Development of diaphragm and it's anamolies full details for md exam answer 15 marks
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Finding Sources
I now have comprehensive information from authoritative embryology and surgical textbooks. Let me compile the complete MD exam answer.
Development of the Diaphragm and Its Anomalies
INTRODUCTION
The diaphragm is a dome-shaped, musculotendinous partition separating the thoracic and abdominal cavities. It is a composite structure derived from four distinct embryonic components. Several candidate genes on chromosome 15q play a critical role in its development.
EMBRYONIC COMPONENTS (Four Sources)
1. Septum Transversum
- Formed during the 4th week from mesodermal tissue ventrolateral to the body wall
- Grows dorsally, forming a semicircular shelf separating the heart from the liver
- After head folding, it forms a thick, incomplete connective tissue partition between the pericardial and abdominal cavities
- Contributes to the central tendon of the diaphragm
- Large pericardioperitoneal canals persist along the sides of the esophagus at this stage
- The septum subsequently fuses with the dorsal mesentery of the esophagus and pleuroperitoneal membranes
2. Pleuroperitoneal Membranes
- These folds appear at the beginning of the 5th week, extending from the lateral body wall
- They grow medially and ventrally, fusing with the septum transversum and dorsal mesentery of the esophagus by the 6th-7th week
- This fusion completes the partition between thoracic and abdominal cavities, forming the primordial diaphragm
- Although forming large portions of the early fetal diaphragm, they represent relatively small portions of the neonate's diaphragm
- Complete closure of the canal occurs by the 8th week, with the right side closing before the left (clinically important)
3. Dorsal Mesentery of the Esophagus
- The septum transversum and pleuroperitoneal membranes fuse with the dorsal mesentery of the esophagus
- This constitutes the median (mesial) portion of the diaphragm
- The crura of the diaphragm - leg-like diverging muscle bundles crossing in the median plane anterior to the aorta - develop from myoblasts that grow into the dorsal mesentery of the esophagus
4. Muscular Ingrowth from the Lateral Body Walls
- Occurs during the 9th to 12th weeks as the lungs and pleural cavities enlarge, burrowing into the lateral body walls
