Shwanomma
Reading File
Finding Sources
Finding Sources
Searching PubMed
schwannoma
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough, textbook-based overview of Schwannoma (also called neurilemmoma):
Schwannoma (Neurilemmoma)
Definition & Origin
A schwannoma is a benign, encapsulated nerve sheath tumor arising from Schwann cells of myelinated peripheral nerves. It can arise virtually anywhere in the body but shows a strong predilection for certain sites. - Harrison's Principles of Internal Medicine 22e, p. 765; Andrews' Diseases of the Skin, p. 719
Epidemiology & Location
- Age range: 14-81 years, average ~40 years
- Most common single site: The vestibular (8th cranial) nerve - giving rise to vestibular schwannomas (acoustic neuromas), which account for ~9% of all primary brain tumors
- Head and neck: 25-45% of all schwannomas
- Sinonasal: Only ~4% of schwannomas; most arise from ophthalmic/maxillary divisions of CN V
- Peripheral (skin/soft tissue): Usually along main nerve trunks of the extremities, especially flexor surfaces of arms, wrists, and knees; also scalp, neck, and tongue
- Spine/pelvis: Can involve sacral plexus or sciatic nerve
Associations
| Condition | Association |
|---|---|
| NF2 (chr 22q mutation) | Bilateral vestibular schwannomas; multiple schwannomas (schwannomatosis) |
| NF1 | Increased spinal nerve root schwannomas |
| Carney syndrome | Melanotic psammomatous schwannoma + spotty pigmentation + myxomas + endocrine overactivity |
Pathology
Gross
- Well-demarcated, encapsulated nodule, 3-30 mm (peripheral) or larger
- Firm to rubbery, yellow-tan or pale pink
- May become cystic when >3-4 cm
Histology - the hallmark is two tissue patterns:
| Pattern | Description |
|---|---|
| Antoni A | Compact spindle cells with nuclear palisading; contains Verocay bodies (two rows of palisading nuclei separated by fibrillary material) |
| Antoni B | Loose, myxoid/edematous stroma; ectatic (thick-walled) blood vessels; cystic spaces; considered degenerative |
- Source: Andrews' Diseases of the Skin, p. 719; Campbell's Operative Orthopaedics 15e, p. 1262
Immunohistochemistry
- S-100 protein: Strongly and diffusely positive (hallmark)
- Vimentin: Positive
- Myelin basic protein: Positive in hard (Antoni A-dominant) schwannomas
- EMA: Positive in perineurial capsule
- Neurofilament stain (Bodian): Very few/no nerve fibers within the tumor bulk; compressed nerve may be visible at one edge
Special variants
- Ancient schwannoma: Marked nuclear atypia without mitoses - a benign degenerative change; must not be confused with malignant peripheral nerve sheath tumor (MPNST)
- Plexiform schwannoma: Single or multiple, in dermis/subcutaneous tissue; may be associated with NF-1 or NF-2
- Melanotic psammomatous schwannoma: Associated with Carney syndrome; contains Verocay bodies + EMA-positive capsule
Imaging
MRI (modality of choice)

Postgadolinium MRI of a right vestibular schwannoma - the tumor involves the internal auditory canal (Harrison's, Fig. 95-6)
- Vestibular schwannoma: Densely enhancing mass enlarging the internal auditory canal, extending into the cerebellopontine angle (CPA); differential includes meningioma
