Deep neck spaces detail p from dhingra book of ent
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed to write a comprehensive answer. Note: the library does not contain Dhingra's book specifically, but KJ Lee's Essential Otolaryngology and Cummings Otolaryngology are the two premier ENT references with essentially the same content on deep neck spaces. Let me now compile the complete answer.
Deep Neck Spaces - Detailed Notes (ENT)
Note: Dhingra's Diseases of Ear, Nose & Throat is not in this textbook library. The following is drawn from K.J. Lee's Essential Otolaryngology (Chapter 37 - Neck Spaces and Fascial Planes) and Cummings Otolaryngology Head and Neck Surgery (Chapter 9), which cover the same anatomy in comparable depth and are the standard ENT references for this topic.
Fascial Layers of the Neck (Foundation)
Understanding deep neck spaces requires knowledge of the fascia that creates them.
Superficial Cervical Fascia
- Envelopes the platysma and muscles of facial expression
- Extends from the zygomatic process superiorly to the clavicle inferiorly
- Significance: Acts as the main plane of resistance to spread of cellulitis into the deep neck; allows skin mobility over deep structures
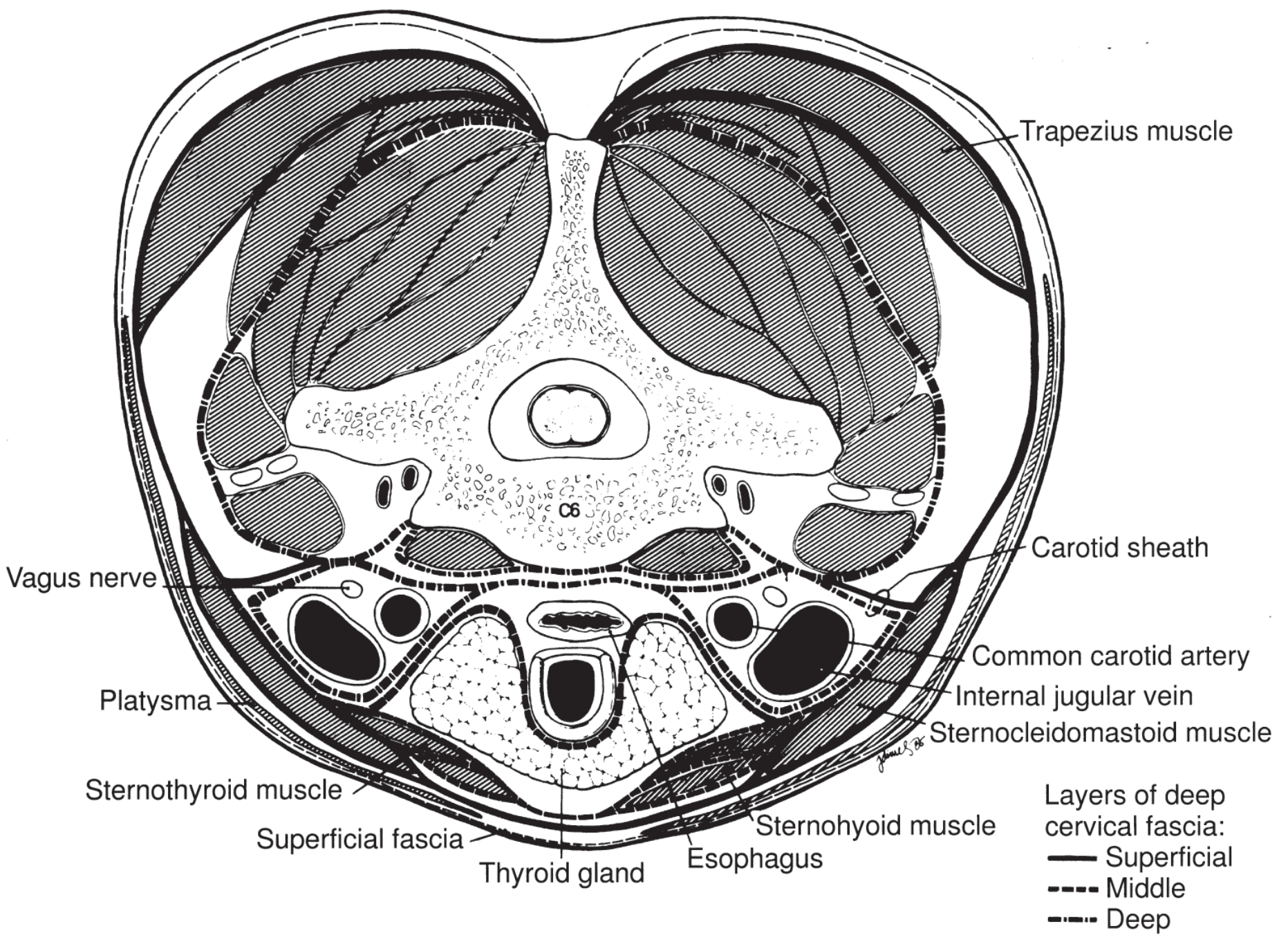
Deep Cervical Fascia (Three Layers)
A. Superficial (Investing) Layer
- Envelopes SCM, trapezius, masseter, and medial pterygoid muscles; also envelopes the parotid and submandibular glands
- Attaches to: occiput, mastoid, zygomatic arch, lower border of mandible, hyoid bone, clavicle, acromion, spine of scapula