- Body-wall tissue splits into two layers:
- External layer - becomes part of the definitive abdominal wall
- Internal layer - contributes to the peripheral parts of the diaphragm (external to the pleuroperitoneal membrane-derived portions)
- Further extension forms the costodiaphragmatic recesses, establishing the characteristic dome-shaped configuration
POSITIONAL CHANGES AND INNERVATION
| Feature | Detail |
|---|---|
| Initial position | Opposite C3-C5 cervical somites at 4th week |
| Descent by 6th week | Level of thoracic somites |
| Descent by 8th week | Level of L1 vertebra |
| Motor innervation | Phrenic nerve (C3, C4, C5) - "C3, 4, 5 keeps the diaphragm alive" |
| Sensory - central | Phrenic nerve (superior and inferior surfaces of domes) |
| Sensory - costal border | Lower intercostal nerves (T7-T12), due to origin from lateral body walls |
- During the 5th week, myoblasts from cervical somites migrate into the developing diaphragm, carrying their nerve fibers with them - this is why the phrenic nerve arises from C3-5
- The rapid growth of the dorsal embryo causes apparent caudal descent of the diaphragm, explaining why the phrenic nerves are ~30 cm long in adults
- The phrenic nerves pass through the pleuropericardial membranes - this is why they lie on the fibrous pericardium in adults
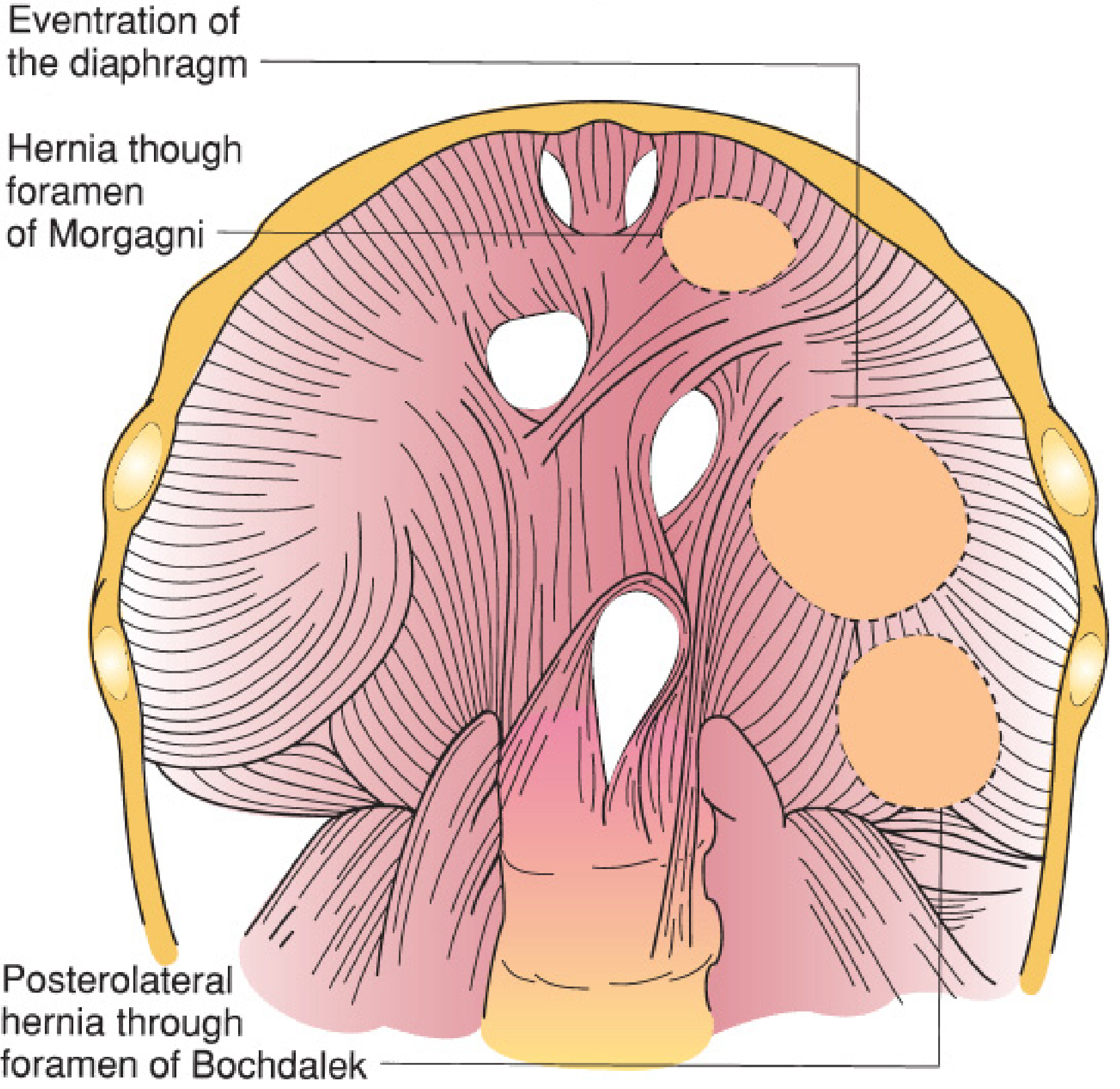
ANOMALIES OF THE DIAPHRAGM
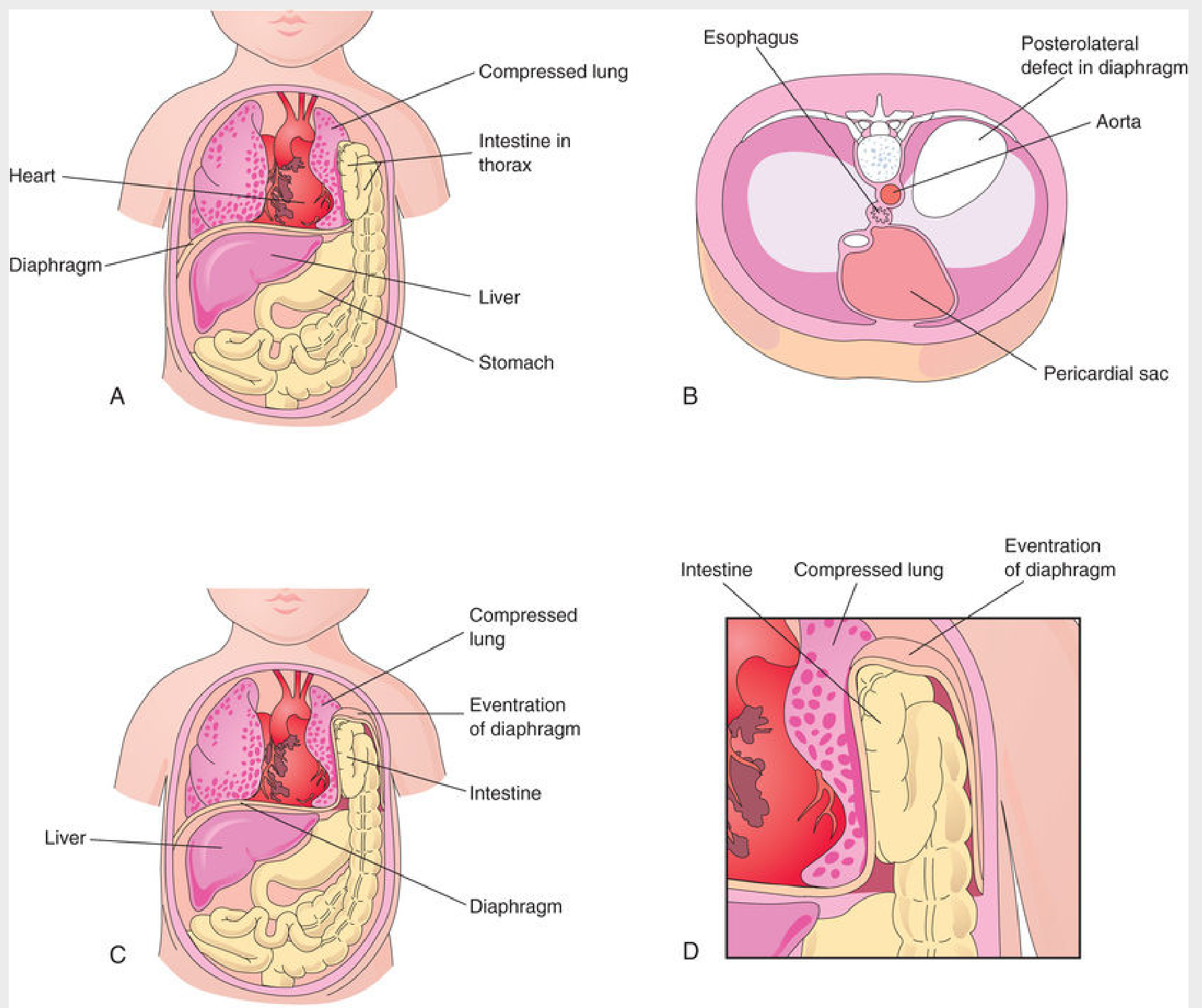
A. Posterolateral Defect (Bochdalek Hernia) - MOST COMMON
Incidence: 1 in 2200-5000 neonates; accounts for ~70-75% of all CDH
Pathogenesis:
- Results from defective formation and/or failure of fusion of the pleuroperitoneal membranes with the other three diaphragmatic components
- Creates a large opening in the posterolateral region (lumbocostal triangle/foramen of Bochdalek)
- If closure of the pleuroperitoneal canal has not occurred by the time the midgut returns to the abdomen (9th-10th weeks), abdominal viscera herniate into the thorax
- No hernia sac is present if herniation occurs before complete closure; a non-muscularized membrane forms a sac in ~10-15% of cases
Laterality:
- Left side in 85-90% of cases (right side closes earlier due to earlier right pleuroperitoneal membrane fusion)
- Right in 13%; bilateral in ~2%