- Peripheral schwannoma: Fusiform mass along the course of a major nerve
- Split fat sign: Rim of fat on T1 around the mass
- Target sign: Decreased T2 signal centrally, increased T2 peripherally (~50% of cases) - suggests benign diagnosis
- Antoni A-dominant tumors: intermediate T1 and T2 signal
- Antoni B-dominant tumors: hyperintense on T2 (loose myxoid stroma)
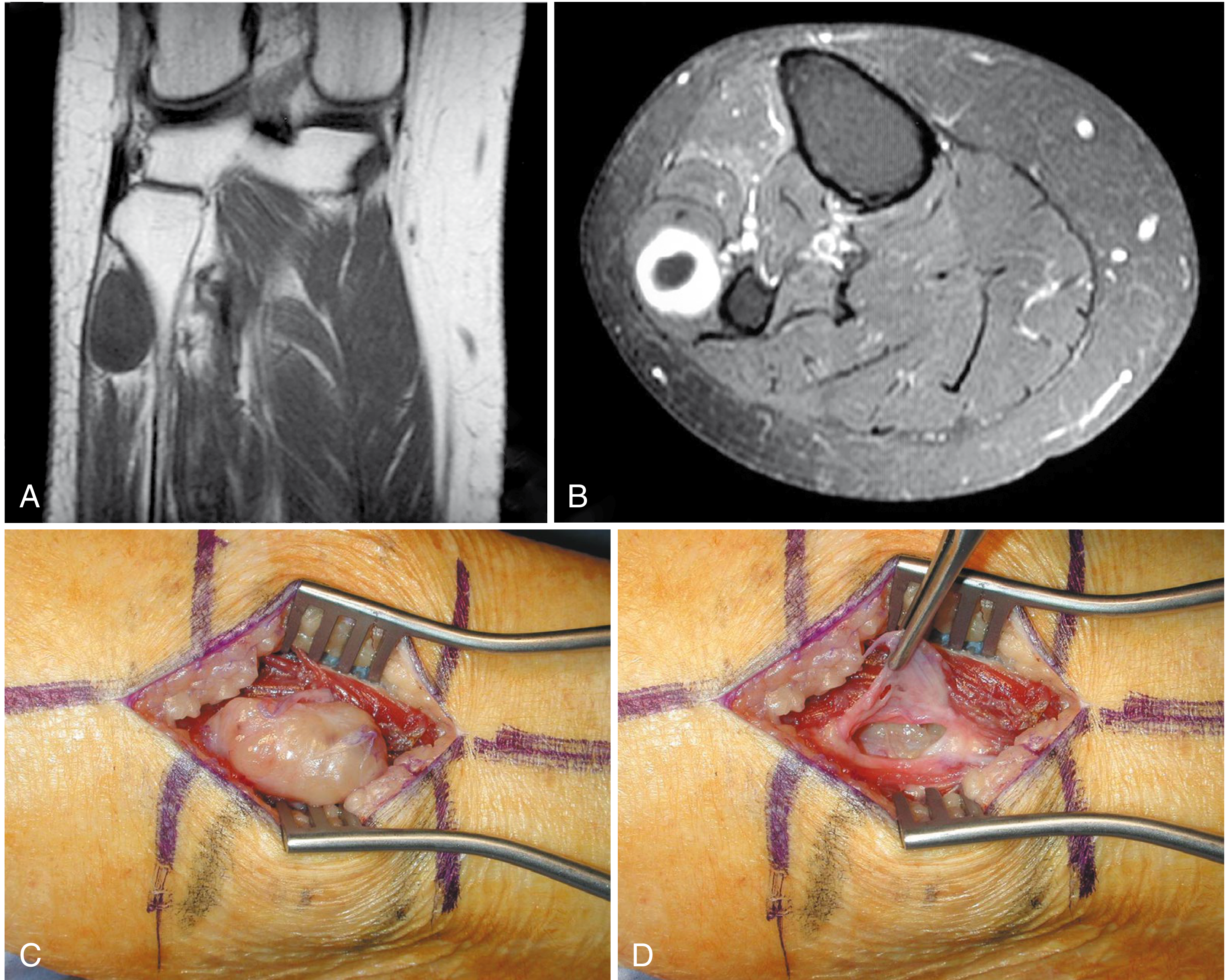
A: T1 coronal MRI - fusiform mass. B: Axial CT. C-D: Intraoperative - tumor dissected free from nerve (Campbell's Operative Orthopaedics 15e, Fig. 30.5)
Clinical Features
Peripheral schwannomas
- Soft or firm nodule, may or may not be painful
- Tinel sign may be positive on percussion (rare with other soft-tissue masses)
- Symptoms from nerve compression: paresthesias, radicular pain
Vestibular schwannoma (acoustic neuroma)
- Progressive unilateral sensorineural hearing loss
- Dizziness, tinnitus
- If large: brainstem/cerebellar compression
- May be found incidentally on neuroimaging
Sinonasal schwannoma
- Headache, facial pain, nasal obstruction, epistaxis, anosmia, diplopia/proptosis, Horner syndrome
Differential Diagnosis
- Neurofibroma (not encapsulated, nerve runs through it, associated with NF-1)
- Meningioma (for vestibular/CPA lesions)
- MPNST (malignant peripheral nerve sheath tumor) - mitoses present, arises in NF-1 neurofibromas
- Solitary fibrous tumor, leiomyoma, fibrous histiocytoma, fibrosarcoma
Treatment
| Location | Treatment |
|---|---|
| Peripheral nerve | Careful blunt dissection through epineurium; tumor spreads nerve fibers apart, allowing nerve-sparing excision |
| Vestibular (small, asymptomatic) | Serial MRI observation ("watch and wait") |
| Vestibular (larger/symptomatic) | Surgery or stereotactic radiosurgery (SRS) |
| Sinonasal | Radical surgery; endoscopic transnasal approach increasingly preferred |
- Excision is almost invariably curative for benign schwannomas
- Recurrence rate is very low (3% in sinonasal series; ~0% in recent endoscopic series)
- Malignant variety (MPNST): Wide resection + radiotherapy required
Recent Evidence (2025)
A 2025 systematic review of clinical practice guidelines for vestibular schwannoma management (Khan et al., Eur Arch Otorhinolaryngol) evaluated current guideline quality for treatment decisions - relevant for the observation-vs-intervention dilemma in small vestibular schwannomas. [PMID: 40782158]
Sources: Harrison's Principles of Internal Medicine 22e | Andrews' Diseases of the Skin | Campbell's Operative Orthopaedics 15e | Cummings Otolaryngology | Andrews' Dermatology
Red nucleus
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Here is a comprehensive, textbook-based account of the Red Nucleus:
Red Nucleus (Nucleus Ruber)
Location & Naming
The red nucleus is a paired, oval-shaped structure in the midbrain tegmentum, at the level of the superior colliculus. Its name comes from its distinctive pinkish hue in freshly dissected brain tissue (rubro = Latin for "red"), caused by iron-containing pigment and a rich vascular supply. - Neuroscience: Exploring the Brain, 5e
Structure - Two Subdivisions
The red nucleus has two functionally distinct parts:
