Physiology of swallowing. Ms ent University exam pattern for 20 marks.
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have all the content needed for a thorough 20-mark MS ENT university exam answer. Let me compile it.
Physiology of Swallowing (Deglutition)
MS ENT University Exam - 20 Marks
Introduction
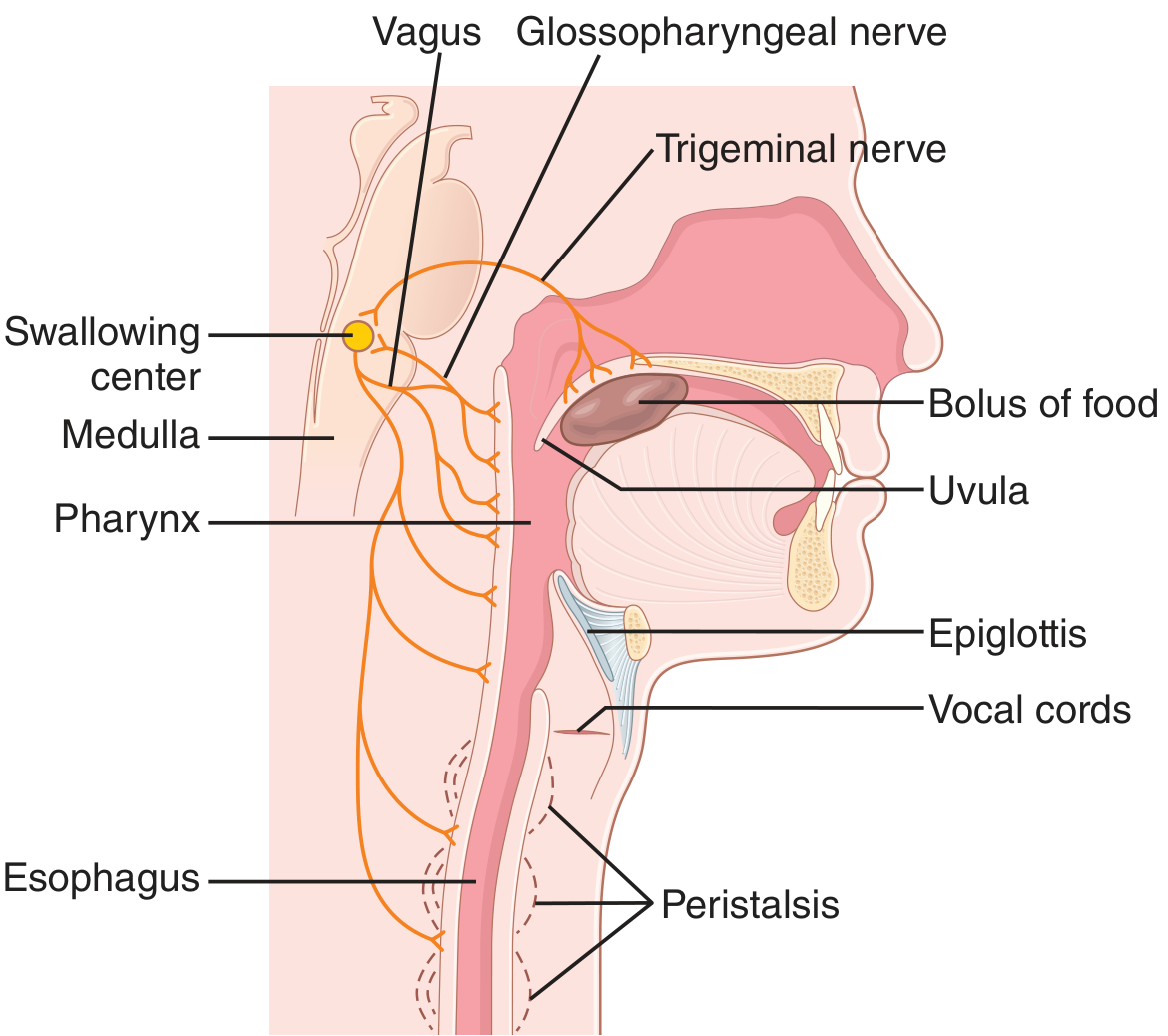
Swallowing (deglutition) is one of the most complex neuromuscular functions in living beings. It involves over 30 muscles coordinated by the CNS and peripheral nervous system. The laryngopharynx serves as a "time-share" for respiration and deglutition - the fundamental challenge is moving a bolus completely through the pharynx while the glottis is closed, requiring momentary interruption of respiration.