Contents of hernial sac: Stomach, intestine, spleen, colon, left lobe of liver (left-sided); liver dominates the right hemithorax in right-sided defects
Clinical features:
- Severe respiratory distress at birth
- Scaphoid abdomen
- Heart and mediastinum displaced to the right (left-sided hernia)
- Absent breath sounds on affected side
- Bowel sounds in chest
- Polyhydramnios in utero
Complications:
- Pulmonary hypoplasia (most common cause) - both ipsilateral and contralateral, ipsilateral more severe; fewer bronchial branches, reduced alveolar surface area
- Pulmonary hypertension - increased arteriolar smooth muscle thickness, decreased cross-sectional vascular area
- Persistent fetal circulation (right-to-left shunting through foramen ovale and ductus arteriosus)
- Abnormal intestinal rotation and fixation
Genetic associations: Chromosome 15q26 (GATA6, GATA4, ZFPM2, NR2F2, WT1); deletions at 8p23.1 and 4p16.3
Diagnosis: Prenatal ultrasound (as early as 15 weeks), MRI - bowel/liver in thorax, mediastinal shift, polyhydramnios
Treatment: Surgical repair after hemodynamic stabilization; inhaled nitric oxide for pulmonary hypertension; ECMO in severe cases; survival 65-90%
B. Retrosternal (Parasternal) Hernia - Morgagni Hernia
Incidence: ~23-28% of CDH; uncommon overall
Pathogenesis:
- Herniation through the sternocostal hiatus (foramen of Morgagni) - the opening between the sternal and costal parts of the diaphragm, through which the superior epigastric vessels pass
- Results from incomplete fusion of sternal and costal components at the anterior diaphragm
Side: Usually right-sided (right cardiophrenic angle mass on X-ray)
Contents: Omentum most commonly; may contain bowel (colon, stomach)
Clinical features:
- Often asymptomatic, discovered incidentally on chest X-ray
- May present with epigastric pain, respiratory symptoms, or bowel obstruction
- Anterior mediastinal mass on lateral chest film
Complications: Intestinal herniation into the pericardial sac, or conversely, part of the heart descending into the peritoneal cavity
C. Eventration of the Diaphragm
Pathogenesis:
- Not a true diaphragmatic hernia - it is a superior displacement of viscera into a sac-like outpouching
- One half of the diaphragm has defective musculature (failure of muscular tissue from the body wall to extend into the pleuroperitoneal membrane on that side)