| Division | Location | Key Connections |
|---|---|---|
| Magnocellular (caudal, smaller in humans) | Caudal portion | Receives input from interposed cerebellar nuclei (emboliform + globose); gives rise to the rubrospinal tract |
| Parvocellular (rostral, dominant in humans) | Rostral portion | Receives input from dentate nucleus; projects to inferior olive via the central tegmental tract |
- Neuroanatomy through Clinical Cases, 3e; Guyton & Hall Medical Physiology
Connections (Inputs & Outputs)
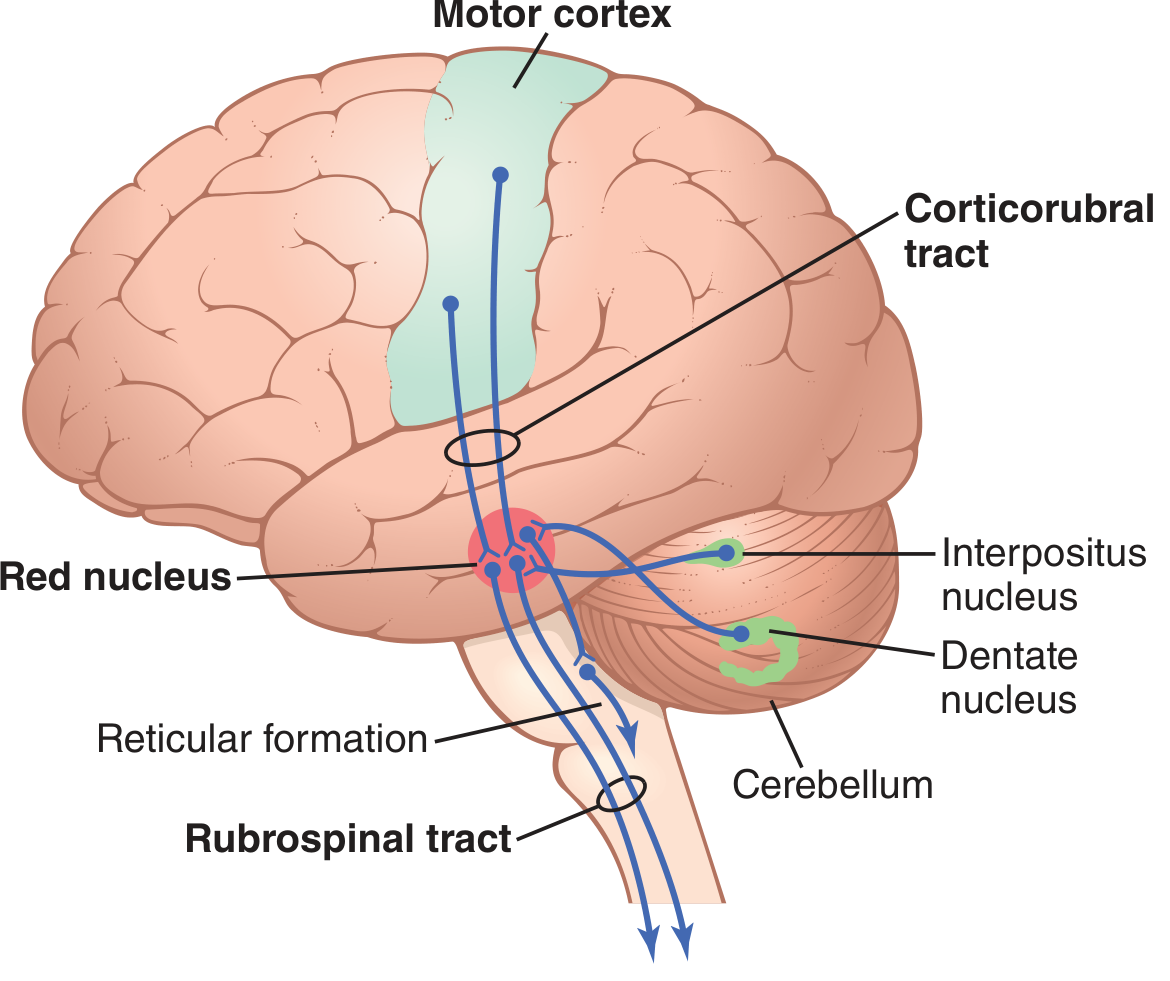
The corticorubrospinal pathway (Guyton & Hall, Fig. 56.5)
Inputs to the Red Nucleus
- Primary motor cortex - via the corticorubral tract (direct fibers + collaterals of the corticospinal tract as it passes through the mesencephalon)
- Interposed cerebellar nuclei (emboliform + globose) - via the superior cerebellar peduncle (brachium conjunctivum) - to the magnocellular division
- Dentate nucleus - output fibers penetrate the red nucleus; some terminate in the parvocellular division
Outputs from the Red Nucleus
- Rubrospinal tract - from the magnocellular division:
- Crosses immediately (decussates in the ventral tegmental decussation of Forel)
- Descends in the lateral column of the spinal cord, adjacent to the corticospinal tract
- Terminates on interneurons and anterior motor neurons in the intermediate gray matter, controlling distal limb muscles (especially flexors)
- Central tegmental tract - from the parvocellular division:
- Projects ipsilaterally down to the inferior olivary nucleus (part of the Guillain-Mollaret triangle)
Function
1. Accessory Motor Pathway (Corticorubrospinal System)
The red nucleus serves as an alternative/accessory route for transmitting motor cortex commands to the spinal cord. Key points:
- The magnocellular portion has a somatotopic map of all muscles (less precise than motor cortex, especially in humans)
- Stimulation of a single point produces contraction of a muscle or small muscle group
- Together with the corticospinal tract, it forms the lateral motor system of the cord, controlling distal limb movements
- When the corticospinal tract is destroyed but the rubrospinal pathway is intact: discrete voluntary movements survive, but fine finger and hand movements are impaired; wrist movements are preserved
- When both are destroyed: severe impairment of fractionated limb/hand movements (confirmed in Lawrence & Kuypers' primate lesion studies)
2. Cerebellar Relay
- Acts as a key relay in cerebellar motor circuits:
- Parvocellular red nucleus → inferior olive → cerebellum (part of the dentatorubro-olivary loop)
- Interposed nuclei → magnocellular red nucleus → rubrospinal tract (influencing lateral motor control)
3. Evolutionary Note
In humans, the rubrospinal tract is relatively small - its functions have been largely taken over by the expanded corticospinal tract during primate evolution. The parvocellular division (cerebellar relay role) is proportionally dominant in humans. - Neuroscience: Exploring the Brain, 5e
Guillain-Mollaret Triangle
A key anatomical circuit involving the red nucleus:
Red Nucleus (midbrain)
|
Central tegmental tract (descending, ipsilateral)
