2+
- Growth patterns: comedo (with central necrosis), cribriform, micropapillary, papillary
- No longer classified as Tis (LCIS is now considered a benign risk marker, not a true carcinoma)
Paget Disease of the Nipple
- DCIS extending through ducts to nipple skin; classified as Tis (Paget)
- Presents as unilateral erythematous, scaly eruption; may be mistaken for eczema
Invasive Carcinomas
Based on SEER data (135,157 women), histologic subtypes and their frequency:
| Subtype | Frequency |
|---|---|
| Invasive Ductal Carcinoma (IDC) | ~76% |
| Invasive Lobular | ~8% |
| Ductal/Lobular mixed | ~7% |
| Mucinous/Colloid | ~2.4% |
| Tubular | ~1.5% |
| Medullary | ~1.2% |
| Papillary | ~1% |
IDC typically presents as a firm, gray-white, gritty mass with characteristic irregular stellate shape on imaging due to fibrous stromal reaction. - Mulholland & Greenfield's Surgery, 7e
Staging: AJCC TNM System (8th Edition)
The 8th edition AJCC system adds pathologic prognostic factors (receptor status, tumor grade, gene expression) beyond pure anatomic staging. The anatomic TNM framework is as follows:
T - Primary Tumor
| Stage | Criteria |
|---|---|
| Tis | Carcinoma in situ (DCIS) or Paget disease with no tumor |
| T1 | Invasive tumor ≤20 mm |
| T2 | >20 mm but ≤50 mm |
| T3 | >50 mm |
| T4 | Any size with chest wall extension, skin edema/ulceration, satellite nodules, or inflammatory carcinoma (T4d) |
N - Regional Lymph Nodes
Clinical (cN):
- cN0: No regional lymph node metastases
- cN1: Mobile ipsilateral level I/II axillary nodes
- cN2: Fixed/matted axillary nodes or ipsilateral internal mammary (IM) nodes
- cN3: Infraclavicular, combined IM + axillary, or supraclavicular involvement
Pathologic (pN) - preferred when available:
- pN0: No regional metastases
- pN1mi: Micrometastases (>0.2 mm or >200 cells, but none >2.0 mm)
- pN1: 1-3 axillary nodes and/or IM nodes (SLN detected, not clinically apparent)
- pN2: 4-9 axillary nodes or clinically detected IM nodes without axillary involvement
- pN3: ≥10 axillary nodes, infraclavicular (level III), supraclavicular, or combined IM + axillary involvement
Important: Metastases must be >0.2 mm and exceed 200 cells to be clinically relevant. Circulating tumor cells in blood/bone marrow <0.2 mm are designated cM0(i+).
M - Distant Metastasis
- M0: No distant metastasis
- M1: Detectable distant metastases (clinically, radiographically, or histologically proven, >0.2 mm)
- Metastasis to contralateral axilla or cervical nodes = M1 (distant disease)
Stage Grouping
| Stage | T | N | M |
|---|---|---|---|
| 0 | Tis | N0 | M0 |
| I | T1 | N0 | M0 |
| IIA | T0-1/N1 or T2/N0 | - | M0 |
| IIB | T2/N1 or T3/N0 | - | M0 |
| IIIA | T0-3/N2 or T3/N1 | - | M0 |
| IIIB | T4/N0-2 | - | M0 |
| IIIC | Any T/N3 | - | M0 |
| IV | Any T | Any N | M1 |
- Mulholland & Greenfield's Surgery, 7e, p. 3930-31; Schwartz's Principles of Surgery, 11e
Precursor Lesion Risk Stratification
Understanding benign breast lesions and their cancer risk is part of diagnosis:
| Pathologic Lesion | Relative Risk | Absolute Lifetime Risk |
|---|---|---|
| Nonproliferative changes (cysts, adenosis, duct ectasia) | 1.0 | ~3% |
| Proliferative without atypia (usual ductal hyperplasia, sclerosing adenosis) | 1.5-2x | ~5%-7% |
| Proliferative with atypia (ADH, ALH) | 4-5x | ~13%-17% |
| Carcinoma in situ (LCIS, DCIS) | 8-10x | ~25%-30% |
- Robbins & Cotran Pathologic Basis of Disease, Table 23.1
Key Staging Principles
- The TNM staging system estimates predicted survival but should not be used alone to dictate treatment
- Sentinel lymph node (SLN) biopsy is the preferred method for axillary staging in clinically node-negative patients
- Axillary dissection can be avoided in patients with 1-2 positive SLNs who are treated with breast-conserving surgery + whole breast radiation + systemic therapy
- Treatment decisions are best made via a multidisciplinary approach, incorporating tumor biology (receptor status, grade) alongside anatomic stage
- MRI screening is recommended for BRCA mutation carriers and women with >20%-25% lifetime risk
With diagrams
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Here is the full illustrated guide to Breast Cancer: Diagnosis & Staging, with diagrams from authoritative surgical and pathology textbooks.