B. Middle Layer - has two divisions:
- Muscular division - covers strap muscles (sternohyoid, sternothyroid, thyrohyoid, omohyoid); extends from hyoid to thorax
- Visceral division - forms the pretracheal fascia (over trachea) and buccopharyngeal fascia (overlies the pharyngeal wall = anterior border of retropharyngeal space). The buccopharyngeal fascia forms the midline raphe and the pterygomandibular raphe
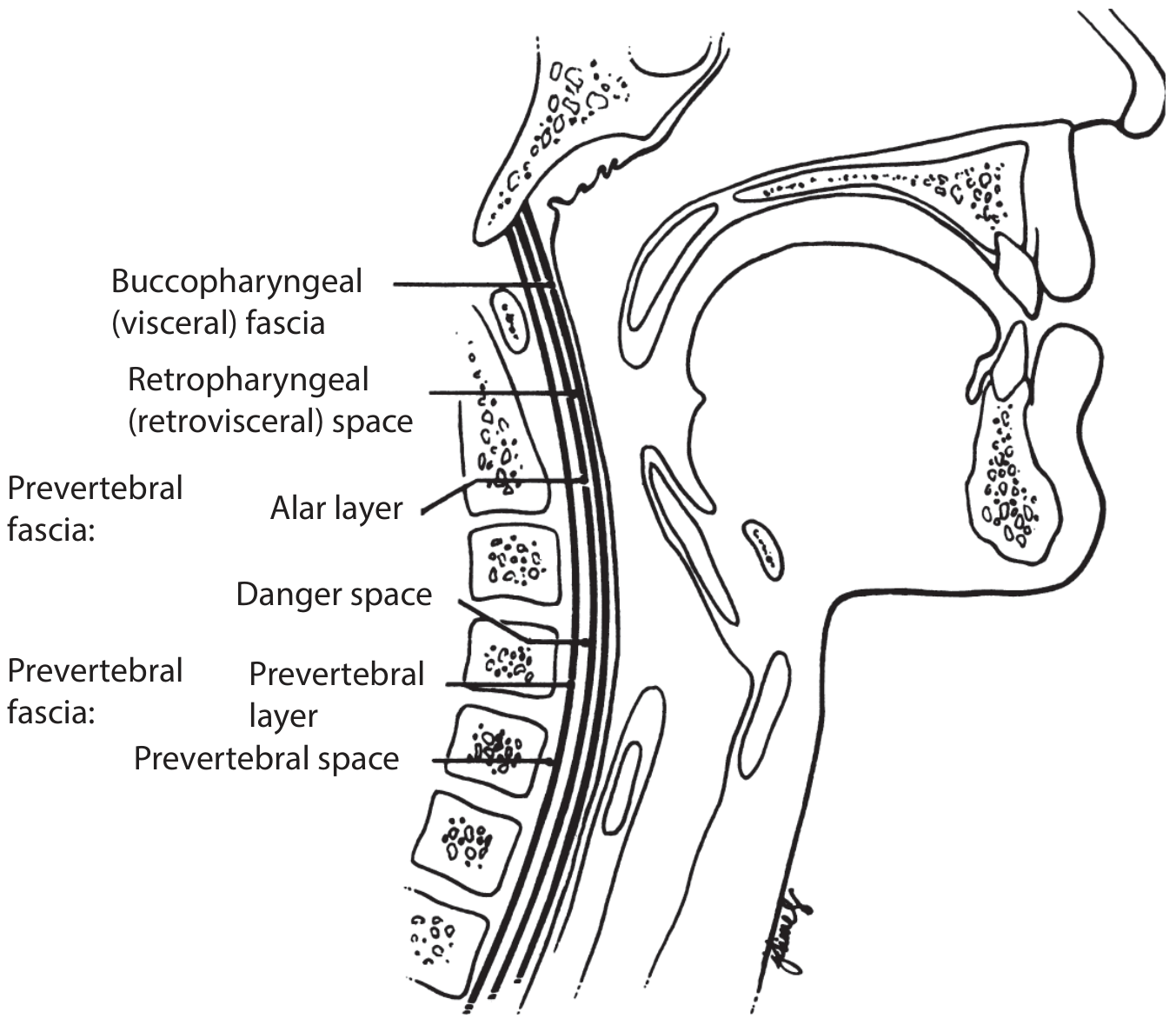
C. Deep Layer (Prevertebral Fascia) - has two sub-layers:
- Prevertebral layer - covers vertebral bodies, paraspinous and scalene muscles; attaches to transverse processes laterally; extends base of skull to coccyx
- Alar layer - lies between the prevertebral layer and the visceral layer; covers the cervical sympathetic trunk; extends base of skull to mediastinum
The Danger Space lies between the alar and prevertebral layers.
D. Carotid Sheath Fascia
- Comprises contributions from all three layers of deep cervical fascia
- Envelopes: common carotid artery, internal jugular vein, vagus nerve
- Extends from base of skull to the thorax
- Known as the "Lincoln Highway of the Neck" - a potential avenue for rapid spread of infection
The Deep Neck Spaces
1. Peritonsillar Space (Paratonsillar Space)
| Feature | Detail |
|---|---|
| Medial | Palatine tonsil |
| Lateral | Superior constrictor muscle |
| Contents | Loose connective tissue; tonsillar branches of lingual, facial, ascending pharyngeal vessels |