↓
Inferior Olivary Nucleus (medulla)
|
Olivocerebellar fibers (crossing via inferior cerebellar peduncle)
↓
Contralateral Cerebellum (dentate/interposed nuclei)
|
Superior cerebellar peduncle (crossing back up)
↑
Red Nucleus
Clinical relevance: Lesions disrupting this triangle (e.g., in the central tegmental tract or inferior olive) cause palatal myoclonus (also called palatal tremor) and can cause hypertrophic degeneration of the inferior olive. - Localization in Clinical Neurology, 8e
Clinical Syndromes Involving the Red Nucleus
Benedikt Syndrome
A midbrain tegmental lesion (usually posterior cerebral artery infarct) involving:
- Ipsilateral CN III palsy (with dilated pupil) - fascicle involvement
- Contralateral hemiataxia with intention tremor - red nucleus destruction
- Contralateral hemiparesis with hyperreflexia - involvement of the corticospinal tract
Claude Syndrome
More dorsal midbrain lesion affecting the dorsal red nucleus + brachium conjunctivum:
- Ipsilateral CN III palsy
- Prominent contralateral cerebellar signs (ataxia, asynergia, dysmetria, dysdiadochokinesis)
Nothnagel Syndrome
- Unilateral or bilateral CN III palsy + contralateral cerebellar ataxia
Source: Localization in Clinical Neurology, 8e, p. 946
Summary Table
| Feature | Detail |
|---|---|
| Location | Midbrain tegmentum, level of superior colliculus |
| Color | Pinkish-red (iron pigment + vascularity) |
| Subdivisions | Magnocellular (caudal) + Parvocellular (rostral) |
| Main input | Motor cortex, interposed nuclei, dentate nucleus |
| Main output (magno) | Rubrospinal tract (crosses → lateral spinal cord) |
| Main output (parvo) | Central tegmental tract → inferior olive |
| Function | Accessory motor pathway; cerebellar relay |
| Lesion syndrome | Benedikt syndrome (CN III + contralateral ataxia + hemiparesis) |
Sources: Guyton & Hall Textbook of Medical Physiology | Neuroscience: Exploring the Brain, 5e | Neuroanatomy through Clinical Cases, 3e | Localization in Clinical Neurology, 8e
Malignant hyperthermia
Finding Sources
Finding Sources
Searching PubMed
"malignant hyperthermia"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
This is rich. I now have everything needed for a comprehensive answer.
Malignant Hyperthermia (MH)
Definition
Malignant hyperthermia is a pharmacogenetic, life-threatening hypermetabolic syndrome of skeletal muscle triggered by volatile halogenated anesthetic agents and/or the depolarizing muscle relaxant succinylcholine in genetically susceptible individuals. Without prompt treatment, it is fatal. - Miller's Anesthesia, 10e, p. 4525
Epidemiology
| Parameter | Data |
|---|---|
| Incidence (fulminant MH) | 1:10,000 to 1:250,000 anesthetics |
| Prevalence of MH-susceptible mutations | ~1:2,000 in general population |
| Pediatric cases | 52.1% of all MH reactions |
| Sex | Males more susceptible than females |
| Mortality (historical) | 60-80% |
| Mortality (current, with dantrolene) | <1.4-5% |
- Miller's Anesthesia, 10e; Sabiston Textbook of Surgery
Pathophysiology
Normal Excitation-Contraction Coupling (ECC)
- Motor nerve impulse → acetylcholine release at NMJ