Breast Cancer: Diagnosis & Staging — Illustrated
1. Breast Cancer Classification Overview
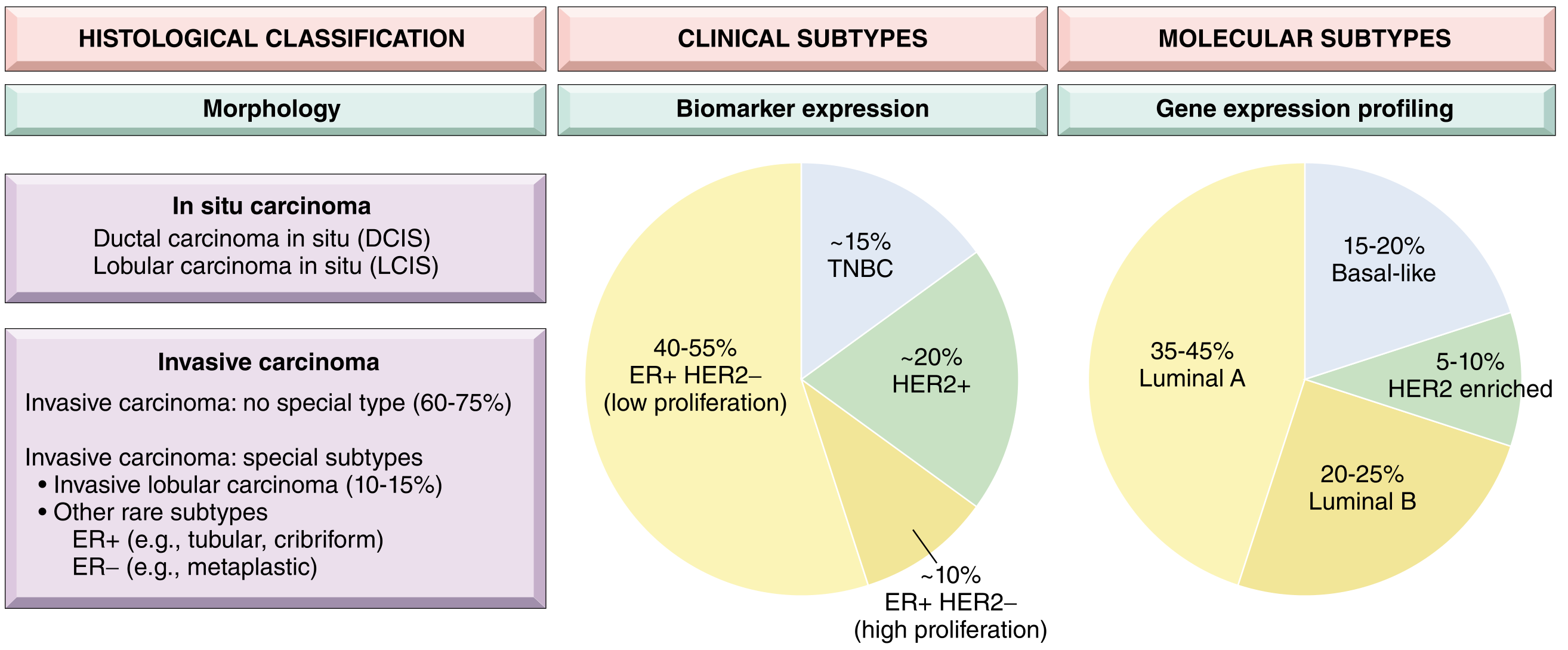
Fig. 1 - Breast cancer is classified three ways: by histological morphology (in situ vs invasive), by biomarker expression (ER, PR, HER2 status), and by gene expression profiling into molecular subtypes. Luminal A (ER+/HER2-, low proliferation) is the most common at 35-45%. - Robbins & Cotran Pathologic Basis of Disease
2. Mammography: Normal vs. Malignant Features
Normal mammogram (bilateral mediolateral oblique and craniocaudal views):
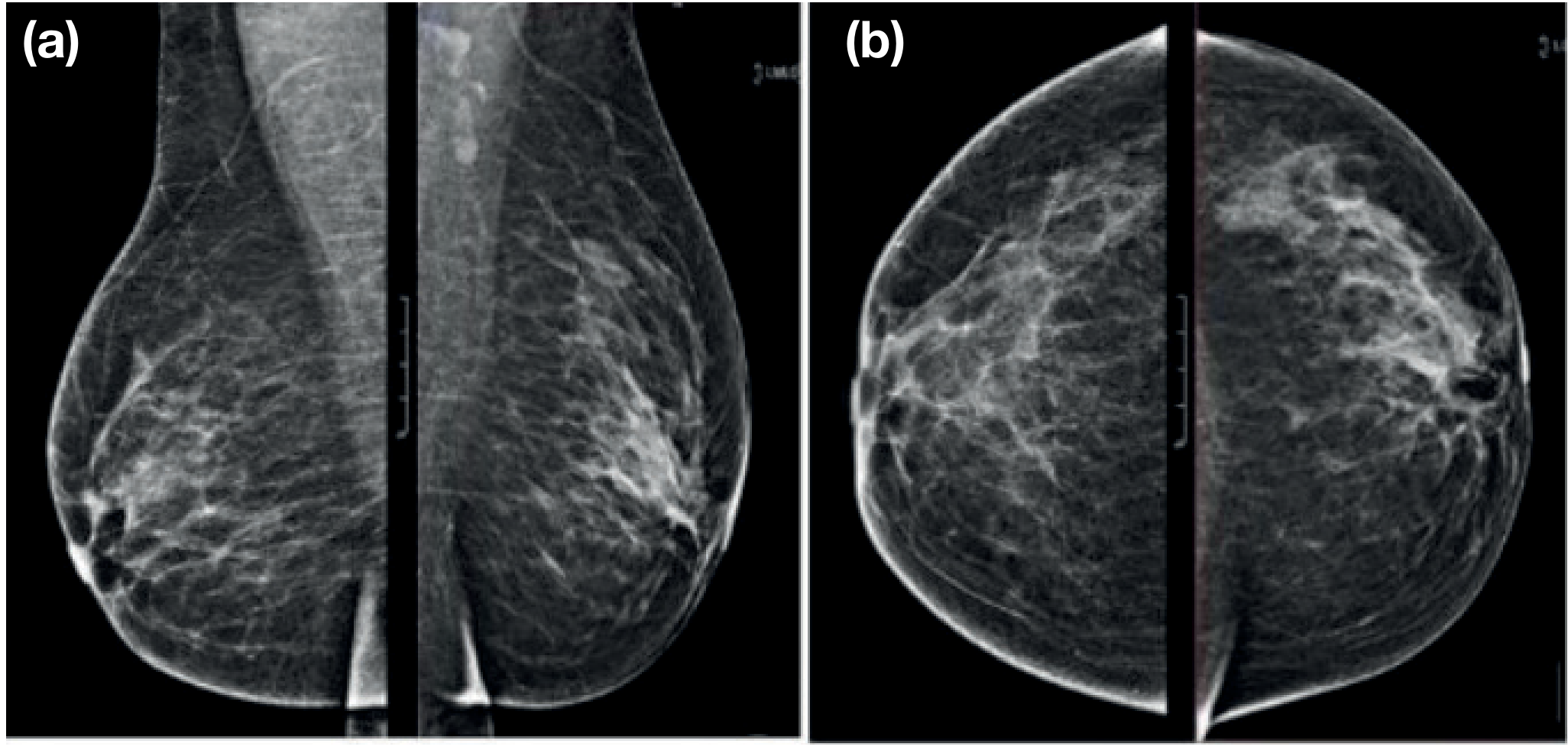