Swallowing is classically divided into three phases:
- Oral Phase (voluntary)
- Pharyngeal Phase (involuntary reflex)
- Esophageal Phase (involuntary)
(Guyton & Hall Medical Physiology; KJ Lee's Essential Otolaryngology)
Phase 1: Oral Phase (Voluntary)
Function: Prepares and delivers the food bolus to the pharynx.
The oral phase has two sub-stages:
a) Oral Preparatory Sub-stage:
- Mastication of food with addition and mixing of saliva
- Bolus formation and control by lips, tongue, buccinator muscle, and palate
- Selection and verification of bolus safety (volume, texture, foreign bodies)
- Sensory input via mechanoreceptors (touch, pressure), proprioceptors, chemoreceptors, and taste/temperature receptors in tongue, teeth, soft palate, and hard palate
- Mechanoreceptors in the tongue and palate modulate muscles of mastication through brain-stem integrative pathways
b) Oral Transit Sub-stage:
- The bolus is "voluntarily" squeezed or rolled posteriorly into the pharynx by upward and backward pressure of the tongue against the palate
- The oral phase ends when the bolus is pressed against the faucial arches - pressure-sensitive receptors on the anterior tonsillar pillar (CN IX and X) trigger the next involuntary phase
- Duration: variable (under voluntary control, can be prolonged)
(KJ Lee's Essential Otolaryngology, p. 672; Guyton & Hall, p. 788)
Phase 2: Pharyngeal Phase (Involuntary Reflex)
Function: Moves the bolus quickly (under 1 second) past the closed glottis through the UES into the esophagus.
This is entirely reflex and involves the following sequential events:
2a. Nasopharyngeal Closure
- Soft palate elevates (levator and tensor veli palatini muscles)
- Passavant's ridge forms by contraction of the superior pharyngeal constrictor
- Prevents bolus regurgitation into the nasopharynx/nasal cavity
2b. Palatopharyngeal Fold Approximation
- The palatopharyngeal folds on each side are pulled medially to form a sagittal slit
- Acts as a selective gate - only adequately masticated food passes; large objects are impeded
- Entire stage lasts less than 1 second
2c. Cessation of Respiration
- Respiration is inhibited, usually occurring during the expiratory phase
- The swallowing center in the medulla directly inhibits the respiratory center
- The entire pharyngeal stage lasts less than 6 seconds - interrupting respiration for only a fraction of the respiratory cycle
2d. Glottic Closure (Airway Protection - Multi-level)
- Sequence (in order): True vocal cords adduct first → false vocal cords close → arytenoids approximate against the epiglottis
- Adduction of the lateral cricoarytenoid muscles approximates the arytenoids
- Vocal fold adduction during swallowing averages approximately 2.3 seconds
- This is the most critical protective mechanism - destruction of vocal cord adductor function markedly increases aspiration risk
2e. Laryngeal Elevation and Epiglottic Retroflexion
- Suprahyoid muscles and the thyrohyoid muscle contract, pulling the hyolaryngeal complex superiorly and anteriorly
- Laryngeal elevation serves three functions:
- Protects the laryngeal vestibule from aspiration
- Causes epiglottic retroflexion (tilting backward over the laryngeal inlet)
- Actively dilates the upper esophageal sphincter (UES/cricopharyngeus)
- Epiglottic retroflexion: partly active (due to laryngeal elevation, pharyngeal constriction, tongue base retraction) and partly passive (pressure from the bolus itself)
- The epiglottis diverts food laterally into the pyriform sinuses (piriform fossae)
- Note: The epiglottis is NOT absolutely essential for airway protection - functional swallowing has been documented even with an absent epiglottis
2f. Bolus Propulsion
- Tongue base protrusion provides the primary "tongue driving force"
- Sequential contraction of pharyngeal constrictors from top to bottom (superior → middle → inferior) generates peristaltic propulsion
- The bolus passes through the now-open UES into the esophagus
2g. UES (Cricopharyngeal Sphincter) Opening
Three factors work together:
- Relaxation of cricopharyngeus muscle - precedes bolus arrival (neurally mediated)
- Active dilation - contraction of suprahyoid and thyrohyoid muscles pulls the hyolaryngeal complex forward, mechanically opening the sphincter (most important component)
- Pressure of descending bolus - assists opening from above
Between swallows, the UES remains strongly contracted, preventing air entry into the esophagus during respiration.