- ACh activates nicotinic receptors → action potential propagates along sarcolemma into T-tubules
- T-tubule depolarization is sensed by Cav1.1 (DHPR - dihydropyridine receptor), the L-type voltage-gated Ca²⁺ channel
- DHPR mechanically activates the RyR1 (ryanodine receptor type 1) on the sarcoplasmic reticulum (SR)
- RyR1 opens → Ca²⁺ floods from SR into myoplasm → muscle contraction
In MH - What Goes Wrong
In susceptible individuals, triggering agents (volatile agents / succinylcholine) cause:
- Uncontrolled, sustained opening of RyR1 → massive Ca²⁺ release from SR
- Persistently elevated myoplasmic Ca²⁺ drives skeletal muscle into a hypermetabolic state
- Rapid ATP consumption → heat generation, CO₂ production, O₂ consumption all surge
- Progressive muscle contracture → rhabdomyolysis
- Metabolic acidosis, hyperkalemia, hyperthermia ensue
This is a disease of excitation-contraction coupling dysregulation - not of central thermoregulation. - Miller's Anesthesia, 10e, p. 4529
Genetics
- Inheritance: Autosomal dominant with incomplete penetrance (many susceptible individuals never develop MH even with exposure)
- RYR1 gene (chromosome 19q13.2): >230 mutations identified; accounts for 50-80% of cases
- Encodes the type 1 ryanodine receptor (SR Ca²⁺ release channel)
- Classic porcine model: Arg615Cys missense mutation - all susceptible swine carry this identical mutation
- CACNA1S gene: 3 mutations identified; encodes the α1 subunit (pore-containing) of Cav1.1/DHPR
- At least 5 other loci have been identified
- Genetic heterogeneity means mutations vary between families; phenotype varies even within a single genotype due to sex, age, epigenetic, and environmental modifiers
Thompson & Thompson Genetics and Genomics, 9e; Bradley & Daroff's Neurology; Miller's Anesthesia
Triggering Agents
| Triggers MH | Safe (non-triggering) |
|---|---|
| All volatile halogenated agents: halothane, isoflurane, sevoflurane, desflurane | Propofol |
| Succinylcholine (depolarizing NMBA) | Non-depolarizing NMBAs (vecuronium, rocuronium, etc.) |
| Nitrous oxide | |
| IV agents (ketamine, barbiturates, benzodiazepines) | |
| Local anesthetics | |
| Opioids |
Clinical Features
MH can manifest at any point during general anesthesia or up to 60 minutes after cessation. Signs roughly progress from early metabolic to late catastrophic:
Early Signs
- ↑ End-tidal CO₂ despite increased minute ventilation - one of the earliest and most reliable signs
- Tachycardia
- Tachypnea / increased O₂ consumption
- Mixed metabolic and respiratory acidosis
Late / Fulminant Signs
- Masseter muscle rigidity (especially after succinylcholine) - may be the first sign
- Generalized muscle rigidity
- Hyperthermia - temperature can rise by 1°C every 5 minutes (a very late sign; do not wait for it)
- Rhabdomyolysis → myoglobinuria → acute kidney injury
- Hyperkalemia (from muscle breakdown) → life-threatening arrhythmias
- Extreme metabolic acidosis
- Disseminated intravascular coagulation (DIC) in severe cases
Key teaching point: Hyperthermia is a late sign - MH should be diagnosed and treated before temperature rises significantly. Early rising CO₂ and rigidity are the actionable clues.
Diagnosis
