Malignant melanoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"melanoma"[MeSH Terms] AND "treatment"[MeSH Terms]
Reading File
Reading File
Reading File
Searching PubMed
melanoma immunotherapy checkpoint inhibitor
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material to deliver a thorough, well-structured answer on malignant melanoma. Let me compile the complete response.
Malignant Melanoma
Definition and Epidemiology
Malignant melanoma is a neoplasm arising from melanocytes - the pigment-producing cells normally found at the dermoepidermal junction (DEJ). Despite being less common than basal or squamous cell carcinoma, it is far more deadly. Its incidence has increased dramatically over recent decades, driven by increased UV exposure in fair-skinned populations and improved early detection. Australia and New Zealand have among the highest reported incidences (~33.6 per 100,000), reflecting the combination of a predominantly white-skinned immigrant population and intense sun exposure. Approximately 5% of patients with malignant melanoma will develop a second primary melanoma; 7% present as occult metastases from an unknown primary.
- Robbins & Kumar Basic Pathology, p. 894
- Bailey and Love's Short Practice of Surgery, p. 677
Risk Factors
| Category | Specific Factors |
|---|---|
| Phenotypic | Light complexion, light eyes, blonde/red hair, heavy freckling, poor tanning, easy sunburning |
| Sun exposure | Intense intermittent UV exposure in childhood; "flash fry" holiday burns favour SSM and nodular subtypes; cumulative UV favours lentigo maligna |
| Naevi | >50 common naevi, >30 sun-acquired naevi, clinically or histologically atypical (dysplastic) nevi, giant congenital nevi |
| Personal/family history | Prior melanoma, first-degree relative with melanoma |
| Genetic | CDKN2A (encodes p16 and p14 tumour suppressors) - germline mutations in ~40% of familial melanoma; BRAF mutations (non-chronically sun-exposed skin in Caucasians); KIT mutations + cyclin D1 amplification (acral and mucosal types) |
| Other | PUVA therapy, tanning lamps, xeroderma pigmentosum, immunosuppression (increases risk 20-30-fold), burn scars |
- Andrews' Diseases of the Skin, p. 802
- Bailey and Love's, p. 677
- Robbins & Kumar Basic Pathology, p. 894
Pathogenesis and Molecular Steps
Melanoma develops through stepwise acquisition of driver mutations, largely UV-induced. The diagram below illustrates the key morphologic and molecular progression:
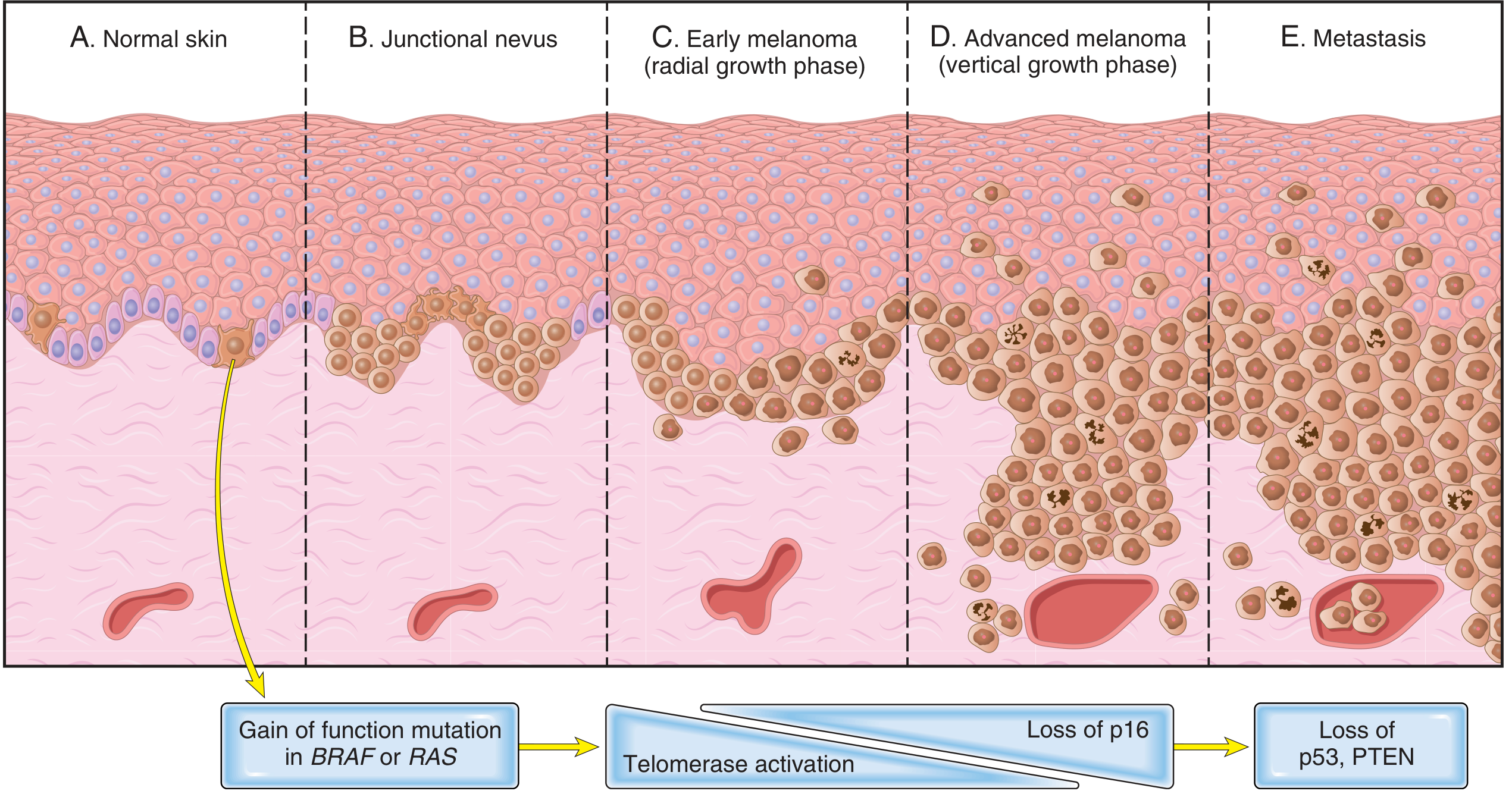
Key molecular events:
- BRAF or RAS gain-of-function mutation - drives proliferation of junctional melanocytes (forms a nevus)
- Telomerase activation - leads to transformation and early melanoma in the radial growth phase