(KJ Lee's Essential Otolaryngology, p. 672-673; Guyton & Hall, p. 788-789; Scott-Brown's Otorhinolaryngology, p. 944)
Phase 3: Esophageal Phase (Involuntary)
Function: Conveys the bolus to the stomach, taking an average of 3 to 6 seconds (upright position) via peristalsis.
Two Types of Peristalsis:
Primary Peristalsis:
- Direct continuation of the peristaltic wave that began in the pharynx
- Passes from the pharynx to the stomach in approximately 8 to 10 seconds
- In the upright position, gravity assists, delivering the bolus in 5 to 8 seconds
Secondary Peristalsis:
- Triggered when the primary wave fails to clear all retained food
- Initiated by esophageal distension from the retained bolus
- Mediated by: (a) intrinsic myenteric nervous system circuits, and (b) reflexes from the pharynx transmitted via vagal afferent fibers to the medulla, then back through glossopharyngeal and vagal efferents
Muscle Types and Innervation:
- Upper 1/3 of esophagus (pharyngeal wall included): striated muscle - controlled by CN IX and X (skeletal nerve impulses)
- Lower 2/3 of esophagus: smooth muscle - controlled by the vagus nerve via the myenteric (Auerbach's) plexus
- Even after vagotomy, the myenteric plexus can maintain secondary peristalsis
Lower Esophageal Sphincter (LES / Gastroesophageal Sphincter):
- Located in the lower ~3 cm of esophagus
- Normally tonically constricted at approximately 30 mmHg intraluminal pressure
- As a peristaltic wave approaches, "receptive relaxation" occurs ahead of it (via myenteric inhibitory neurons), allowing easy passage of bolus into the stomach
- Prevents gastroesophageal reflux (failure = achalasia if incomplete relaxation, or GERD if inadequate tone)
(Guyton & Hall, p. 789-790; KJ Lee's Essential Otolaryngology, p. 672)
Neural Control of Swallowing
Swallowing Center
- Located in the medulla oblongata and lower pons (reticular formation)
- Key nuclei: Nucleus ambiguus (CN IX, X), dorsal motor nucleus of vagus (CN X), tractus solitarius (receives all sensory input from mouth/pharynx)
- Coordinates the entire sequential swallowing pattern
- Modulated by the cerebral cortex (which is why voluntary suppression or modification of swallowing is possible)
- Directly inhibits the respiratory center during the pharyngeal phase
Sensory Afferent Pathway:
- Trigger zone: Ring around the pharyngeal opening, with greatest sensitivity at the tonsillar pillars (anterior faucial pillar)
- Sensory receptors also on: soft palate, tongue base, posterior pharyngeal wall
- Central ganglia:
- CN V - Gasserian ganglion
- CN IX - Inferior (Andersch) and superior (Ehrenritter) ganglia
- CN X - Inferior (jugular) and superior (nodose) ganglia
- Impulses travel via CN V (trigeminal) and CN IX (glossopharyngeal) → tractus solitarius in medulla
Motor Efferent Pathway:
| Cranial Nerve | Structures Innervated |
|---|---|
| CN V | Teeth, jaw, masticators, mylohyoid, tensor veli palatini, anterior belly of digastric |
| CN VII | Lips, facial musculature, stylohyoid, posterior belly of digastric |
| CN IX | Pharynx (stylopharyngeus) |
| CN X | Pharynx (levator veli palatini, palatopharyngeus, salpingopharyngeus, pharyngeal constrictors, cricopharyngeus), larynx, esophagus |
| CN XII | All tongue muscles |
| Superior cervical nerves | Also contribute |
(KJ Lee's Essential Otolaryngology, p. 673; Guyton & Hall, p. 789; Cummings Otolaryngology)
Summary Table
| Phase | Control | Duration | Key Events |
|---|---|---|---|
| Oral | Voluntary | Variable | Mastication, bolus formation, tongue propulsion |
| Pharyngeal | Involuntary reflex | < 1 second | Nasopharyngeal closure, glottic closure, laryngeal elevation, epiglottic retroflexion, UES opening |
| Esophageal | Involuntary (ANS + myenteric) | 3-10 seconds | Primary + secondary peristalsis, LES relaxation |
Clinically Relevant Points (for exam scoring)
- Aspiration risk increases when laryngeal elevation is impaired - cricopharyngeal opening is limited, pressure drop during deglutition is slower, and the transient negative pressure in the cricopharyngeal sphincter does not occur (Scott-Brown's, p. 944)
- Achalasia: failure of LES to relax - food accumulates in esophagus
- Laryngeal penetration (barium above true vocal cords) can occur in healthy individuals; aspiration is defined as material passing below the true vocal cords into the trachea
- The epiglottis is NOT essential for airway protection in all cases - patients without an epiglottis can swallow safely
- FEES (Fiberoptic Endoscopic Evaluation of Swallowing) and Modified Barium Swallow are the principal investigations for dysphagia
Sources:
- Guyton & Hall Textbook of Medical Physiology (p. 788-790)
- KJ Lee's Essential Otolaryngology (p. 672-673)
- Cummings Otolaryngology Head and Neck Surgery
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (p. 944)
Stroboscopy in ent. Ms ent University exam pattern for 10 marks.
