thomas splint in orthopaedics give detailed explanation about history applications
Reading File
Finding Sources
Finding Sources
Searching the Web
Thomas splint orthopaedics history applications traction femur fracture
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative sources. Let me compile the full, detailed answer.
The Thomas Splint - A Detailed Explanation
1. Origins and Inventor
The Thomas splint was first described by Hugh Owen Thomas (1834-1891), a Welsh-born Liverpool surgeon and bonesetter, in his 1875 book "Diseases of the Hip, Knee and Ankle Joints with their Deformities, Treated by a New and Efficient Method." Thomas came from a long line of Welsh bone-setters and is widely considered the father of British orthopaedic surgery.
Thomas was strongly influenced by the concept of physiologic rest - he believed that allowing an injured limb to move continuously prevented healing and argued forcefully for complete rest as a method of treatment. This philosophy underpinned his splint design. He was also motivated by his working-class patient population and wanted a device that was simple, cheap, and accessible to the poorest patients.
His original design was used primarily for tuberculous joint disease of the knee, not fractures. It consisted of:
- A padded metal ring fitted snugly at the groin
- Two iron rods extending distally from the ring
- A smaller ring or crosspiece at the foot end
- Leather strips or tapes supporting the leg
2. Design and Structure
The Thomas splint in its classic form has the following components:
| Component | Description |
|---|---|
| Proximal ring | An oval/circular padded metal ring sized to fit snugly at the ischial tuberosity and perineum |
| Two side rods | Steel rods extending from the ring distally, angled slightly outward, converging to the distal end |
| Distal crosspiece | The two rods meet and cross beyond the foot, allowing traction cords to be tied |
| Fabric slings | Non-stretch bandage slings support the limb at the thigh, knee, and just above the heel |
