Tell me how to disgnoee bowel conditions, like how to differentiate one from other
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the information needed for a thorough, well-illustrated answer. Let me compile the full response.
Diagnosing and Differentiating Bowel Conditions
Bowel conditions span a wide spectrum - from functional disorders like IBS, to structural inflammatory diseases (Crohn's, UC), to infectious colitis, ischemia, and malignancy. The key to diagnosis is combining clinical features, lab markers, endoscopy, histology, and imaging in a systematic way.
1. The Major Bowel Conditions to Differentiate
| Condition | Key Feature |
|---|---|
| Crohn's Disease (CD) | Transmural, patchy, any GI segment |
| Ulcerative Colitis (UC) | Mucosal only, continuous, colon only |
| Irritable Bowel Syndrome (IBS) | Functional, no structural disease |
| Infectious Colitis | Acute onset, stool culture positive |
| Ischemic Colitis | Vascular, watershed areas |
| Microscopic Colitis | Watery diarrhea, normal endoscopy |
| Colorectal Cancer | Mass, obstruction, weight loss |
2. Crohn's Disease vs. Ulcerative Colitis - The Core Differentiation
This is the most clinically important distinction.
Clinical Features Compared
| Feature | Crohn Disease | Ulcerative Colitis |
|---|---|---|
| Peak age of onset | 15-30 yrs (2nd peak in 7th decade) | 20-40 yrs (smaller 2nd peak after 7th decade) |
| Sex | F slightly > M (1.2:1) | Equal (1:1) |
| GI sites involved | Esophagus to anus (mouth-to-anus) | Colon only |
| Pattern of involvement | Patchy, "skip" lesions | Continuous, no skip areas |
| Transmural inflammation | Yes | No (mucosal/submucosal only) |
| Type of ulceration | Discrete | Continuous |