Fig. 2 - Normal mammogram (Bailey & Love, 28th ed.): (a) mediolateral oblique view; (b) craniocaudal view. Normal breast tissue shows a fine trabecular pattern without masses or calcifications.
Malignant mammographic features (BI-RADS Category 5):
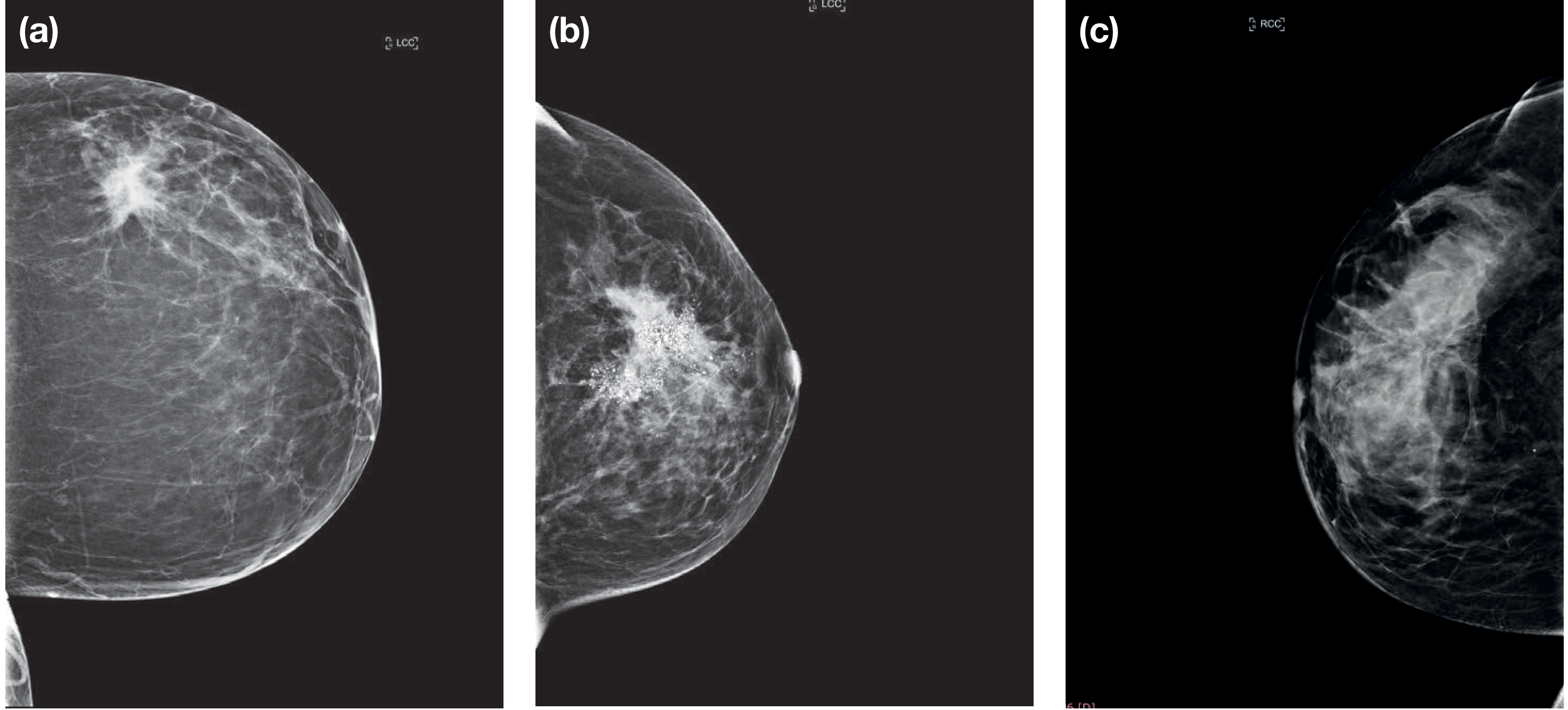
Fig. 3 - Imaging features of breast cancer on mammography - Bailey & Love's Surgery, 28th ed.:
- (a) Irregular, spiculated mass (stellate shape from fibrous stromal reaction - classic for invasive ductal carcinoma)
- (b) Fine pleomorphic microcalcifications (typical of DCIS)
