Base excess
Reading File
Finding Sources
Finding Sources
Searching the Web
base excess definition physiology acid-base
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information to write a thorough, well-organized answer.
Base Excess (BE)
Definition
Base excess is the amount of strong acid (HCl) or strong base (NaOH) required to titrate 1 L of whole blood back to a pH of 7.40, at a standardized PaCO2 of 40 mmHg and temperature of 37°C. It is reported in mEq/L (mmol/L).
- Normal range: -2 to +2 mEq/L (some sources use -4 to +4 as the outer limit before labeling it "abnormal")
- Positive value → excess base present → metabolic alkalosis
- Negative value (base deficit) → deficit of base → metabolic acidosis
- Current Surgical Therapy 14e
Historical Background
The concept was developed through a series of key steps:
- 1948 - Singer & Hastings introduced the "buffer base" - the sum of HCO3⁻ and non-volatile buffer ions (albumin, phosphate, hemoglobin), representing total buffering capacity.
- Early 1950s - Astrup et al. (Copenhagen) developed the standard bicarbonate - [HCO3⁻] measured at 37°C and PaCO2 of 40 mmHg.
- Siggaard-Andersen & Astrup recognized that PaCO2 and [HCO3⁻] are not independent variables, and derived BE to separate respiratory from metabolic acid-base disturbances. This is the "Copenhagen approach."
- Miller's Anesthesia, 10e
Why Not Just Use Bicarbonate?
Bicarbonate (HCO3⁻) alone is problematic because it does not separate respiratory from metabolic contributions. When PaCO2 rises (respiratory acidosis), HCO3⁻ also rises secondarily due to CO2 hydration - giving a falsely elevated bicarbonate even with no metabolic change. BE corrects for this: in pure acute respiratory acidosis or alkalosis, BE = 0 (does not change), making it a cleaner measure of the metabolic component.
- Morgan & Mikhail's Clinical Anesthesiology, 7e
Standard Base Excess (SBE) - The Modern Formula
Modern blood gas analyzers report the Standard Base Excess (SBE) - also called the base excess of extracellular fluid - using this formula:
SBE = ([HCO3⁻]act − 24.8) + (16.2 × (pH − 7.40))
This corrects for some of the errors in Siggaard-Andersen's original assumptions about extracellular and intracellular buffering.
The underlying Van Slyke equation uses hemoglobin concentration (Hb accounts for ~53 mmol/L of the ~63 mmol/L non-bicarbonate buffer value in erythrocytes), which is why Hb is required in the calculation.
- Tietz Textbook of Laboratory Medicine, 7e; Miller's Anesthesia, 10e
Changes in SBE with Acid-Base Disturbances
| Disturbance | SBE Change |
|---|---|
| Acute respiratory acidosis | ΔBE = 0 |
| Acute respiratory alkalosis | ΔBE = 0 |
| Chronic respiratory acidosis | ΔBE = 0.4 × ΔPaCO2 |
| Metabolic acidosis | ΔPaCO2 = ΔBE (compensation) |