- The affected half balloons into the thoracic cavity as a thin aponeurotic/membranous sheet
- Abdominal viscera are displaced superiorly into the pocket-like outpouching
- Some cases are acquired (phrenic nerve injury)
Clinical significance: May simulate CDH clinically (respiratory distress, mediastinal shift), but is distinct in that there is no true defect in the diaphragm
D. Congenital Hiatal Hernia
- Part of the fetal stomach herniates through an excessively large esophageal hiatus
- Usually acquired in adult life, but a congenitally enlarged hiatus may predispose
- The esophageal hiatus transmits the esophagus and vagus nerves
E. Accessory Diaphragm
- Rare anomaly (>30 cases reported)
- Most often on the right side
- Associated with lung hypoplasia and other respiratory complications
- Diagnosed by MRI or CT; treated by surgical excision
SUMMARY TABLE OF DIAPHRAGMATIC ANOMALIES
| Anomaly | Location | Side | Cause | Key Feature |
|---|---|---|---|---|
| Bochdalek hernia | Posterolateral | Left (85%) | Failure of pleuroperitoneal membrane fusion | Most common CDH; pulmonary hypoplasia |
| Morgagni hernia | Anterosternal | Right | Incomplete sternal-costal fusion | Omentum/colon; often asymptomatic |
| Eventration | Any | Either | Defective muscular ingrowth | No true defect; membranous pouch |
| Hiatal hernia | Esophageal hiatus | Central | Large hiatus | Stomach/GEJ herniation |
| Accessory diaphragm | Variable | Right | Unknown | Very rare |
EMBRYOLOGICAL BASIS OF CLINICAL IMPORTANCE
- Why left side is affected more - The right pleuroperitoneal membrane closes first; the left side is therefore still open when the midgut returns to the abdomen at 9-10 weeks
- Why referred pain from diaphragm is felt at shoulder tip - Central diaphragm is supplied by C3-5 phrenic nerve, same segment supplying the shoulder
- Why phrenic nerve is so long (~30 cm) - The diaphragm descends from its cervical origin (C3-5) to the thoracolumbar junction as the embryo grows
- Pulmonary hypoplasia in CDH - Visceral herniation at critical phase of lung branching (5-16 weeks) compresses the lung and disrupts both ipsilateral and contralateral development; sonic hedgehog signaling is also delayed
Sources: The Developing Human: Clinically Oriented Embryology (Moore & Persaud), 10th ed.; Sabiston Textbook of Surgery, 21st ed.; Mulholland and Greenfield's Surgery, 7th ed.