- (c) Architectural distortion (normal trabecular pattern disrupted without a visible mass)
3. MRI of Breast Cancer
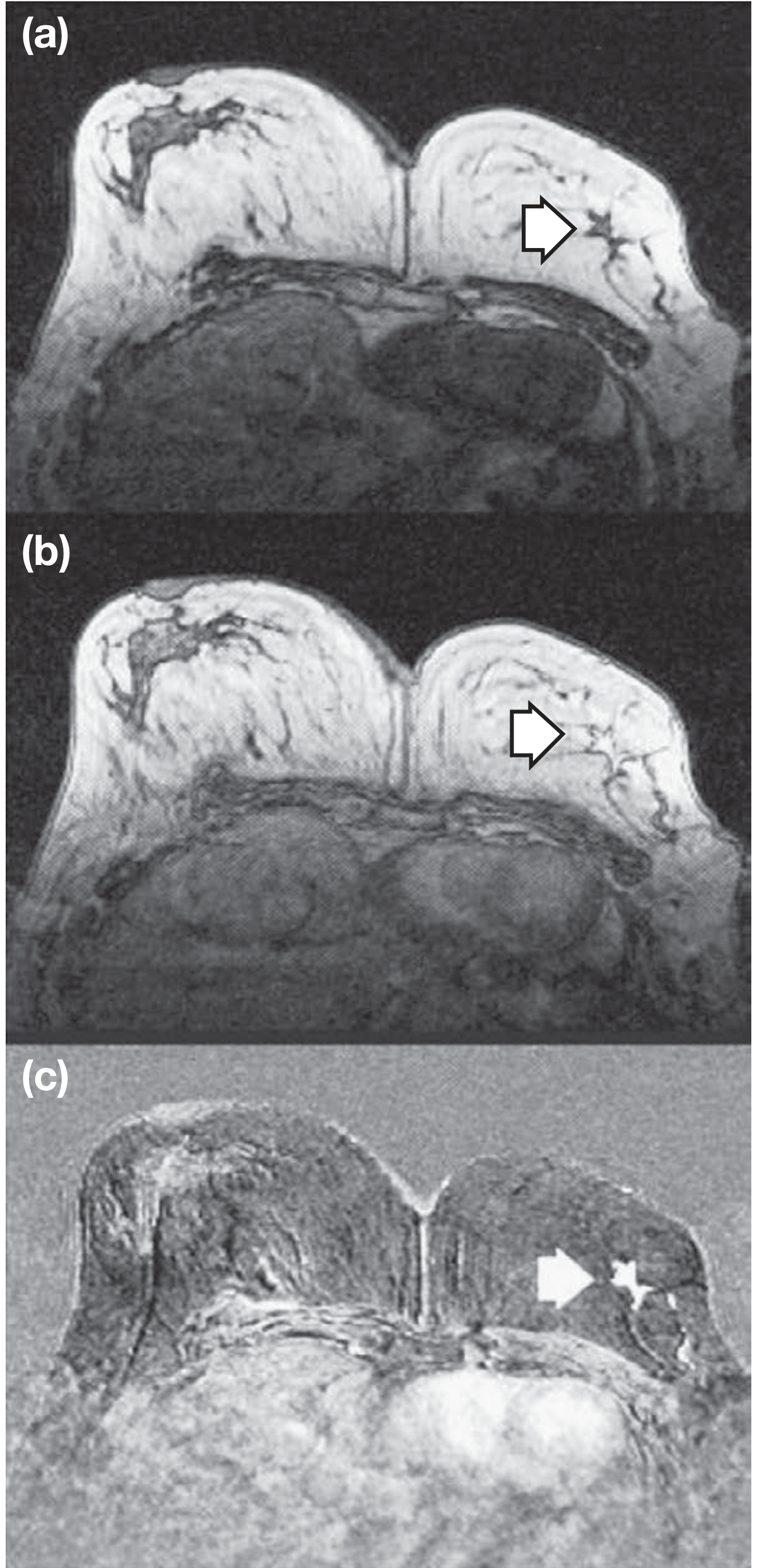
Fig. 4 - MRI showing carcinoma of the left breast (arrows) - Bailey & Love's Surgery, 28th ed.:
- (a) Pre-contrast: lesion is isointense, not visible
- (b) Post-gadolinium: lesion enhances (irregular, suspicious kinetics)
- (c) Subtraction image: confirms true enhancement pattern
MRI is the most sensitive modality for invasive breast cancer and is used for local staging, assessing multifocality, monitoring neoadjuvant therapy, and screening BRCA mutation carriers.