| Metabolic alkalosis | ΔPaCO2 = 0.6 × ΔBE (compensation) |
- Miller's Anesthesia, 10e (Table 44.3)
Copenhagen Nomogram
The acid-base nomogram below (Schlichtig's revision) allows classification of all disturbances from just two values - PaCO2 and SBE:
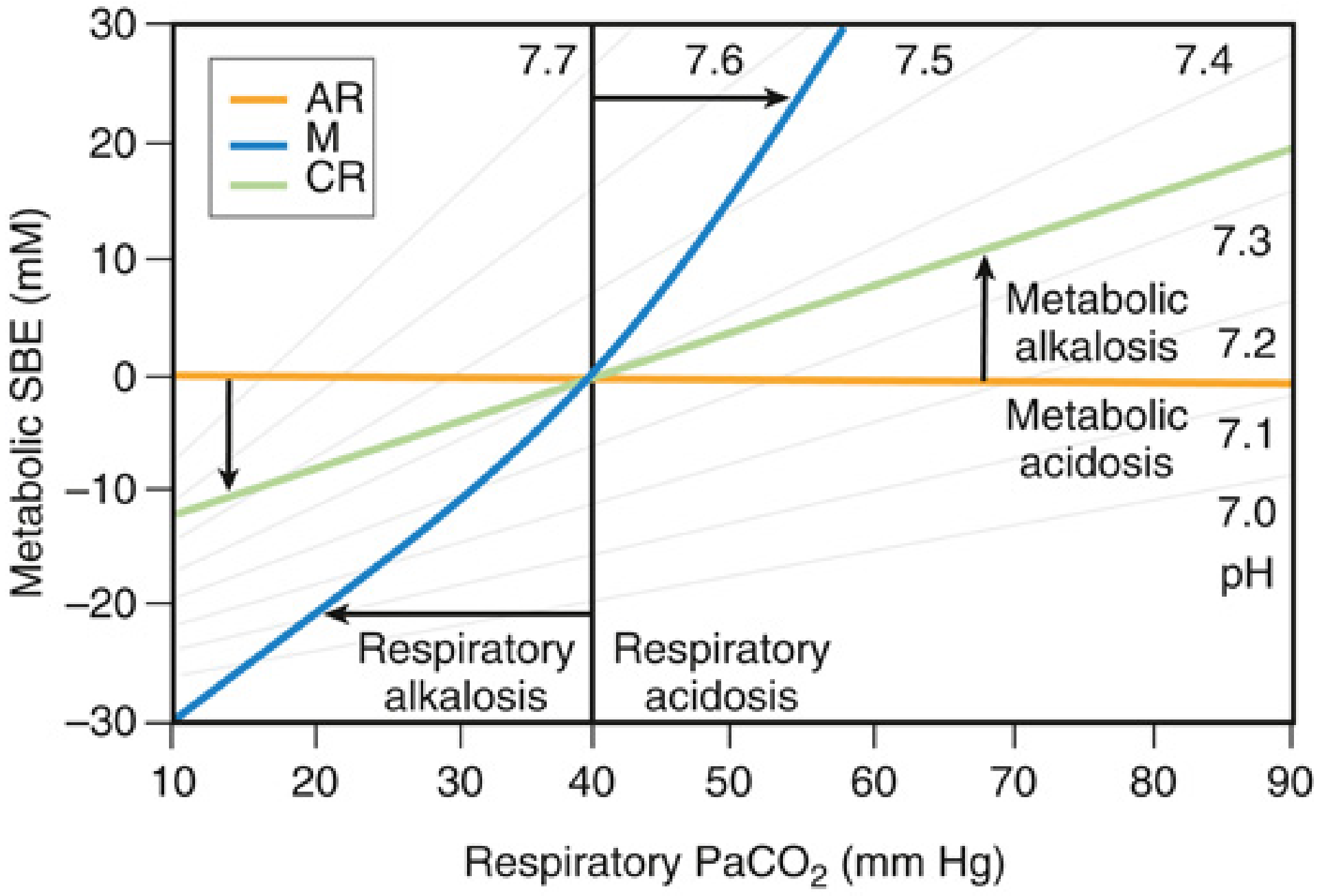
Key points from the nomogram:
- AR (orange line): Acute respiratory disturbances - SBE stays at zero regardless of PaCO2 change
- M (blue diagonal): Metabolic disturbances - SBE shifts vertically while PaCO2 compensates
- CR (green diagonal): Chronic respiratory disturbances - renal compensation raises SBE over days
- Miller's Anesthesia, 10e, Fig. 44.5
Base Excess Gap and the Fencl Approach
BE by itself cannot identify which metabolic process is responsible. The Base Deficit Gap (BDG) / Fencl approach decomposes the total BE into its contributing components:
| Component | Formula |
|---|---|
| Na/water effect (BE_NaW) | 0.3 × ([Na⁺]measured − 140) |
| Chloride effect (BE_Cl) | 105 − [Cl⁻]effective |
| Albumin effect (BE_prot) | (42 − [Albumin] g/L) × (0.148 × pH − 0.818) |
| Calculated BE (BE_calc) | Sum of above |
| BE Gap | BE_calc − BE_actual − [lactate] |
The BE Gap mirrors the strong ion gap (SIG) and the corrected anion gap, identifying unmeasured anions (e.g. from acute kidney injury or toxins) once lactate and ketoacidosis are excluded.
This approach can identify:
- Contraction alkalosis
- Hypoalbuminemic alkalosis
- Hyperchloremic acidosis
- Organic anion acidosis (lactate, ketones)
- Unmeasured anion acidosis
- Miller's Anesthesia, 10e (Boxes 44.4, 44.5)
Limitations
- BE is closely linked to HCO3⁻ and both are derived from the Henderson-Hasselbalch equation - so they convey similar information.
- Both approaches can be misleading in mixed disorders. A critically ill patient with concurrent hypoalbuminemia (metabolic alkalosis) and lactic acidosis (metabolic acidosis) may show a normal pH, HCO3⁻, and BE - masking both abnormalities.
- Neither BE nor HCO3⁻ alone distinguishes why there is a metabolic disturbance (chloride vs. lactate vs. dehydration) - this requires the BE gap / anion gap analysis.
- Miller's Anesthesia, 10e
ABG Interpretation: Where BE Fits In
Step-by-step ABG interpretation (from Current Surgical Therapy 14e):
- pH - < 7.35 = acidemia; > 7.45 = alkalemia
- PaCO2 - assesses respiratory component
- HCO3⁻ - assesses metabolic component
- Base excess - confirms metabolic contribution; abnormal if > +4 or < -4
- PO2 - assess oxygenation and its role in driving acid-base changes
Normal ABG values for reference:
| Variable | Normal | Range |
|---|---|---|
| pH | 7.40 | 7.35-7.45 |
| PaCO2 | 40 mmHg | 38-42 mmHg |
| HCO3⁻ | 24 mEq/L | 22-26 mEq/L |
| Base Excess | 0 | -2 to +2 mEq/L |
This is a shared conversation. Sign in to Orris to start your own chat.