| Rectal involvement | Usually spared | Almost always involved (disease spreads proximally from rectum) |
| Ileal involvement | Present in ~70% | Only "backwash ileitis" in severe pancolitis |
| Fistula formation | Common (20-40%) - perianal, enterocutaneous, rectovaginal, enterovesicular | Rare |
| Strictures | Common | Rare (when present, biopsy to exclude malignancy) |
| Perianal disease | Prominent - skin tags, fissures, complex fistulas, abscesses | Rare |
(Sources: Goldman-Cecil Medicine, Table 127-1; Maingot's Abdominal Operations, Table 34-2)
3. Symptoms Side by Side
Crohn's Disease
- Right lower quadrant pain (terminal ileum in ~70%)
- Diarrhea (with or without blood)
- Weight loss, fever, fatigue
- Can mimic acute appendicitis
- Obstructive symptoms if strictures develop
- Perianal discharge/pain
- Vitamin B12 deficiency (ileal disease)
- Calcium oxalate kidney stones (fat malabsorption binds calcium, leaving oxalate unbound)
- Polymicrobial UTIs (enterovesicular fistula)
Ulcerative Colitis
- Hematochezia (almost universal - blood and mucus per rectum)
- Diarrhea, tenesmus, urgency
- Abdominal pain (often left-sided or diffuse)
- In proctitis: paradoxical constipation (difficulty defecating despite urgency)
- Fever and weight loss in severe/extensive disease
- Anemia, hypoalbuminemia in severe cases
(Goldman-Cecil Medicine, pp. 1481-1482)
4. Endoscopic Appearance
Crohn's Disease
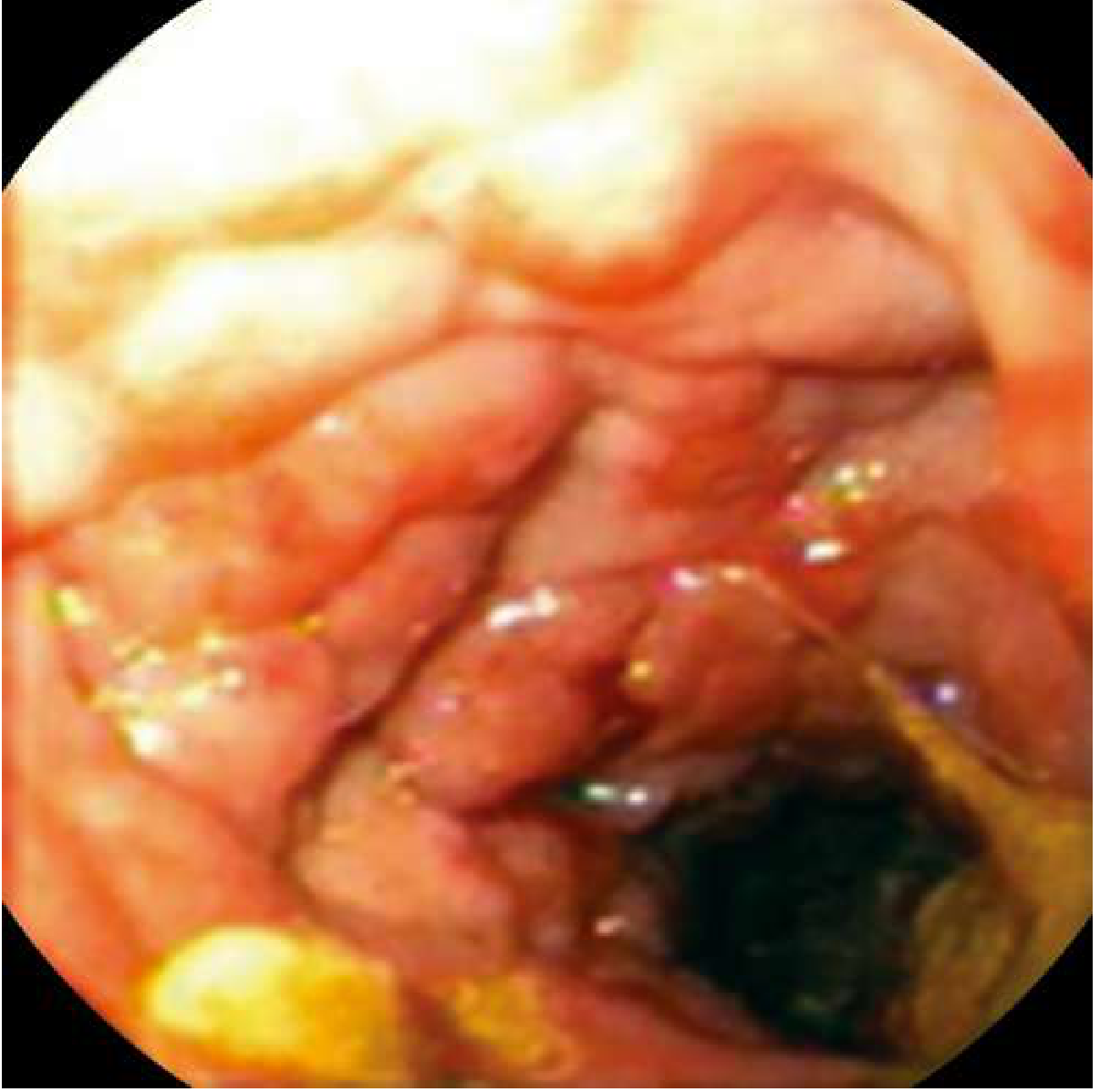
Early: aphthous ulcers. With progression: stellate ulcers, serpiginous "bear claw" ulcers, then classic cobblestoning (normal mucosa elevated between intersecting longitudinal + transverse ulcers). Skip areas of normal-looking mucosa between inflamed patches are characteristic.