4. Apocrine Cysts (Histology) - Benign Differential
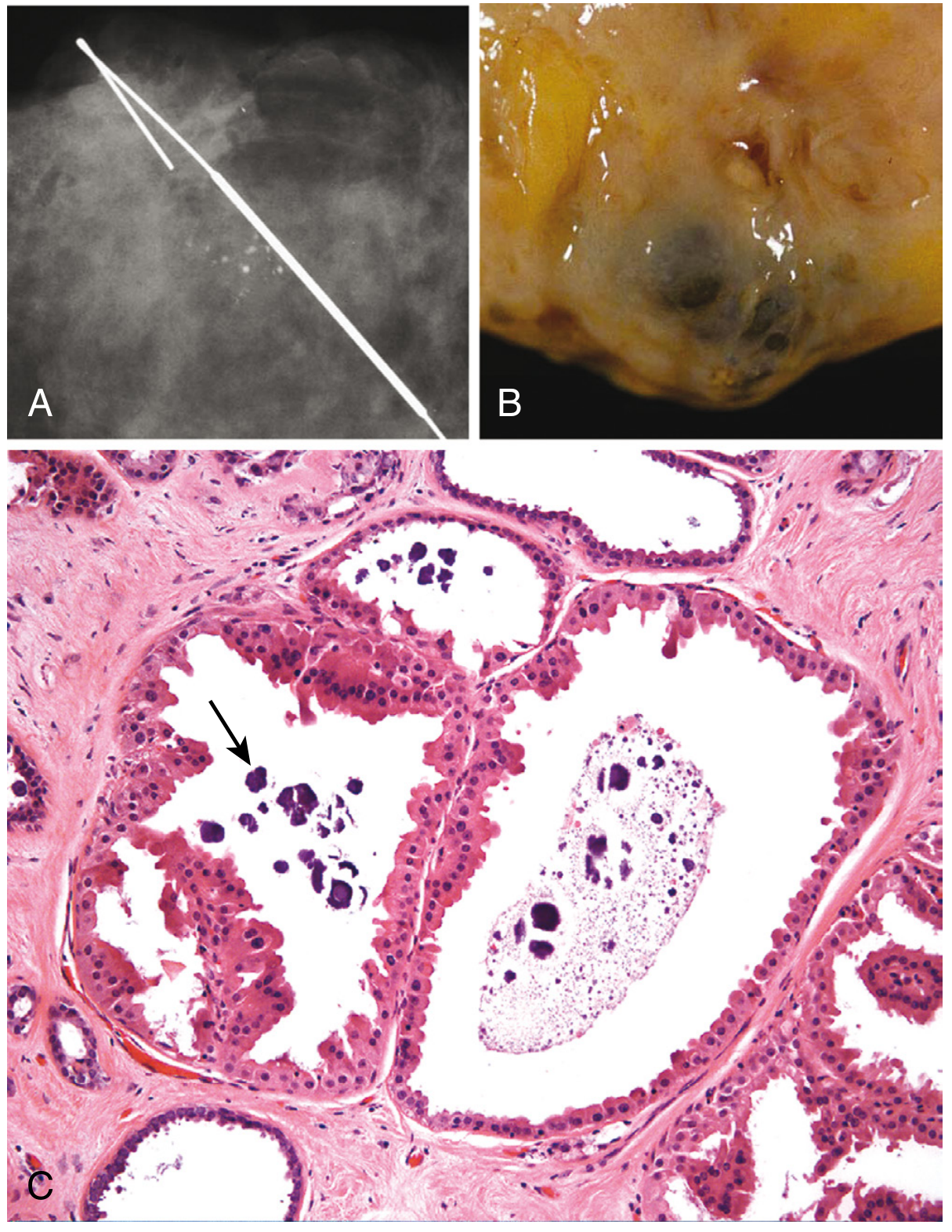
Fig. 5 - Apocrine cysts (benign differential of breast mass) - Robbins & Cotran: (A) clustered calcifications on specimen radiograph, (B) gross blue-dome cysts with dark turbid fluid, (C) microscopy showing apocrine epithelium and intraluminal calcifications (arrow). Diagnosis confirmed by disappearance of mass after FNA.