- Loss of p16 (CDKN2A) - the CDK inhibitor that normally maintains Rb in its active state; its loss drives invasive vertical growth
- Loss of p53 and PTEN - associated with metastatic spread
The CDKN2A locus also encodes p14, which augments p53 activity by preventing its degradation. Loss of this locus therefore compromises both the Rb and p53 tumour suppressor pathways simultaneously.
- Robbins & Kumar Basic Pathology, p. 894
Growth Phases
| Phase | Behaviour | Clinical Significance |
|---|---|---|
| Radial growth phase | Lateral expansion along the DEJ; no capacity to invade or metastasize | Curable surgically |
| Vertical growth phase | Invasion into the dermis; dermal mitoses present; nodule develops | Risk of metastasis; Breslow thickness measured here |
Almost half of melanomas develop in pre-existing naevi; the remainder arise de novo on previously normal skin.
- Robbins & Kumar Basic Pathology, p. 894
- Andrews' Diseases of the Skin, p. 801
Clinical Subtypes
1. Superficial Spreading Melanoma (SSM)
- Most common - 70% of all melanomas
- Usually arises in a pre-existing naevus after years of slow change, followed by rapid growth
- Nodularity signals onset of the vertical growth phase
2. Nodular Melanoma (NM)
- 15% of all melanomas; most aggressive
- Arises de novo, lacks horizontal growth phase - no warning radial phase
- Typically blue/black papule, 1-2 cm, on trunk/head/neck; more common in men
- Up to 5% are amelanotic - a diagnostic trap
3. Lentigo Maligna Melanoma (LMM)
- Previously known as Hutchinson's melanotic freckle
- Slow-growing, variegated brown macule on face/neck/hands in the elderly
- Positively correlated with prolonged, intense cumulative sun exposure; commoner in women
- 5-10% of melanomas; less metastatic potential (slower entry into vertical growth phase)
- Biopsy is problematic due to large size, skip areas, and cosmetically sensitive locations
4. Acral Lentiginous Melanoma (ALM)
-
Affects soles, palms, and subungual regions
-
Rare in white-skinned individuals (2-8%) but most common subtype in Afro-Caribbean, Hispanic, and Asian populations (35-60%)
-
Associated with KIT gene mutations and cyclin D1/CDK4 amplifications
-
25% are amelanotic - can mimic fungal infection or pyogenic granuloma
-
Bailey and Love's Short Practice of Surgery, pp. 678-679
-
Andrews' Diseases of the Skin, p. 801
ABCDE Criteria for Clinical Recognition
| Letter | Feature |
|---|---|
| A | Asymmetry |
| B | Border irregularity |
| C | Colour variegation |
| D | Diameter >6 mm |
| E | Evolution (change in an existing lesion) |
These criteria are imperfect but valuable for lay and clinical use. Epiluminescence microscopy (dermoscopy) enhances subsurface visualisation in experienced hands, and AI-assisted dermoscopy is an emerging tool.