| Communicates with | Parapharyngeal space |
| Clinical note | Peritonsillar abscess (quinsy) - most common deep neck infection; may extend to parapharyngeal space |
2. Parapharyngeal Space (Lateral Pharyngeal / Pterygomaxillary Space)
This is the central hub - it communicates with nearly all other deep neck spaces, making it the most clinically important space.
Boundaries:
- Superior: base of middle cranial fossa
- Inferior: hyoid bone
- Anterior: pterygomandibular raphe
- Posterior: prevertebral fascia
- Medial: pharyngobasilar fascia (superiorly), superior constrictor muscle
- Lateral: deep lobe of parotid gland, mandible, medial pterygoid muscle
The styloid process divides it into two compartments:
Prestyloid (Muscular / Anterior) Compartment:
- Fat
- Lymph nodes
- Internal maxillary artery
- Inferior alveolar, lingual, auriculotemporal nerves
- Medial and lateral pterygoid muscles
- Deep lobe of parotid tissue
Poststyloid (Neurovascular / Posterior) Compartment:
- Carotid artery (internal carotid)
- Internal jugular vein
- Sympathetic chain
- Cranial nerves IX (glossopharyngeal), X (vagus), XI (accessory), XII (hypoglossal)
Communicates with: Peritonsillar, submandibular, visceral, retropharyngeal, carotid, masticator, parotid spaces
Clinical tip: A mass in the parapharyngeal space displaces the tonsil medially; this differentiates it from a peritonsillar abscess. Parapharyngeal tumors can mimic peritonsillar swelling on exam but absence of pain/inflammation and CT imaging reveal the true nature.