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have excellent, comprehensive content. Let me compile the full 10-mark answer.
Stroboscopy in ENT (Laryngeal Stroboscopy / Videostroboscopy)
MS ENT University Exam - 10 Marks
Definition and Principle
Stroboscopy is a lighting technique that uses a flashing light source to create an apparent slow-motion or "frozen" visualization of vocal fold vibration. Since the vocal folds vibrate at 100-1000+ cycles per second (Hz) during phonation - far exceeding the 16 frames/second limit of the human eye (Talbot's law) - direct continuous illumination cannot resolve individual vibratory movements.
Principle (Talbot's Law / Phi Phenomenon):
The strobe light flashes at a frequency slightly different from the fundamental frequency (F0) of vocal fold vibration. By illuminating the vocal folds at successively different phases of consecutive vibratory cycles, it produces a composite "sampling" of vibration that appears as slow-motion movement to the observer. When the strobe flashes at exactly the same frequency as F0 ("stop/locked mode"), the vocal folds appear completely stationary - frozen at one phase of the cycle.
(Cummings Otolaryngology Head and Neck Surgery; KJ Lee's Essential Otolaryngology)
Equipment
A complete videostroboscopy system consists of:
- Strobe light source - synchronized to the patient's F0 (detected via a microphone or contact sensor at the neck)
- Rigid 70° or 90° telescope (oropharyngeal) - gives higher image quality, preferred for most adults
- Flexible nasopharyngoscope - used when the rigid scope cannot be tolerated, or for connected speech evaluation
- Video camera and monitor - for real-time visualization and recording
- Microphone/frequency detector - picks up the patient's F0 to synchronize the strobe
Limitation: If vocal fold vibration is severely irregular (highly aperiodic), stroboscopy cannot function - the strobe cannot lock onto a consistent F0, and the image blurs or "quivers" rather than yielding slow-motion. In such cases, high-speed laryngeal videoendoscopy is the preferred alternative.
Vocal Fold Anatomy Relevant to Stroboscopy (Body-Cover Model)
Understanding the body-cover model is essential for interpreting stroboscopic findings:
| Layer | Components | Properties |
|---|---|---|
| Cover | Epithelium + superficial lamina propria (Reinke's space) | Pliable, loose |
| Transition | Intermediate + deep lamina propria | Stiffening layer |
| Body | Thyroarytenoid muscle | Stiff, contractile |
The mucosal wave travels from the inferior to the superior surface of the vocal fold (a wave propagating from the subglottis upward and laterally). It depends entirely on the pliability of the cover - the superficial lamina propria. Stroboscopy is the only clinical tool that can directly visualize this mucosal wave.