Intraoperative (clinical diagnosis)
Diagnosis is clinical - based on the constellation of signs above in the setting of volatile agent/succinylcholine exposure.
Laboratory findings
- ↑↑ Creatine kinase (CK) - markedly elevated
- Metabolic + respiratory acidosis (↓pH, ↑PaCO₂, ↑lactate)
- Hyperkalemia
- Myoglobinuria
- ↑ Temperature
Confirmatory Testing (after acute episode - for susceptibility testing)
- Caffeine-halothane contracture test (CHCT / IVCT): Gold standard
- Thin strip of explanted (biopsied) muscle stimulated electrically, then exposed to caffeine ± halothane
- Abnormally increased contracture = positive = MH-susceptible
- Highly operator-dependent; only done at specialized centers
- Genetic testing: RYR1/CACNA1S mutation analysis - positive in ~50-80% of confirmed cases
- 2025 European MH Group updated guidelines (Rüffert et al., Br J Anaesth 2026) provide the current framework for susceptibility investigation [PMID: 41478797]
Treatment - Emergency Protocol
Immediate actions (the "ABCDE" of MH crisis):
1. Stop the trigger
- Immediately discontinue all volatile agents and succinylcholine
- Switch to total IV anesthesia (propofol)
- Hyperventilate with 100% O₂ at high fresh gas flows
2. Dantrolene - the antidote
- Mechanism: Inhibits Ca²⁺ release from the SR by binding RyR1, directly counteracting the pathological process
- Dose: 2.5 mg/kg IV bolus immediately
- Re-dose: Every 10-15 minutes as needed for ongoing fever, acidosis, and rigidity
- Total dose: Up to 10 mg/kg or more may be required
- Continue dantrolene for 24-48 hours post-crisis to prevent recurrence
3. Active cooling
- Cooling blankets, ice packs to axilla/groin, cold IV saline
- Target temperature <38.5°C
- Stop cooling at ~38°C to avoid overshoot hypothermia
4. Supportive measures
| Problem | Treatment |
|---|---|
| Metabolic acidosis | Sodium bicarbonate |
| Hyperkalemia | Calcium, glucose/insulin, sodium bicarbonate |
| Arrhythmias | Standard antiarrhythmics (avoid calcium channel blockers - interact with dantrolene) |
| Myoglobinuria/AKI | IV fluid resuscitation, forced diuresis, monitor urine output |
| DIC | FFP, cryoprecipitate, platelets as needed |
5. ICU admission
-
Monitoring and observation in ICU are warranted after all MH episodes
-
Sabiston Textbook of Surgery; Bradley & Daroff's Neurology; Miller's Anesthesia, 10e
Preoperative Management of MH-Susceptible Patients
- Use total IV anesthesia (TIVA) - propofol-based
- Use non-depolarizing NMBAs only
- Pre-treat with oral dantrolene (controversial - most centers now use TIVA without routine prophylactic dantrolene, but have dantrolene immediately available)
- Have dantrolene drawn up and ready before induction
- Avoid volatile anesthetic machines unless thoroughly flushed (flush with O₂ for 20 min at high flow)
- Post-op monitoring for at least 4 hours
Related Conditions
| Condition | Relation to MH |
|---|---|
| Central core disease (CCD) | Caused by RYR1 mutations; ~50% have MH susceptibility |
| King-Denborough syndrome | Rare myopathy + MH susceptibility |
| Neuroleptic malignant syndrome (NMS) | Clinically similar (hyperthermia, rigidity) but triggered by antipsychotics/dopamine antagonists; treated with bromocriptine + dantrolene |