- Andrews' Diseases of the Skin, p. 801
- Robbins & Kumar Basic Pathology, p. 897
Histopathology
Key histological features that distinguish melanoma from a benign nevus:
- Asymmetry - melanomas are typically asymmetric
- Failure of maturation - benign nevi show smaller, more neuroid cells with descent into the dermis; melanomas do not
- Irregular junctional nests - elongated, randomly distributed, often involve arches over dermal papillae; in nevi nests are round, equidistant, at tips of rete ridges
- Buckshot scatter (pagetoid spread) - individual melanocytes scattered throughout the epidermis in SSM
- Dermal nests fail to diminish with depth (unlike nevi)
- Mitotic figures in the dermis are a key marker of vertical growth phase
- Satellite metastasis - a powerful adverse prognostic indicator
- Lymphoid infiltrate at the base, often with plasma cells
- Additional features of note: ulceration, angiolymphatic invasion, neurotropism, regression
Reports must include: Breslow thickness, margin assessment, ulceration, mitotic rate (has largely replaced Clark's level due to poor inter-observer concordance).
- Andrews' Diseases of the Skin, pp. 803-804
Staging: Breslow Thickness
Breslow thickness (measured to the nearest 0.1 mm from the top of the granular cell layer to the base of the tumour) is the single most important prognostic indicator in the absence of lymph node metastases. The AJCC staging system incorporates:
- Breslow thickness
- Ulceration
- Mitotic rate
- Lymph node involvement (N)
- Distant metastases (M)
Practical staging thresholds (surgical margins):
-
Melanoma in situ: 5 mm margin
-
<1 mm deep: 1 cm margin
-
1 mm deep: 2 cm margin (no evidence that wider margins improve outcomes)
-
Bailey and Love's Short Practice of Surgery, p. 731
Sentinel Lymph Node Biopsy (SNB/SLNB)
-
Risk of regional lymph node metastasis is proportional to Breslow thickness
-
SNB maps the first draining node(s) of a primary melanoma - offered to patients with T2a disease or greater (Breslow ≥1 mm)
-
Provides prognostic information and guides adjuvant therapy
-
Lymphatic metastases proceed in an orderly, predictable fashion - the basis of mapping
-
Bailey and Love's Short Practice of Surgery, p. 731
-
Robbins & Kumar Basic Pathology, p. 897
Metastatic Disease
When metastases occur, common sites include:
- Regional lymph nodes
- Liver
- Lungs
- Brain
- Virtually any organ
Risk of metastasis is increased by: greater Breslow thickness, high mitotic rate, ulceration, lack of local immune response, and positive sentinel node.
Treatment
Surgery (Primary and Potentially Curative)
Surgery is the only current cure for malignant melanoma. Wide local excision margins as above are standard. Lentigo maligna (melanoma in situ) requires complete excision; once fully excised, no further treatment is needed.
Targeted Therapy
- BRAF inhibitors (e.g., vemurafenib, dabrafenib): dramatic responses in patients with metastatic BRAF-mutant tumours (~50% of melanomas); however, many tumours develop resistance and recur
- KIT inhibitors: effective in KIT-mutant tumours (acral/mucosal subtypes)
Immunotherapy (Checkpoint Inhibitors)
Immune checkpoint inhibitors that augment host anti-tumour cytotoxic T-cell responses have transformed management of advanced melanoma:
- Anti-PD-1 (pembrolizumab, nivolumab)
- Anti-CTLA-4 (ipilimumab)
- Current standard for advanced disease: combinations of checkpoint inhibitors + targeted therapies (e.g., BRAF + MEK inhibitors)
- Some patients achieve remarkable tumour regression and even durable clinical remissions
A recent 2024 systematic review on checkpoint inhibitor rechallenge confirms efficacy of ICI rechallenge in advanced solid tumours including melanoma (PMID: 39726701).
- Robbins & Kumar Basic Pathology, p. 897
- Bailey and Love's Short Practice of Surgery, p. 731
Prognosis Summary
| Factor | Better Prognosis | Worse Prognosis |
|---|---|---|
| Breslow thickness | Thin (<1 mm) | Thick (>4 mm) |
| Ulceration | Absent | Present |
| Mitotic rate | Low | High |
| Lymph nodes | Negative | Positive |
| Growth phase | Radial only | Vertical |
| Tumour-infiltrating lymphocytes | Present (brisk) | Absent |
| Satellite metastasis | Absent | Present |
Most superficial melanomas detected today are cured surgically - the improvement in outcomes reflects increased public awareness of ABCDE criteria and the shift toward earlier detection.
Sources: Robbins & Kumar Basic Pathology | Andrews' Diseases of the Skin (Clinical Dermatology) | Bailey and Love's Short Practice of Surgery, 28th ed.
This is a shared conversation. Sign in to Orris to start your own chat.