Parameters Assessed on Stroboscopy
The following parameters are systematically evaluated (standardized checklist):
1. Symmetry
- Refers to whether both vocal folds mirror each other in their movements
- Asymmetry suggests a difference in mass, tension, or innervation between the two folds
- Unilateral lesions, paresis, or scar characteristically produce asymmetric vibration
2. Regularity (Periodicity)
- Describes how consistent the cycle-to-cycle vibration is
- In stop mode: regular vibration = image appears static; irregular vibration = image quivers
- Irregularity suggests: paresis, neuromuscular disease (e.g., spasmodic dysphonia), stiff lesions (cyst, carcinoma), or edematous lesions
3. Glottal Closure Pattern
- Describes the degree and shape of vocal fold contact at the most closed instant
- Assessed at most comfortable pitch and loudness (MCPL)
- Closure patterns:
- Complete closure - normal in men
- Posterior gap - most common normal pattern in women
- Anterior gap / Spindle-shaped gap - normal variant in older adults; also seen in scar, sulcus vocalis, atrophy
- Hourglass gap - characteristic of bilateral vocal nodules or unilateral lesion with contralateral reactive change
- Incomplete closure (full length) - vocal fold paralysis, scar, severe atrophy
4. Amplitude of Vibration
- Lateral excursion of the vocal fold from midline during the open phase
- Reduced amplitude: suggests stiffness (scar, malignancy, post-radiation change)
- Exaggerated amplitude: seen in flaccid paralysis or edema (Reinke's edema)
5. Mucosal Wave
- The traveling wave that propagates from the inferior to superior surface during each vibratory cycle - a direct marker of cover pliability
- Absent or reduced mucosal wave = stiff cover (scar, post-surgical fibrosis, carcinoma, sulcus vocalis, radiation changes)
- Normal mucosal wave essentially rules out deep invasion by carcinoma
- This is the single most diagnostically useful stroboscopic parameter
6. Adynamic Segments
- Portions of the vocal fold that fail to vibrate while adjacent areas vibrate normally
- Indicates focal stiffness - very suspicious for submucosal lesion, cyst, scar, or carcinoma
7. Phase Closure (Open Quotient)
- Refers to the proportion of each vibratory cycle during which the glottis is open
- Normal: glottis is open for approximately two-thirds of one cycle at MCPL
- Closed phase generally decreases with higher pitch
8. Vertical Closure Level
- Normal: both vocal folds meet at the same horizontal plane
- Abnormal vertical level difference: suggests vocal fold paralysis or arytenoid dislocation
9. Vocal Fold Edges
- Shape of the free edge of the vocal fold
- Straight, smooth edge = normal
- Irregular, notched, or bowed edges suggest sulcus, scar, or prior phonosurgery
Clinical Applications / Indications
- Dysphonia evaluation - the single most important investigation for any persistent voice change
- Differentiation of benign lesions - vocal nodules vs. polyps vs. cysts vs. sulcus vocalis (all have characteristic patterns)
- Assessment of vocal fold paralysis/paresis - asymmetric mucosal wave, abnormal closure, adynamic segments
- Mucosal pliability assessment - distinguishing superficial mucosal disease from deep/submucosal lesion
- Suspected early carcinoma - absent or markedly reduced mucosal wave suggests submucosal invasion, prompting biopsy
- Pre- and post-phonosurgery assessment - baseline documentation and monitoring of tissue healing
- Professional voice users - identify subtle lesions before the voice complaint becomes severe
- Reinke's edema - characteristic large-amplitude, slow, undulating mucosal wave
- Spasmodic dysphonia - irregular, aperiodic vibration pattern with abnormal adductory/abductory spasms
Stroboscopy changes the diagnosis in 30-47% of patients diagnosed by flexible endoscopy alone, and provides additional diagnostic detail in a further 32%. (Cummings Otolaryngology)
Limitations
- Not reliable when vibration is severely aperiodic (irregular F0)
- Requires patient cooperation - sustained phonation for adequate assessment
- The slow-motion image is a composite reconstruction, not true continuous recording of a single cycle (contrast with high-speed videoendoscopy)
- Rigid scope requires adequate mouth opening and gag reflex control
- Does not show subglottic or tracheal pathology
Comparison: Stroboscopy vs. High-Speed Videoendoscopy
| Feature | Stroboscopy | High-Speed Videoendoscopy |
|---|---|---|
| Frame rate | ~30 fps composite | 2000-10,000 fps |
| Periodicity required | Yes (fails with aperiodic vibration) | No |
| True slow motion | No (composite illusion) | Yes |
| Clinical availability | Widely available | Limited, expensive |
| Mucosal wave | Visualized | Better quantified |
Summary
Laryngeal stroboscopy is currently the gold standard clinical method for evaluating vocal fold vibration patterns. It uses the stroboscopic illusion to assess the mucosal wave - a marker of cover pliability that cannot be seen with continuous light - and systematically evaluates symmetry, regularity, amplitude, glottal closure, adynamic segments, and phase closure. It is indispensable in the workup of dysphonia, differentiating benign laryngeal lesions, detecting early mucosal changes suspicious for malignancy, and guiding phonosurgery.
Sources:
- Cummings Otolaryngology Head and Neck Surgery (Chapter 54, 58)
- KJ Lee's Essential Otolaryngology (p. 918)
This is a shared conversation. Sign in to Orris to start your own chat.