| Serotonin syndrome | Similar features; triggered by serotonergic agents |
| Porcine stress syndrome | Identical mechanism in pigs (Arg615Cys RyR1 mutation); triggered by any stress |
Historical Landmark
The modern era began in 1960 when Denborough et al. reported a 21-year-old Australian whose 10 relatives had died during anesthesia. Dantrolene was first shown effective in porcine MH in 1975 (Harrison) and rapidly confirmed in humans. Before dantrolene, mortality was 60-80%; today it is <5%. - Miller's Anesthesia, 10e
2025-2026 Guideline Updates
Two major practice guidelines were published in early 2026:
- JSA guideline for management of MH (2025) - Japanese Society of Anesthesiologists [PMID: 41504952]
- European MH Group 2025 guidelines for investigation of MH susceptibility - updated contracture testing and genetic testing protocols [PMID: 41478797]
Sources: Miller's Anesthesia, 10e | Sabiston Textbook of Surgery | Bradley & Daroff's Neurology in Clinical Practice | Thompson & Thompson Genetics & Genomics in Medicine, 9e | Emery's Elements of Medical Genetics
Hiccup treatment at home and hosp
Finding Sources
Finding Sources
Searching PubMed
"hiccup"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
I now have everything needed for a complete, well-organized answer.
Hiccup (Singultus) - Treatment at Home & Hospital
What Is a Hiccup?
A hiccup is an involuntary spasmodic contraction of the inspiratory muscles (primarily the diaphragm), followed 30-40 ms later by abrupt glottic closure - producing the characteristic sound. It has no known protective function.
Reflex arc: Afferent signals travel via the phrenic nerve, vagus nerve, and thoracic sympathetic chain. The reflex center is in the brainstem. Most triggers work by stimulating, inflaming, or injuring one of these nerves. - Tintinalli's Emergency Medicine
Classification by Duration
| Type | Duration | Significance |
|---|---|---|
| Benign / self-limited | < 48 hours | Usually no underlying disease |
| Persistent | 48 hours - 1 month | Often vagal/phrenic nerve irritation |
| Intractable | > 1 month | Usually organic cause; needs investigation |
Common Causes
| Acute / Benign | Persistent / Intractable |
|---|---|
| Gastric distension (food, carbonated drinks, air) | CNS structural lesions (brainstem infarct, tumor, MS) |
| Alcohol intoxication | Vagal or phrenic nerve irritation |
| Excessive smoking | Metabolic: uremia, hyperglycemia |
| Abrupt temperature change | General anesthesia / post-op |
| Psychogenic | Drugs: dexamethasone, chemotherapy agents |
| Foreign body in ear touching tympanic membrane | |
| Peritonitis involving diaphragmatic peritoneum | |
| Advanced renal failure |
Surgical pearl: In the early postoperative period, hiccups suggest upward diaphragmatic pressure from gastric distension or paralytic ileus - insert a nasogastric tube and aspirate. - S Das Manual on Clinical Surgery, 13e
Home Remedies (Physical Maneuvers)
These work by stimulating the pharynx to block the vagal arc or by increasing PaCO₂ to suppress the reflex centre. No single method is proven superior to another.