It's applied anatomy?
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
I now have comprehensive applied anatomy content. Let me compile the full MD exam answer.
Applied Anatomy of the Diaphragm
(15-mark MD Exam Answer)
I. INTRODUCTION
The diaphragm is a dome-shaped, musculotendinous partition sealing the inferior thoracic aperture and separating the thoracic cavity from the abdominal cavity. It is the principal muscle of respiration, accounting for ~70% of the tidal volume during quiet breathing.
II. GROSS STRUCTURE
The diaphragm consists of:
- A central tendinous part (central tendon) - a trefoil (three-leaflet) sheet of strong fibrous tissue
- Peripheral muscular part - radially arranged muscle fibers that arise from the margins of the inferior thoracic aperture and converge into the central tendon
The diaphragm is not flat - it balloons upward on both sides to form two domes. The right dome is higher than the left (reaches rib V in expiration), because of the underlying liver. The left dome reaches the 5th intercostal space.
III. ATTACHMENTS (ORIGIN)
Sternal Part
- Two muscular slips from the posterior surface of the xiphoid process
Costal Part
- Inner surfaces of the lower six costal cartilages and their adjacent ribs (ribs 7-12), interdigitating with transversus abdominis
Vertebral / Lumbar Part - via Two Crura and Three Arcuate Ligaments
Crura:
| Crus | Vertebral attachment |
|---|---|
| Right crus (longer, thicker) | Anterolateral bodies of L1, L2, L3 and intervertebral discs |
| Left crus | Anterolateral bodies of L1, L2 and disc |
The crura blend with the anterior longitudinal ligament of the vertebral column.
Arcuate Ligaments (3 pairs):
| Ligament | Attachment | Structure it arches over |
|---|---|---|
| Median arcuate | Connects two crura across midline | Aorta |
| Medial arcuate | Transverse process of L1 (lateral) to side of body of L1/L2 (medial) | Psoas major muscle |
| Lateral arcuate | Transverse process of L1 (medial) to rib XII (lateral) | Quadratus lumborum muscle |
IV. OPENINGS IN THE DIAPHRAGM
Three major openings transmit important structures:
| Opening | Level | Contents |
|---|---|---|
| Aortic hiatus | T12 (between the two crura, behind median arcuate ligament) | Aorta, thoracic duct, sometimes azygos vein |
| Esophageal hiatus | T10 (in the muscular part of the right crus) | Esophagus, anterior and posterior vagal trunks, esophageal branches of left gastric artery and vein, lymphatics |
| Caval opening (IVC foramen) | T8 (in the central tendon, to the right of midline) | Inferior vena cava, right phrenic nerve |
Additional smaller passages:
- Greater, lesser, and least splanchnic nerves - through the crura
- Hemi-azygos vein - through the left crus
- Sympathetic trunks - posterior to the medial arcuate ligament
- Superior epigastric vessels - anterior to the diaphragm, deep to ribs (between sternal and costal origins = sternocostal triangle / foramen of Morgagni)
- Left phrenic nerve - through the muscular part just anterior to the central tendon on the left side
Mnemonic for level of openings: "I 8 (ate) 10 eggs AT 12"
- IVC = T8, Esophagus = T10, Aorta = T12
V. RELATIONS
Superior (Thoracic) Surface
- Right dome: Right lung and pleura, right lobe of liver
- Left dome: Left lung and pleura, fundus of stomach, spleen
- Central: Pericardium and heart (fibrous pericardium is adherent to the central tendon)
Inferior (Abdominal) Surface
- Right: Right lobe of liver, right kidney, right suprarenal gland
- Left: Left lobe of liver, stomach, spleen, left kidney, left suprarenal gland
- Centrally: Covered by peritoneum except where bare area of liver is in contact
VI. BLOOD SUPPLY
| Surface | Arteries | Source |
|---|---|---|
| Superior (thoracic) | Superior phrenic arteries | Thoracic aorta |
| Superior | Pericardiacophrenic and musculophrenic arteries | Internal thoracic artery |
| Inferior (abdominal) | Inferior phrenic arteries (largest supply) | Abdominal aorta (first branches) |
Venous drainage parallels the arteries; the right inferior phrenic vein drains to the IVC, the left to the left suprarenal vein or directly to the IVC.