Ulcerative Colitis
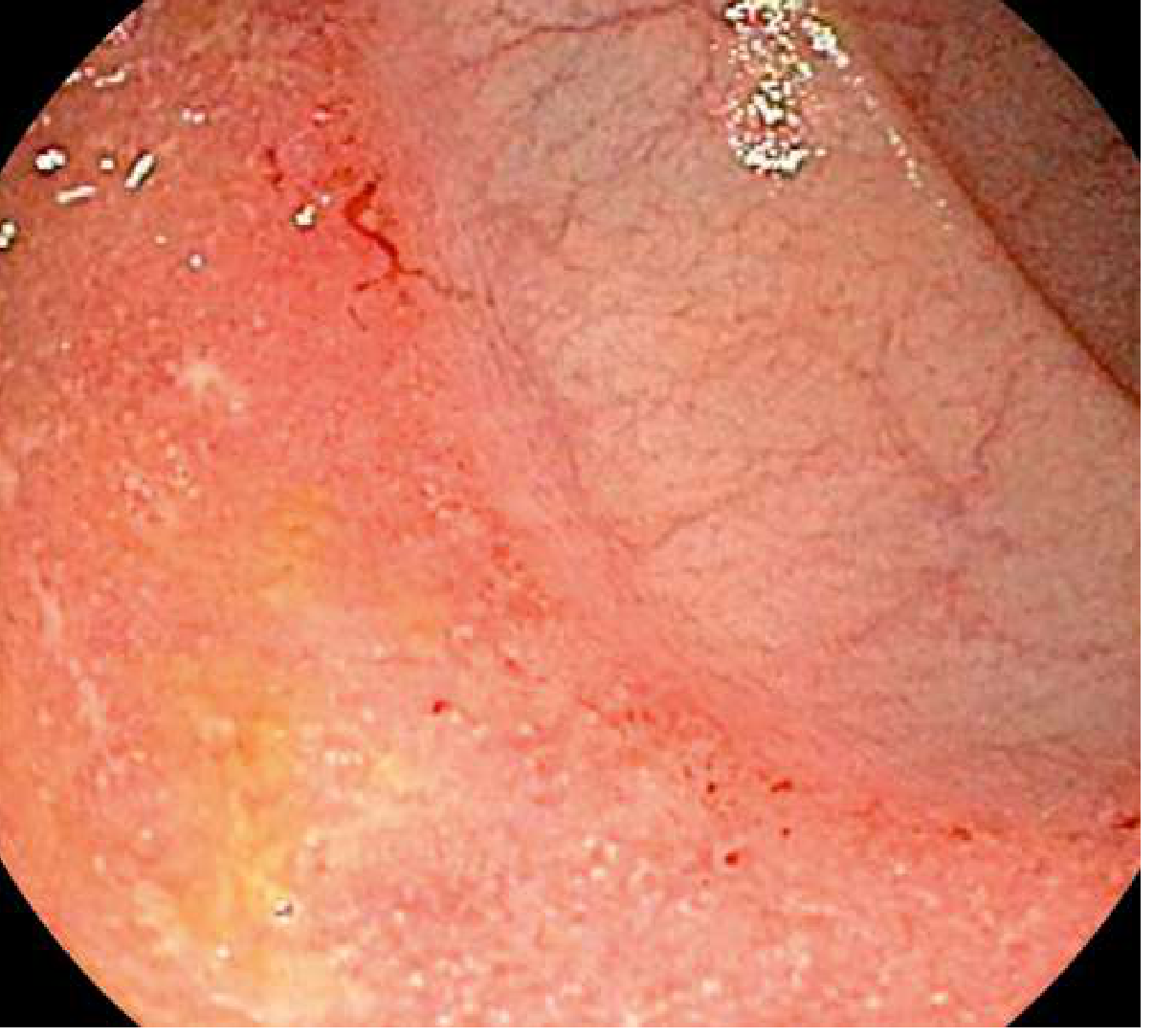
Loss of normal vascular markings, diffuse granular/friable mucosa, continuous involvement from rectum extending proximally. Large ulcers can be surrounded by inflamed mucosa and pseudopolyps in severe disease.
5. Histopathology (Biopsy)
| Feature | Crohn's Disease | Ulcerative Colitis |
|---|---|---|
| Depth | Transmural | Mucosal/submucosal |
| Granulomas | Noncaseating granulomas (pathognomonic if present) | Absent |
| Crypt changes | Distortion | Crypt distortion + lymphocytic infiltration |
Noncaseating granulomas alone are diagnostic of Crohn's. In the absence of granulomas, the full clinical picture is needed. - Goldman-Cecil Medicine, p. 1482
6. Serological Markers
When endoscopy/biopsy is equivocal (especially in Crohn's confined to the colon):
| Marker | Crohn's | UC |
|---|---|---|
| pANCA (atypical perinuclear ANCA) | ~20% positive | ~70% positive |
| ASCA (anti-Saccharomyces cerevisiae antibody - IgG/IgA) | 60-70% positive | ~10-15% positive |
- pANCA+/ASCA- combination = specific for UC
- pANCA-/ASCA+ combination = specific for Crohn's
- Combined specificity >90%, but sensitivity only ~50%, so useful as supplementary test, not primary diagnosis.