How to size it: Ring size is determined by measuring the thigh circumference at the groin. Length equals the distance from the crotch to the underside of the heel on the uninjured leg, plus 15-25 cm extra beyond the foot.
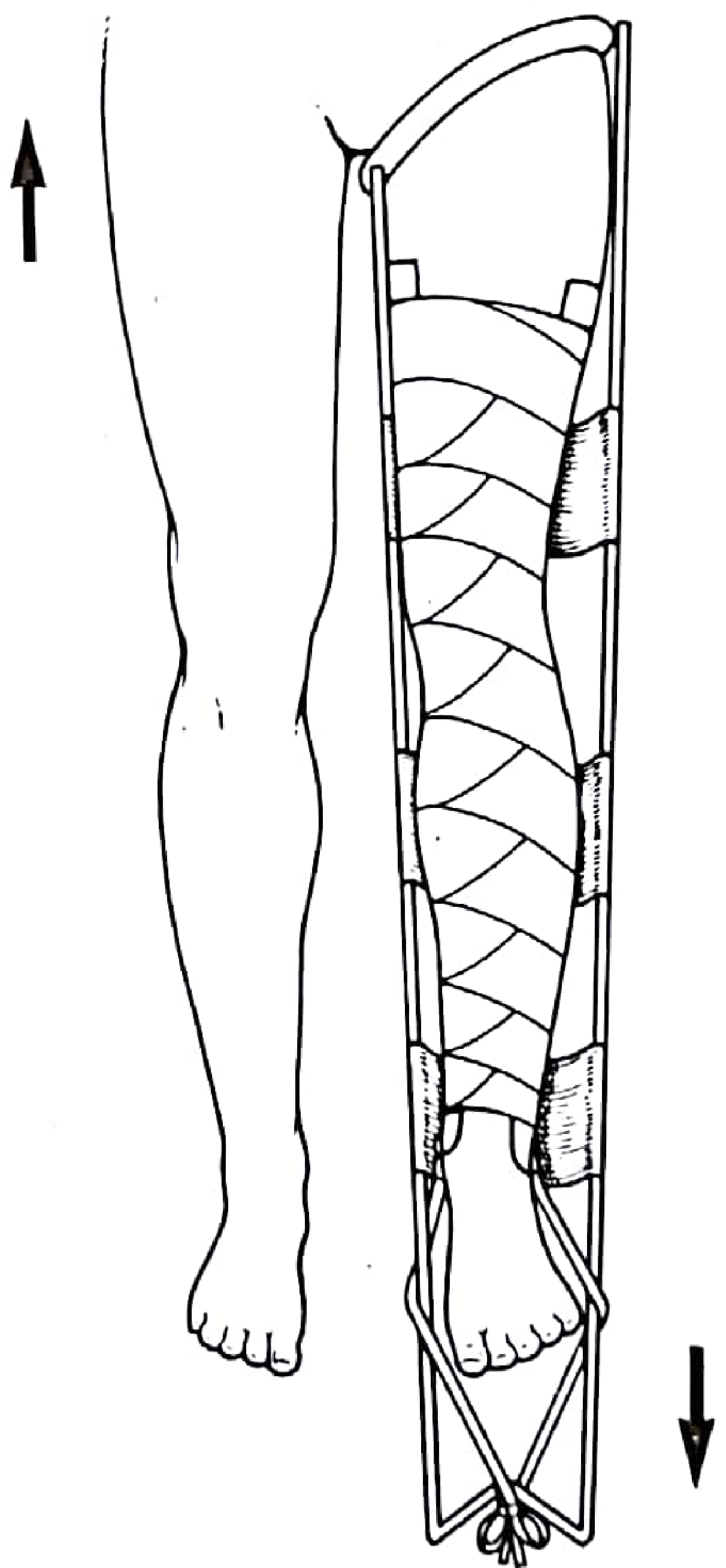
Thomas splint applied with skin traction (from Pye's Surgical Handicraft, 22nd Ed.)
3. Mechanism of Action
The Thomas splint works on a fixed traction (static) principle:
- The proximal ring bears against the ischial tuberosity and acts as the counter-force (fulcrum)
- Traction is applied distally via skin tapes or skeletal pins tied to the distal crosspiece
- The opposing forces reduce overriding of fracture fragments, overcome muscle spasm, and maintain alignment and length
There are two modes of use:
a) Static (Fixed) Traction
The force and counter-force are both contained within the splint itself. The tibial traction pin cord is tightened using a Spanish windlass (a wooden stick used to twist the cord). The ring presses against the ischium. This is a closed, self-contained system suitable for transport and prehospital use.
b) Balanced (Dynamic) Traction
Once in hospital, the splint is suspended from an overhead frame (Balkan beam) and weights are applied to the traction pin cord. The patient's own body weight provides counter-traction. This allows nursing access and some mobility in bed.
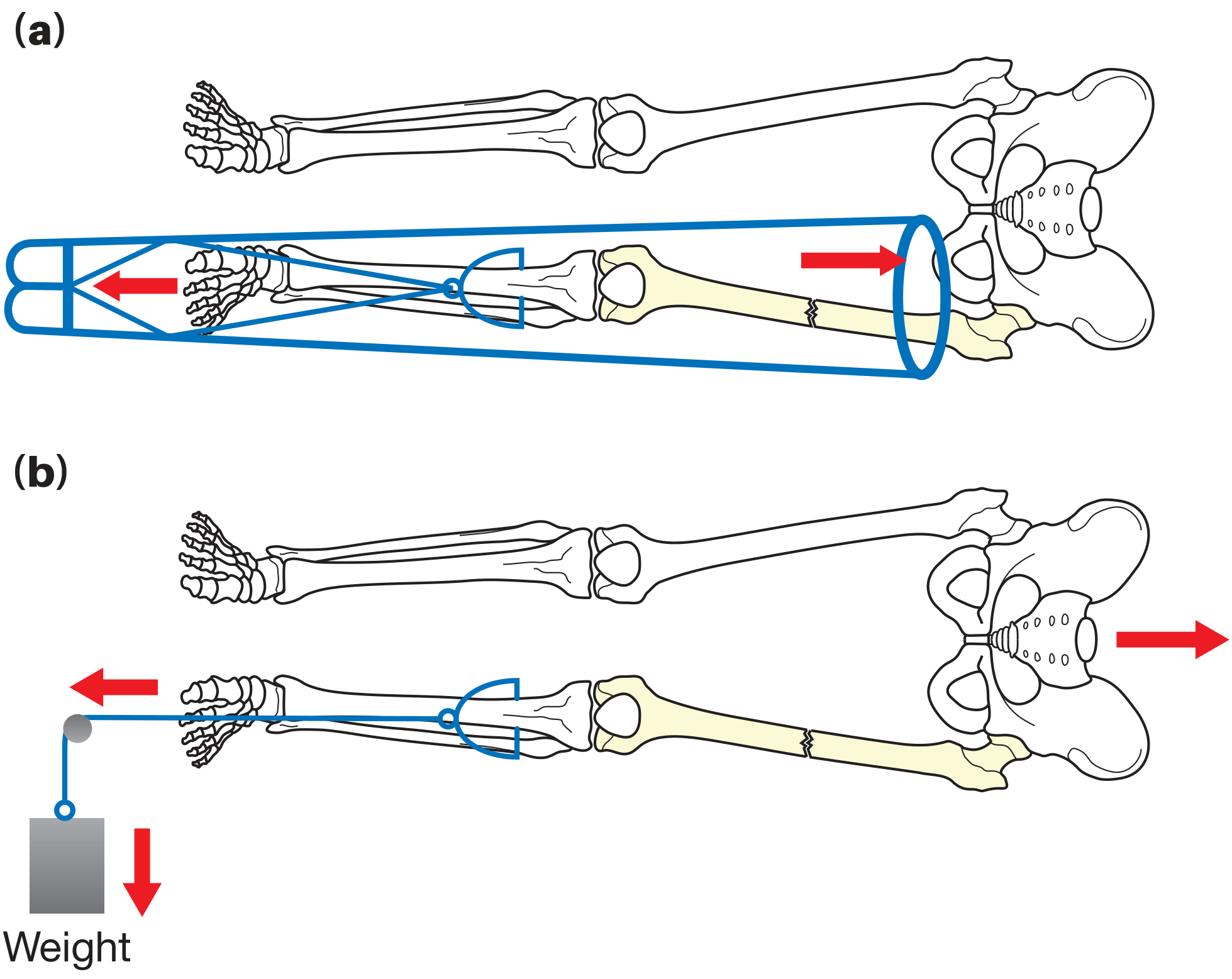
Static vs. balanced traction with Thomas splint (from Bailey and Love's Short Practice of Surgery, 28th Ed.)
4. World War I - The Defining Moment
Although Thomas died in 1891, his splint remained largely unused in mainstream military surgery. It was his nephew, Sir Robert Jones, consultant orthopaedic surgeon to the British Army, who championed the device during the First World War.
Before its widespread adoption, mortality from battlefield femoral shaft fractures was approximately 80% - largely due to blood loss, fat embolism, and inability to immobilize the limb during transport over rough terrain. The powerful thigh muscles caused severe displacement, tenting of the skin, and vascular injury.