3. Masticator Space
| Feature | Detail |
|---|---|
| Medial | Fascia medial to pterygoid muscles |
| Lateral | Fascia overlying masseter |
| Contents | Masseter muscle, pterygoid muscles, ramus and posterior body of mandible, inferior alveolar nerve |
| Communicates with | Parotid, pterygomaxillary, visceral spaces |
| Source of infection | Dental infections, especially third molar |
4. Submandibular Space
Boundaries:
- Superior: floor of mouth
- Inferior: digastric muscle
- Anterior: mylohyoid and anterior belly of digastric
- Posterior: posterior belly of digastric and stylomandibular ligament
- Medial: hyoglossus and mylohyoid
- Lateral: skin, platysma, mandible
The mylohyoid line divides it into two sub-compartments:
Sublingual (Supramylohyoid) Space:
- Contains: sublingual gland, Wharton's duct, lingual nerve
- Infections: premolars and first molar (apex above mylohyoid line)
- Clinically: marked intraoral lingual swelling, tongue elevation; minimal extraoral swelling
Submaxillary / Submandibular (Inframylohyoid) Space:
- Contains: submandibular gland, lymph nodes, hypoglossal nerve (anteriorly), facial vein and artery, marginal branch of facial nerve
- Infections: second and third molars (apex below mylohyoid line)
- Clinically: swelling at inferior lateral border of mandible extending to digastric area
Ludwig's Angina = Bilateral infection of all three primary mandibular spaces (bilateral sublingual + bilateral submaxillary + submental). Described by Wilhelm Friedrich von Ludwig in 1836. Characterized by rapid, bilateral gangrenous cellulitis, gross swelling, tongue elevation/displacement, and brawny induration of submental region above hyoid. Minimal fluctuance. Clinical diagnosis - no imaging required.
5. Submental Space
- Between the two anterior bellies of digastric
- Contains: submental lymph nodes, anterior jugular veins
- One of the three primary mandibular spaces (along with bilateral submandibular spaces) involved in Ludwig's angina
6. Parotid Space
| Feature | Detail |
|---|---|
| Medial | Parapharyngeal space |
| Lateral | Parotid fascia |
| Contents | Parotid gland, facial nerve (CN VII), external carotid artery, posterior facial (retromandibular) vein |
| Communicates with | Parapharyngeal, temporal fossa, masticator spaces |
7. Temporal Fossa
| Feature | Detail |
|---|---|
| Superior | Temporal line of skull |
| Inferior | Zygomatic arch |
| Lateral | Temporalis fascia |
| Medial | Pterion of skull |
| Contents | Temporalis muscle, temporal fat pad |
| Communicates with | Infratemporal fossa, pterygomaxillary fossa |
8. Infratemporal Fossa
Boundaries:
- Superior: sphenoid and temporal skull, fossa medial to zygomatic arch
- Anterior: infraorbital fissure, maxilla
- Lateral: ramus and coronoid of mandible
- Medial: lateral pterygoid plate with tensor and levator palatine muscles
Contents:
- Pterygoid muscles, temporalis tendon
- Internal maxillary artery
- Pterygoid venous plexus
- Mandibular nerve (V3) with otic ganglion
Communicates with: Temporal fossa, pterygomaxillary (pterygopalatine) fossa
9. Pterygopalatine (Pterygomaxillary) Fossa
Boundaries:
- Superior: sphenoid body, orbital process of palatine bone
- Anterior: posterior wall of maxillary antrum
- Posterior: pterygoid process, greater wing of sphenoid
- Medial: palatine bone (nasal mucoperiosteum)
- Lateral: temporalis muscle via pterygomaxillary fissure
Contents:
- Maxillary nerve (V2)
- Sphenopalatine ganglion
- Internal maxillary artery
Communicates with: Infratemporal fossa, parapharyngeal space, masticator space, temporal fossa
10. Carotid Space (Carotid Sheath Space)
Boundaries:
- Anterior: sternocleidomastoid
- Posterior: prevertebral space
- Medial: visceral space
- Lateral: sternocleidomastoid
Contents:
- Carotid artery
- Internal jugular vein
- Vagus nerve (CN X)
- Ansa cervicalis
Clinical significance: Called the "Lincoln Highway of the Neck" - infections tracking here can spread rapidly to the mediastinum