VII. NERVE SUPPLY
| Nerve | Supply | Levels |
|---|---|---|
| Phrenic nerves (right and left) | Motor to entire diaphragm including crura; Sensory to central diaphragm (peritoneum and pleura over central dome) | C3, C4, C5 (major contribution C4) |
| Lower intercostal nerves (T7-T12) | Sensory only - peripheral part of diaphragm | T7-T12 |
Route of phrenic nerves:
- Arises from cervical plexus in the neck
- Descends vertically in the neck on the anterior surface of scalenus anterior
- Enters thorax through the superior thoracic aperture
- Passes through the mediastinum anterior to the lung roots, between mediastinal pleura and pericardium
- Right phrenic enters diaphragm through the caval opening with the IVC
- Left phrenic pierces the muscular part of the left dome separately
VIII. ACTION AND PHYSIOLOGY
- On contraction: domes descend, vertical diameter of thorax increases, intrathoracic pressure falls - air enters lungs; simultaneously, intra-abdominal pressure rises
- At rest (end-expiration): right dome at rib V, left dome at 5th intercostal space
- After contraction (end-inspiration): both domes descend ~1.5 cm
- The right dome is always higher than the left because of the underlying liver
IX. APPLIED ANATOMY (CLINICALLY IMPORTANT POINTS)
1. Referred Pain to the Shoulder Tip
- Central diaphragm is supplied by the phrenic nerve (C3, C4, C5)
- Any irritation of the central diaphragm (subphrenic abscess, blood, free air under the diaphragm, ruptured spleen, ectopic pregnancy, perforated peptic ulcer) refers pain to the tip of the shoulder (C4 dermatome) and the root of the neck
- The peripheral diaphragm is supplied by intercostal nerves T7-T12; irritation here refers pain to the lower chest and abdominal wall
- Clinically: Post-operative free gas under the right diaphragm causes right shoulder tip pain. Splenic injury causes left shoulder tip pain (Kehr's sign)
2. Hiccup (Singultus)
- A sudden, involuntary contraction of the diaphragm, causing rapid inhalation stopped by glottis closure
- Triggered by stimulation of the phrenic nerve, vagus nerve, or direct irritation of the diaphragm
- Causes include gastric distension, uremia, CNS lesions, pericarditis
- Persistent hiccup may indicate a serious underlying pathology (e.g., esophageal carcinoma, mediastinal tumor, brainstem lesion)
3. Diaphragmatic Paralysis (Phrenic Nerve Palsy)
- Causes: Lung cancer (most important - never miss), malignant mediastinal lymph nodes, aortic aneurysm, postviral neuropathy (varicella zoster), trauma, iatrogenic (cardiac surgery, neck dissection), cervical spondylosis (C3-C5 root compression)
- Signs: Elevated hemidiaphragm on the affected side on chest X-ray; paradoxical movement (rises on inspiration = "paradoxical" - because intra-thoracic negative pressure sucks the flaccid diaphragm up)
- Unilateral: Usually asymptomatic; mild dyspnea on exertion
- Bilateral: Severe respiratory distress; orthopnea prominent (diaphragm falls away from chest wall when supine)
- Treatment: Surgical plication if symptomatic (creates folds in the paralyzed diaphragm)
4. Subphrenic Abscess
- Collection of pus between the diaphragm and the underlying viscera
- Right subphrenic space (between right lobe of liver and diaphragm) is most common
- The diaphragm is irritated from below, causing referred right shoulder pain, hiccup, and pleural effusion
- Chest X-ray shows elevated hemidiaphragm, pleural effusion, and air-fluid level below the diaphragm