5. In Situ Carcinoma Histology
Atypical Ductal Hyperplasia (ADH) and Atypical Lobular Hyperplasia (ALH) - Precursor Lesions
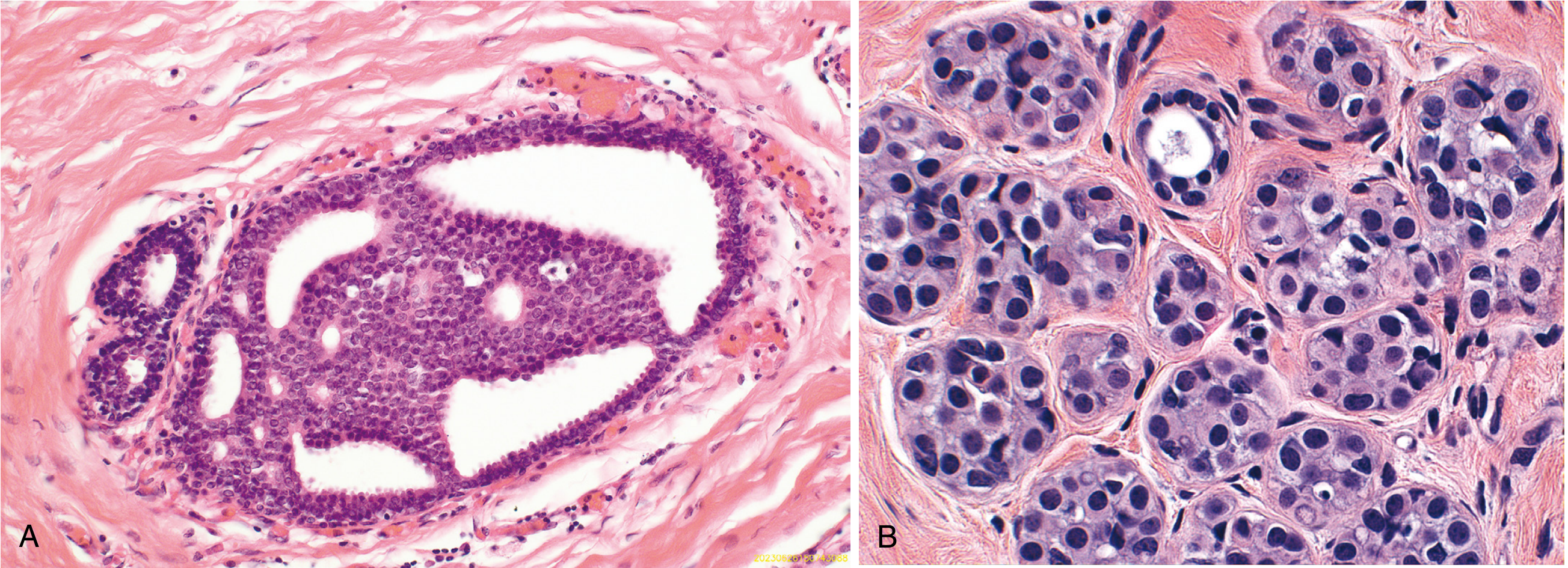
Fig. 6 - Robbins & Cotran, Fig. 23.11:
- (A) Atypical ductal hyperplasia (ADH): Duct partially filled by monotonous rounded cells with cribriform spaces - carries a 4-5x increased lifetime cancer risk
- (B) Atypical lobular hyperplasia (ALH): Small, monomorphic loosely cohesive cells partially filling a lobule
DCIS - Mammographic and Pathological Correlation
Fig. 7 - DCIS correlation - Robbins & Cotran:
- (A) Specimen mammogram: fine calcifications with needle guidance
- (B) Gross: ducts plugged with necrotic material (comedo-type DCIS)
- (C) Microscopy: micropapillary pattern with intraluminal calcifications (arrow)
6. Squamous Metaplasia of Lactiferous Ducts (Important Benign Mimic)
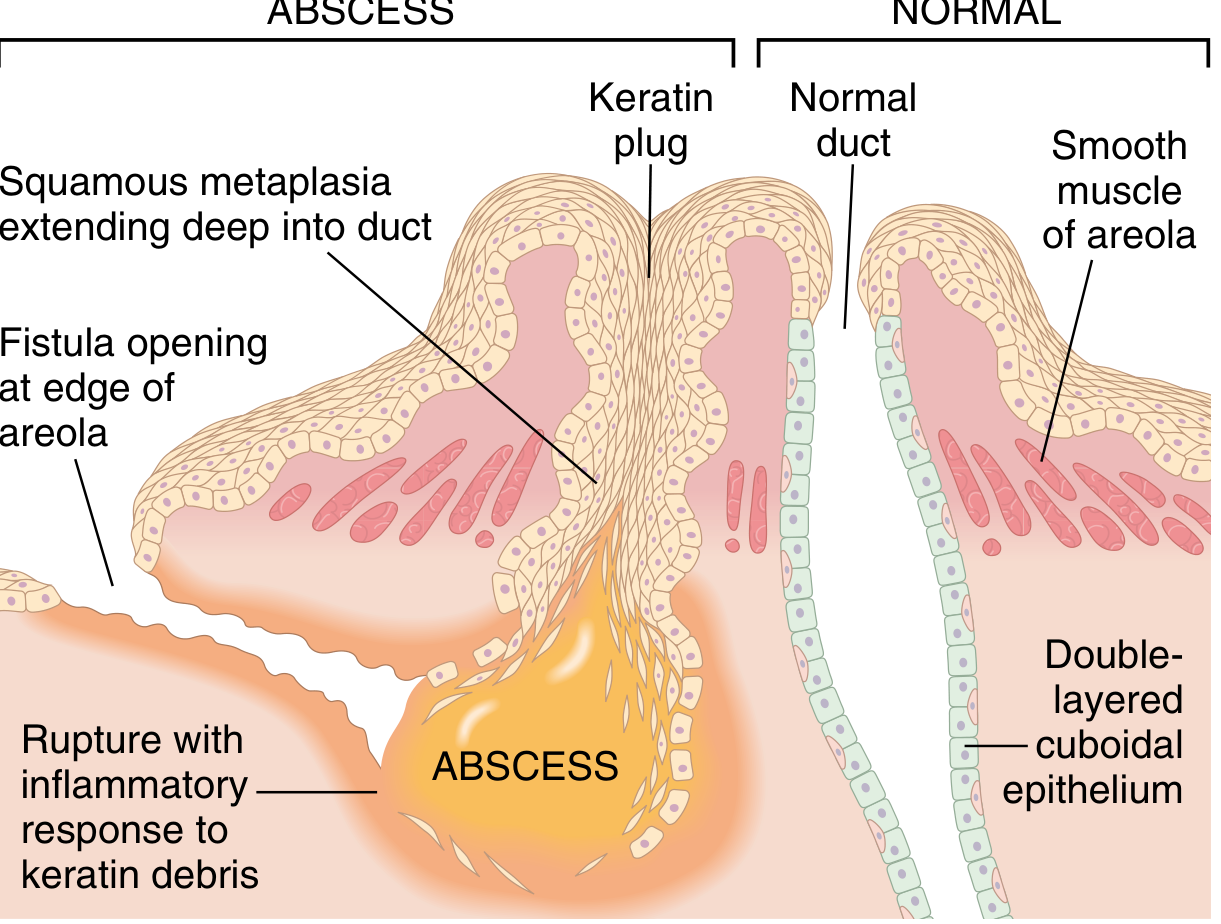
Fig. 8 - Squamous metaplasia of lactiferous ducts vs. normal - Robbins & Cotran, Fig. 23.3. A benign condition (Zuska disease) causing a subareolar abscess that clinically mimics cancer, especially in smokers. Key: failure to improve with antibiotics should prompt imaging and biopsy to exclude malignancy.