Vagal Stimulation Maneuvers
- Swallow a teaspoon of dry granulated sugar - as effective as most others, simple and safe
- Sip or quickly drink ice-cold water
- Breath-holding / Valsalva maneuver - increases intrathoracic pressure
- Breathing into a paper bag - raises CO₂, suppresses reflex
- Swallowing dry bread or crushed ice
- Pulling knees to chest and leaning forward (compresses diaphragm)
- Applying pressure to the eyeballs (stimulates vagus via oculocardiac reflex)
- Digital rectal massage - stimulates rectal branch of vagus (reported effective, rarely used at home)
- Gargling with water
- Tongue traction or pharyngeal stimulation
Ear
- Remove any foreign body from the external auditory canal - a hair touching the tympanic membrane stimulates the auricular branch of the vagus and is a treatable, often-missed cause
Diagnostic clue: If hiccups resolve during sleep, a psychogenic cause is more likely (though not absolute). - Tintinalli's Emergency Medicine, p. 471
Hospital Treatment
Step 1: Identify & Treat the Cause
- Check for foreign body in ear
- Chest X-ray for persistent hiccups
- Rule out: uremia, hyperglycemia, CNS lesion, drug-induced (steroids, chemotherapy)
- Postoperative hiccup → nasogastric tube insertion + aspiration
- Steroid-induced hiccup → reduce steroid dose
- Fluoroscopy (non-ED): assesses unilateral vs bilateral diaphragm movement (unilateral = focal phrenic nerve lesion)
Step 2: Drug Treatment
Chlorpromazine is the only FDA-approved drug for hiccups; all others are off-label.
| Drug | ED/Initial Dose | Maintenance (on discharge) | Notes |
|---|---|---|---|
| Chlorpromazine (FDA-approved) | 25-50 mg IV; repeat in 2-4 h | 25-50 mg PO 3-4×/day | First-line for intractable hiccups; dopamine D2 blocker |
| Metoclopramide | 10 mg IV or IM | 10-20 mg PO 3×/day for 10 days | Prokinetic; reduces gastric distension |
| Haloperidol | 2-5 mg IM | 2-4 mg PO 3×/day | Useful in palliative/cancer patients |
| Baclofen | 10 mg PO | 10 mg PO 3×/day, titrate up to 75 mg/day | GABA-B agonist; good for intractable/neurogenic hiccups |
| Gabapentin | 100 mg PO | 100 mg PO 3×/day, titrate up to 1200 mg/day | Useful in post-stroke and neurological hiccups |
| Nifedipine | 10-20 mg PO | 10-20 mg PO 3-4×/day | Calcium channel blocker; reduces diaphragm excitability |
| Valproic acid | 15 mg/kg PO | 15 mg/kg PO 3×/day | For refractory cases |
Source: Tintinalli's Emergency Medicine, Table 62-7
Other agents mentioned in literature:
- Phenothiazines (in addition to chlorpromazine)
- Pregabalin - similar to gabapentin; used in CNS-origin hiccups
- Ondansetron - occasionally used
- Pethidine (meperidine) - for postoperative hiccup (S Das Manual)
- In palliative care: midazolam infusion for refractory terminal hiccups
Step 3: Invasive Options (truly intractable cases)
- Phrenic nerve block - local anesthetic injection (temporary relief)
- Phrenic nerve crush/section - last resort; risks hemidiaphragm paralysis
- Nasogastric tube insertion + aspiration (for postoperative gastric distension)
- Acupuncture - a 2023 systematic review and meta-analysis found acupuncture effective for post-stroke hiccups (PMID: 37644765)
Quick Reference Summary
HICCUP
│
├─ < 48 hours → Home maneuvers (sugar, cold water, breath-holding, paper bag)
│
├─ 48 hrs - 1 month (Persistent) → Treat cause + Metoclopramide / Chlorpromazine
│
└─ > 1 month (Intractable) → Full workup + Baclofen / Gabapentin / Chlorpromazine IV
Consider phrenic nerve block if all else fails
Sources: Tintinalli's Emergency Medicine | S Das Manual on Clinical Surgery, 13e | Plum & Posner's Diagnosis and Treatment of Stupor and Coma | Sleisenger & Fordtran's GI and Liver Disease | Bradley & Daroff's Neurology
This is a shared conversation. Sign in to Orris to start your own chat.