11. Visceral Space (Pretracheal Space)
Boundaries:
- Superior: hyoid bone
- Inferior: mediastinum (T4 level / arch of aorta)
- Anterior: superficial layer of deep cervical fascia
- Posterior: retropharyngeal space / prevertebral fascia
- Lateral: parapharyngeal space / carotid fascia
Contents:
- Pharynx, esophagus, larynx, trachea, thyroid gland
12. Retropharyngeal Space (Retrovisceral Space)
Boundaries:
- Superior: base of skull
- Inferior: superior mediastinum / tracheal bifurcation (T4) - where middle layer of deep cervical fascia fuses with alar layer
- Anterior: pharynx and esophagus (buccopharyngeal fascia)
- Posterior: alar fascia
- Medial: midline raphe of superior constrictor muscle (causes unilateral abscess in this space)
- Lateral: carotid sheath
Contents:
- Retropharyngeal lymph nodes (Nodes of Rouviere - drain sinuses, nasopharynx, posterior nasal cavity; relevant in pediatric infections)
- Connective tissue
Clinical notes:
- More common in children <6 years (nodes involute with age)
- Plain film: >5 mm prevertebral soft tissue at C2 in children, >7 mm in adults = retropharyngeal infection until proven otherwise
- Air-fluid level on lateral neck X-ray is diagnostic
13. Danger Space (Space 4)
Boundaries:
- Superior: base of skull
- Inferior: diaphragm (most dangerous - extends the full length of the trunk!)
- Anterior: alar fascia of deep layer of deep cervical fascia
- Posterior: prevertebral fascia of deep layer of deep cervical fascia
Contents: Loose areolar tissue
Why it is dangerous: Named for the potential for extremely rapid spread of infection through this loose areolar tissue from the skull base all the way to the diaphragm. Infection in this space can lead to mediastinitis with very high mortality.
14. Prevertebral Space
Boundaries:
- Superior: base of skull
- Inferior: coccyx (extends entire length of vertebral column)
- Anterior: prevertebral fascia
- Posterior: vertebral bodies
Contents: Prevertebral and paravertebral muscles, vertebral column
Clinical note: Infections here tend to be from vertebral osteomyelitis (Pott's disease - TB). Forms a "cold abscess" - no fever, pointing from each side of vertebral column.
Summary: Spaces by Extent
| Space | Superior | Inferior |
|---|---|---|
| Parapharyngeal | Base of skull | Hyoid bone |
| Retropharyngeal | Base of skull | T4 (bifurcation) |
| Danger space | Base of skull | Diaphragm |
| Prevertebral | Base of skull | Coccyx |
| Visceral / Pretracheal | Hyoid | T4 (arch of aorta) |
| Carotid sheath | Base of skull | Thorax |
Fascial Layer Quick Reference
| Fascia | Envelopes | Extends |
|---|---|---|
| Superficial (investing) | SCM, trapezius, masseter, med. pterygoid, parotid, submandibular gland | Occiput/mastoid to clavicle |
| Middle - muscular | Strap muscles | Hyoid to thorax |
| Middle - visceral (buccopharyngeal) | Pharyngeal wall | Base of skull to mediastinum |
| Deep - prevertebral layer | Vertebral bodies, paraspinous, scalene | Base of skull to coccyx |
| Deep - alar layer | Cervical sympathetic trunk | Base of skull to mediastinum |
| Carotid sheath | CCA, IJV, vagus | Base of skull to thorax |
Spread of Infection - Key Points
-
Peritonsillar → Parapharyngeal: Most common route of spread
-
Parapharyngeal → Retropharyngeal / Carotid space: Infection spreads posteriorly or laterally
-
Retropharyngeal → Danger space: Via the alar fascia, can reach mediastinum (descending necrotizing mediastinitis)
-
Danger space: Reaches diaphragm - most life-threatening spread
-
Ludwig's angina: Bilateral submandibular/sublingual spaces → secondary spaces (parapharyngeal, retropharyngeal)
-
K.J. Lee's Essential Otolaryngology, Chapter 37 - Neck Spaces and Fascial Planes
-
Cummings Otolaryngology Head and Neck Surgery, Chapter 9 - Deep Neck Space Infections
This is a shared conversation. Sign in to Orris to start your own chat.