7. Prognosis by Lymph Node Status and Tumor Size
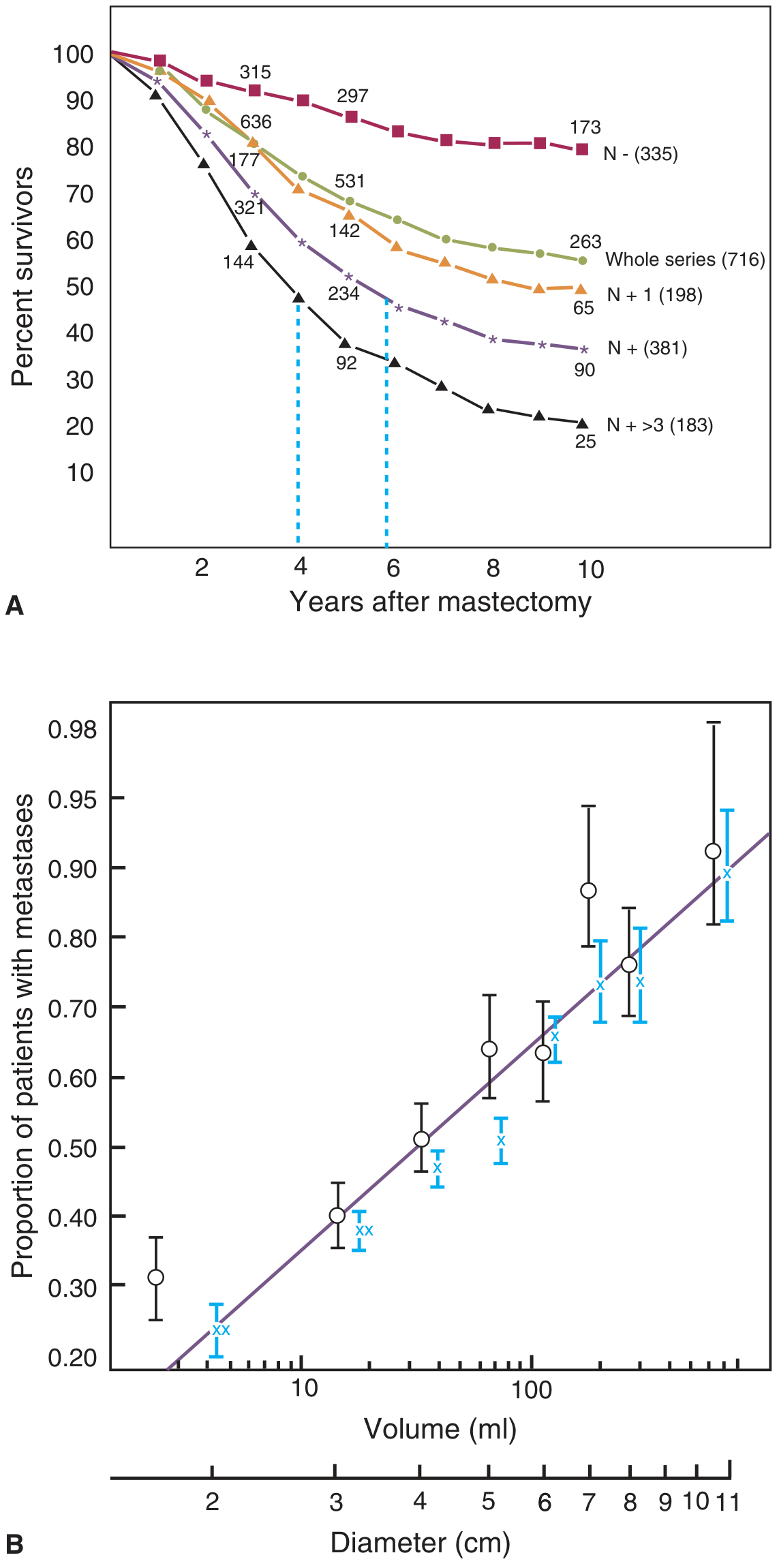
Fig. 9 - Breast cancer prognosis - Schwartz's Principles of Surgery, 11e, Fig. 17-14:
- (A) Survival curves by axillary lymph node status: node-negative (N-) patients have significantly better 10-year survival (>80%) compared to those with >3 positive nodes (<30%)
- (B) Proportion of patients with distant metastases rises sharply as tumor diameter increases - underpinning the importance of early detection
8. AJCC TNM Staging Summary (8th Edition)
T - Primary Tumor
| T Stage | Size/Extent |
|---|---|
| Tis | In situ (DCIS) or Paget with no tumor |
| T1 | ≤20 mm |
| T2 | >20 mm - ≤50 mm |
| T3 | >50 mm |
| T4 | Any size + chest wall/skin extension, IBC |
N - Lymph Nodes (Pathologic)
| N Stage | Nodes Involved |
|---|---|
| pN0 | None |
| pN1mi | Micrometastases (>0.2 mm but ≤2 mm) |
| pN1 | 1-3 axillary nodes |
| pN2 | 4-9 axillary or clinically detected IM nodes |
| pN3 | ≥10 axillary, infraclavicular, supraclavicular, or IM + axillary |