(Maingot's Abdominal Operations)
7. Imaging
- CT/MRI enterography: Best for assessing small bowel extent in Crohn's, detecting transmural complications (abscesses, fistulas, strictures)
- Colonoscopy with terminal ileum intubation: First-line for lower GI symptoms when IBD is suspected
- Capsule endoscopy: Used when Crohn's is still suspected after all other testing is negative - do not use if a stricture is present (use a patency capsule first)
- Small bowel follow-through: Can map strictures and fistulas in Crohn's
8. Differentiating IBS from Organic Bowel Disease
IBS is a functional disorder - no structural, inflammatory, or biochemical abnormality. It is diagnosed by positive symptom criteria after excluding organic pathology.
Rome IV Diagnostic Criteria for IBS
Recurrent abdominal pain at least 1 day per week (on average in the last 3 months, with onset at least 6 months ago), associated with two or more of:
- Related to defecation
- Associated with a change in stool frequency
- Associated with a change in stool form/appearance
IBS Subtypes
- IBS-C: Predominant constipation
- IBS-D: Predominant diarrhea
- IBS-M: Mixed bowel habits
- IBS-U: Unclassified
The IBS Diagnostic Algorithm
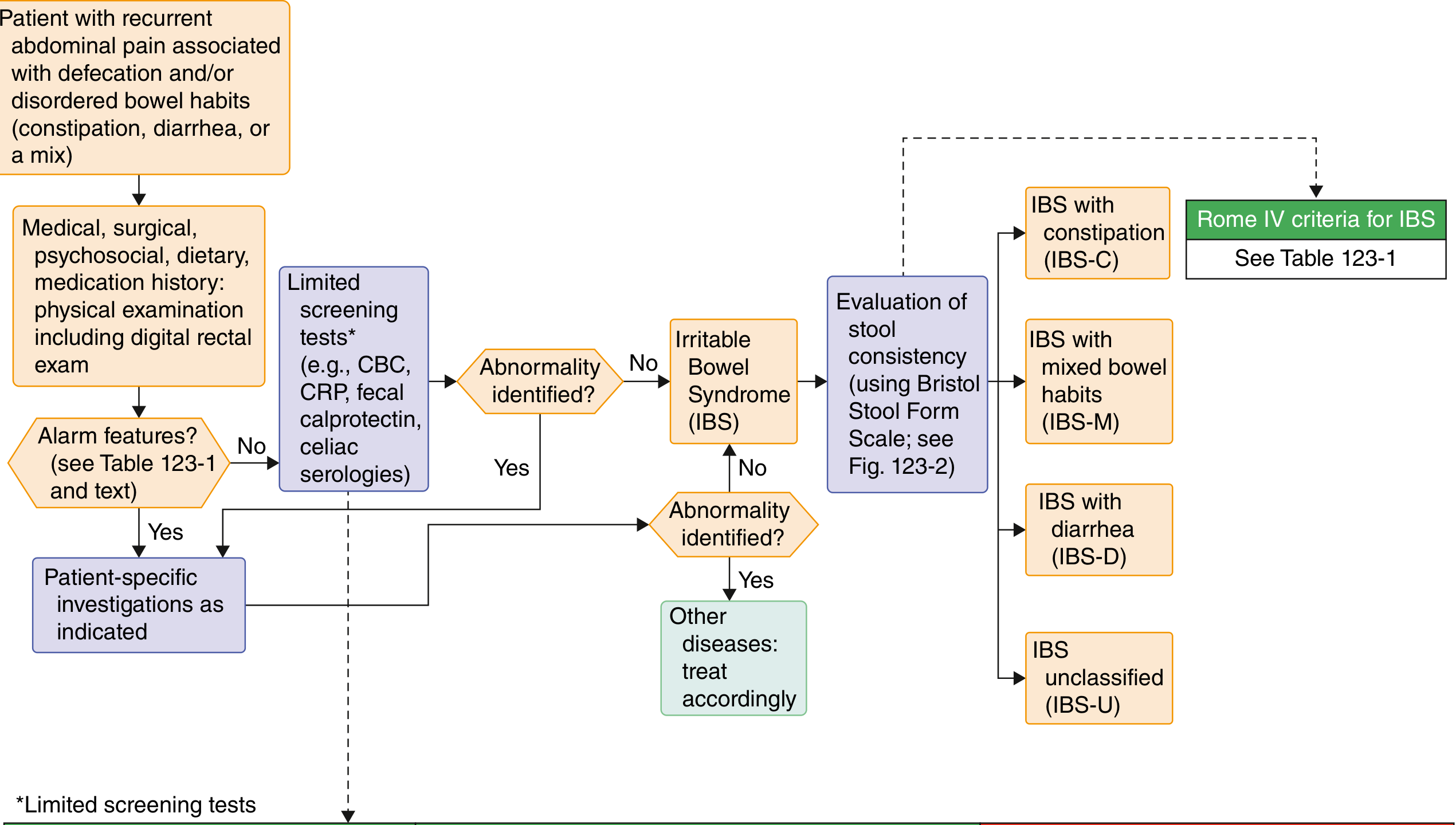
(Goldman-Cecil Medicine, Fig. 123-1)
Alarm Features That EXCLUDE IBS (require further workup)
- New onset at age ≥50 years
- Unintentional weight loss
- Hematochezia or melena (not from hemorrhoids)
- Nocturnal diarrhea (wakes patient from sleep)
- Anemia
- Palpable abdominal mass or lymphadenopathy
- Family history of CRC, IBD, or celiac disease
Key tests in IBS workup:
- CBC, CRP (if elevated, IBD more likely than IBS)
- Fecal calprotectin/lactoferrin - elevated in IBD, normal in IBS (very useful non-invasive discriminator)
- Celiac serologies in IBS-D
- Colonoscopy only if alarm features or age ≥45
9. Infectious vs. Inflammatory Colitis
Infections can look identical to IBD on endoscopy. Always obtain stool cultures, PCR panels, or O&P before assuming IBD.
Key organisms mimicking IBD:
- Bacterial: Salmonella, Shigella, Campylobacter, C. difficile, E. coli O157:H7, Yersinia (can mimic Crohn's with RLQ pain)
- Viral: CMV (especially in immunocompromised)
- Parasitic: Entamoeba histolytica
Yersinia infection deserves special mention - it causes terminal ileitis and mesenteric adenitis that mimics Crohn's disease almost perfectly.
10. Extraintestinal Manifestations (useful clues)
Both CD and UC share several extraintestinal features, but some differ:
| Manifestation | CD | UC |
|---|---|---|
| Oral ulcers (aphthae) | Yes | No |
| Erythema nodosum | Yes | Yes |
| Pyoderma gangrenosum | Yes | Yes |
| Arthropathy | Yes | Yes |
| Ocular (uveitis, episcleritis) | Yes | Yes |
| Primary sclerosing cholangitis | Less common | Strongly associated (70-80% of PSC patients have UC) |
| Nephrolithiasis (oxalate stones) | Yes (small bowel disease) | Yes (but different mechanism) |
(Goldman-Cecil Medicine, Table 127-2)
Quick Decision Framework
Patient with chronic diarrhea / abdominal pain?
│
├── Alarm features (blood, weight loss, nocturnal sx, age >50)?
│ ├── YES → Colonoscopy + biopsy, imaging, stool culture
│ │ Likely IBD, ischemia, infection, or malignancy
│ └── NO → Screen with CBC, CRP, fecal calprotectin, celiac Ab
│ CRP/calprotectin normal? → Consider IBS (apply Rome IV)
│ CRP/calprotectin elevated? → Colonoscopy for IBD
│
├── Endoscopy: Cobblestoning, skip lesions, aphthous ulcers, perianal disease?
│ → Crohn's Disease (confirm with transmural biopsy/granulomas)
│
├── Endoscopy: Continuous mucosal inflammation from rectum upward?
│ → Ulcerative Colitis (confirm with crypt distortion on biopsy)
│
└── Normal endoscopy with watery diarrhea?
→ Biopsy anyway: Microscopic colitis (collagenous/lymphocytic)
The combination of clinical pattern, endoscopic appearance, histopathology, and serological markers (pANCA/ASCA) allows accurate differentiation in the vast majority of cases. In ~10-15% of cases with colonic-only IBD, definitive CD vs UC differentiation remains impossible and the label "IBD-unclassified" (IBD-U) is applied.
This is a shared conversation. Sign in to Orris to start your own chat.