In 1916, Robert Jones mandated use of the Thomas splint across the Western Front. The results were dramatic:
Mortality from femoral shaft fractures dropped to approximately 16%
This ~60% reduction in mortality is one of the most cited examples in the history of trauma care of a simple device saving lives at scale. It replaced the older Liston and Hodgen splints that the Royal Army Medical Corps had been using in 1914. (Sources: RJAH Historical Orthopaedic Fact Sheet, Rockwood and Green's Fractures in Adults, 10th ed.)
5. World War II - The Tobruk Splint
In North Africa, a new problem emerged: the jolting and jarring of casualties over long desert distances was agonizing even in a Thomas splint. The solution was the Tobruk splint, named after the 1941 Battle of Tobruk:
- The limb was placed in traction in the Thomas splint as normal
- The splint and limb were then encased in Plaster of Paris
- This gave excellent immobilization while allowing comfortable transport
This remains an instructive example of adapting the Thomas splint to specific tactical and logistical challenges.
6. Clinical Applications
Primary Indication: Femoral Shaft Fractures
Although originally designed as a knee splint, the Thomas splint is now used primarily for femoral shaft fractures. It provides:
- Reduction of muscle spasm and pain
- Restoration of limb length
- Reduction of blood loss into the thigh compartment
- Safe transport of the injured patient
As noted in Pye's Surgical Handicraft (22nd Ed.): "Although originally designed as a knee splint, the Thomas splint now tends to be used mainly to treat fractures of the femoral shaft."
In modern trauma, the Thomas splint is used in the emergency department as a temporary measure to stabilize and comfort a patient with a femoral shaft fracture until definitive surgical fixation (intramedullary nailing) can be performed. Per the IAEM Clinical Guideline (2023), it remains standard emergency department protocol for suspected or confirmed femoral shaft fractures.