Overall Stage Grouping with 5-Year Survival
| Stage | TNM | 5-yr Survival (All races) |
|---|---|---|
| I | T1, N0, M0 | >99% |
| II | T0-3/N0-1, M0 | 93% |
| III | T0-4/N0-3, M0 (locally advanced) | 75% |
| IV | Any T, Any N, M1 | 29% |
Source: Harrison's Principles of Internal Medicine, 22nd ed. (2025), adapted from CA Cancer J Clin 72:524, 2022
Key Diagnostic Algorithm
Breast symptom / abnormal screening
↓
Clinical examination + Mammography
↓
BI-RADS 1-2 → Routine screening
BI-RADS 3 → Short interval follow-up (6 mo)
BI-RADS 4-5 → CORE NEEDLE BIOPSY (preferred)
↓
Pathology confirms malignancy
↓
Receptor testing (ER, PR, HER2) + Grade
↓
Staging workup:
• Sentinel lymph node biopsy (clinically node-negative)
• CT chest/abdomen/pelvis ± bone scan (T3/T4, N2/N3, or symptomatic)
• PET scan (T3/T4, N2/N3 disease)
↓
Multidisciplinary team discussion → Treatment plan
Sources: Bailey & Love's Surgery 28th ed.; Schwartz's Principles of Surgery 11th ed.; Mulholland & Greenfield's Surgery 7th ed.; Robbins & Cotran Pathologic Basis of Disease; Harrison's Internal Medicine 22nd ed. (2025)
Go
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.