5. Diaphragmatic Hernias (Applied)
| Type | Site of defect | Contents | Clinical notes |
|---|---|---|---|
| Bochdalek (posterolateral) | Failure of pleuroperitoneal membrane fusion; lumbocostal triangle | Stomach, bowel, spleen | Most common (85% left); respiratory distress at birth; scaphoid abdomen |
| Morgagni (retrosternal) | Sternocostal triangle (foramen of Morgagni) | Omentum, colon | Right-sided; often asymptomatic; anterior cardiophrenic angle mass on X-ray |
| Hiatus hernia | Esophageal hiatus (enlarged) | Stomach | Sliding (most common) or rolling (para-esophageal) type; GERD, dysphagia |
| Eventration | No true defect; failure of muscular ingrowth | Viscera displaced into membranous pouch | Mimics CDH; often acquired after phrenic nerve injury |
6. Aortic Aneurysm and the Median Arcuate Ligament
- The aorta passes behind the diaphragm through the aortic hiatus (T12) - it is NOT compressed during diaphragmatic contraction (important surgical and physiological point)
- Median arcuate ligament syndrome: Compression of the celiac axis by a low-placed median arcuate ligament causes postprandial angina and mesenteric ischemia
7. Thoracoabdominal Wounds
- Stab wounds below the level of the nipple (anteriorly, 4th intercostal space) or the tip of the scapula (posteriorly) can penetrate both the thoracic and abdominal cavities, injuring the diaphragm
- This must always be suspected in lower thoracic trauma; laparoscopy is used to assess the diaphragm
8. Costodiaphragmatic Recess
- The potential space between the lowest extent of the parietal pleura and the uppermost extent of the diaphragm
- Clinically: Site of pleural effusion accumulation; requires ~300 mL of fluid before visible on erect chest X-ray (blunting of costophrenic angle); site for diagnostic thoracocentesis
9. Pneumoperitoneum
- Free gas under the diaphragm (best seen under the right dome on erect CXR) is a classical sign of hollow viscus perforation (perforated peptic ulcer)
- The gas irritates the diaphragm, causing referred right shoulder tip pain
10. Liver and Right Dome
- The right dome of the diaphragm sits directly on the right lobe of the liver - elevation of the right dome on CXR may indicate hepatomegaly, right lobe abscess, or right subphrenic collection rather than a primary diaphragmatic problem
X. EMBRYOLOGICAL BASIS OF CLINICAL ANOMALIES (Brief)
- Diaphragm develops from four components: septum transversum (central tendon), pleuroperitoneal membranes, dorsal mesentery of esophagus, and muscular ingrowth from lateral body walls
- Failure of fusion of any component causes the corresponding hernia at that site
- The diaphragm's cervical origin (C3-5) explains the long phrenic nerve and shoulder-tip referred pain
SUMMARY TABLE
| Feature | Detail |
|---|---|
| Levels of openings | IVC: T8; Esophagus: T10; Aorta: T12 |
| Higher dome | Right (liver pushes it up) |
| Motor nerve | Phrenic (C3, C4, C5) |
| Largest blood supply | Inferior phrenic arteries (from abdominal aorta) |
| Central tendon embryology | Septum transversum |
| Crura embryology | Dorsal mesentery of esophagus |
| Most common CDH | Bochdalek (posterolateral, left-sided) |
| Referred pain site | Shoulder tip (C4 dermatome) |
Sources: Gray's Anatomy for Students (Drake, Vogl, Mitchell), 4th ed.; Gray's Anatomy for Students block1 & block2; Bailey and Love's Short Practice of Surgery, 28th ed.; Sabiston Textbook of Surgery, 21st ed.
This is a shared conversation. Sign in to Orris to start your own chat.