Other Applications
- Septic arthritis of the knee - where the knee needs immobilization under close observation
- Complete dislocation of the knee - splinting post-reduction for 4-6 weeks (Pye's Surgical Handicraft)
- Tibial fractures - historically used during World War I
- Acute cervical spine fractures - traction is still used for cervical fractures (though not with the Thomas splint specifically)
- Tuberculous joints - the original application (knee and hip TB)
7. The Thomas Splint with Pearson Knee Attachment
For young, muscular patients where skin traction alone is insufficient to overcome powerful thigh muscles, the splint is modified with a Pearson knee piece attachment:
- A second, smaller Thomas-type splint is attached to the main splint to support the lower leg in a flexed knee position
- A Steinmann pin is inserted through the upper tibia for skeletal traction
- The pin cord is attached to a balanced traction system with weights (usually no more than 10 lbs - over-distraction must be avoided)
- After 2-3 weeks, traction can typically be reduced to 5 lbs with the bed horizontal
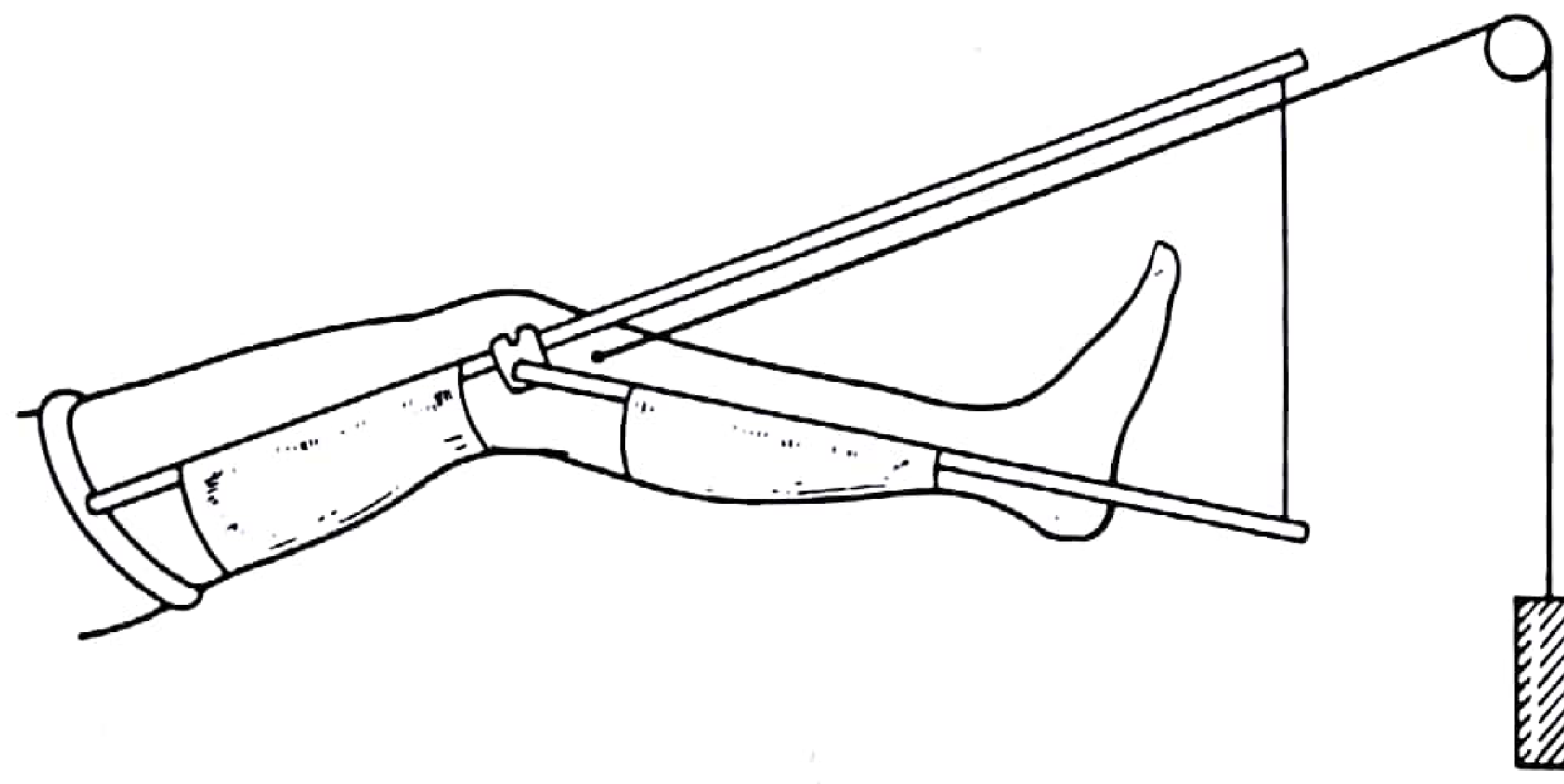
Thomas splint with Pearson knee attachment and skeletal traction (Pye's Surgical Handicraft, 22nd Ed.)
8. Application Technique (Step-by-Step)
From Pye's Surgical Handicraft and the IAEM Clinical Guideline:
- Size selection - Measure thigh circumference at the groin (for ring size). Length = uninjured leg (crotch to heel) + 15-25 cm.
- Prepare slings - Three non-stretch bandage slings are fitted: one under the thigh, one under the knee, one just above the Achilles tendon (heel must not be supported directly).
- Skin extensions - Elastoplast 7.5-10 cm strapping applied to both sides of the limb. The outer strip is placed slightly posterior and the inner strip slightly anterior to counteract external rotation tendency. Extensions are held with crêpe bandages ending just above the malleoli; orthopedic felt pads protect the malleoli.
- Apply traction - Outer tape goes over the lateral bar; inner tape goes under the medial bar (again to counteract rotation). Tapes are tied over the distal crosspiece.
- Increase traction if needed - A wooden windlass bar can be used to increase traction tension.
- Check daily - Sling and tape tension must be assessed and adjusted daily.
9. Complications
| Complication | Mechanism |
|---|---|
| Pressure sores | Over the ischial tuberosity from the ring; over bony prominences from slings |
| Common peroneal nerve palsy | Pressure by the lateral bar at the fibular neck |
| Skin sensitivity / contact dermatitis | Reaction to Elastoplast adhesive |
| Over-distraction | Excessive traction weight causing fracture gap |
| Pin site infection | With Steinmann pin in skeletal traction |
| Thromboembolic complications | From prolonged immobility |
| Joint stiffness | Knee and ankle from prolonged immobilization |
As noted in Pye's Surgical Handicraft: "All such traction devices, many of which require long periods of recumbency in bed...may cause peroneal nerve palsy at the head of the fibula from pressure by the side bar of a Thomas splint."
10. Evolution and Legacy - Modern Derivatives
The Thomas splint's success inspired several modifications, now widely used in emergency medicine and pre-hospital care:
- Hare Traction Splint (1960s, Glen Hare) - A half-ring modification with a ratchet length-adjustment mechanism. More compact and easier to apply in the field. Not suitable for proximal femoral fractures.
- Sager Traction Splint - A unipolar splint applying traction against the ischium; more compact than the original.
- Kendrick Traction Device (KTD) - A lightweight, collapsible version for prehospital and military use.
The Rockwood and Green's Fractures in Adults (10th ed., 2025) notes that intramedullary nailing gradually superseded traction as definitive treatment for femoral fractures through the 1970s-1980s, but traction (and thus the Thomas splint) remains relevant:
- In resource-limited settings as definitive management
- In prehospital and emergency settings as temporary stabilization
- In military medicine (used in the 2003 Gulf conflict; revisited in Afghanistan when external fixators alone proved insufficient)
Summary
The Thomas splint is a 150-year-old device with an essentially unchanged functional design that continues to save lives. Invented by Hugh Owen Thomas in 1875 for tuberculous joints, its true potential was realized by Robert Jones during World War I when it reduced femoral fracture mortality from ~80% to ~16%. Today it serves as a first-line emergency tool for femoral shaft fractures worldwide, operating on a simple but effective biomechanical principle: countertraction against the ischial tuberosity versus distal traction on the limb. Its legacy lives in every modern traction splint in every ambulance and emergency department.
Sources:
- Pye's Surgical Handicraft, 22nd Edition, pp. 185-196
- Bailey and Love's Short Practice of Surgery, 28th Edition, p. 449
- Rockwood and Green's Fractures in Adults, 10th Edition (2025), pp. 315, 321
- RJAH Historical Orthopaedic Fact Sheet - The Thomas Splint
- IAEM Clinical Guideline: Thomas Splint Application (2023)
- EMS Traction Splint - StatPearls/NCBI
This is a shared conversation. Sign in to Orris to start your own chat.