Development of ossicles
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the answer.
Development of the Ossicles (Auditory Ossicles)
The three auditory ossicles — malleus, incus, and stapes — are the smallest bones in the human body. They transfer sound vibrations from the tympanic membrane to the oval window of the inner ear. Their development is a precise, arch-by-arch story.
Pharyngeal Arch Origins
| Ossicle | Pharyngeal Arch | Cartilage | Nerve |
|---|---|---|---|
| Head of malleus | 1st (mandibular) | Meckel's cartilage | CN V₃ (mandibular) |
| Body & short process of incus | 1st (mandibular) | Meckel's cartilage | CN V₃ |
| Manubrium of malleus | 2nd (hyoid) | Reichert's cartilage | CN VII (facial) |
| Long process of incus | 2nd (hyoid) | Reichert's cartilage | CN VII |
| Stapes superstructure | 2nd (hyoid) | Reichert's cartilage | CN VII |
| Stapes footplate (outer rim) | Mesodermal | Otic capsule | — |
The stapes footplate has a dual origin: the crus, base of the footplate, and head are derived from neural crest cells, while the outer rim of the footplate is derived from mesodermal cells — The Developing Human, p. 1148.
The associated muscles follow the same arch innervation rule:
- Tensor tympani (attached to malleus) → innervated by CN V₃ (1st arch nerve)
- Stapedius (attached to stapes) → innervated by CN VII (2nd arch nerve)
Timeline of Development
| Age | Event |
|---|---|
| 3 weeks | First pharyngeal pouch forms the tubotympanic recess |
| 4–6 weeks | Ossicles begin to develop from pharyngeal arch mesenchyme |
| 7 weeks | Tubotympanic recess constricted by 2nd arch → forms Eustachian tube + primitive tympanic cavity; malleoincudal and incudostapedial joints form at ~8 weeks |
| 1st half of fetal life | Ossicles appear but remain embedded in mesenchyme |
| 3rd month | Cavitation of tympanic cavity begins |
| 8th month | Surrounding mesenchyme dissolves; ossicles become free within the tympanic cavity, now lined by endodermal epithelium. The epithelium connects ossicles to the cavity wall in mesentery-like folds; supporting ligaments develop within these folds |
| Birth | Ossicles are adult size and shape |
Tympanic Cavity Formation
The tympanic cavity originates from endoderm of the first pharyngeal pouch. The distal part of the tubotympanic recess expands and gradually envelops the ossicles, their tendons, ligaments, and the chorda tympani nerve. When the mesenchyme dissolves at the 8th month, the tympanic cavity at least doubles in size, and endodermal epithelium covers the now-free ossicles via mesentery-like folds. — Langman's Medical Embryology
Diagrams
Fig. 19.9 (Langman's) — Derivatives of the first three pharyngeal arches showing ossicle origins and the mature middle ear:
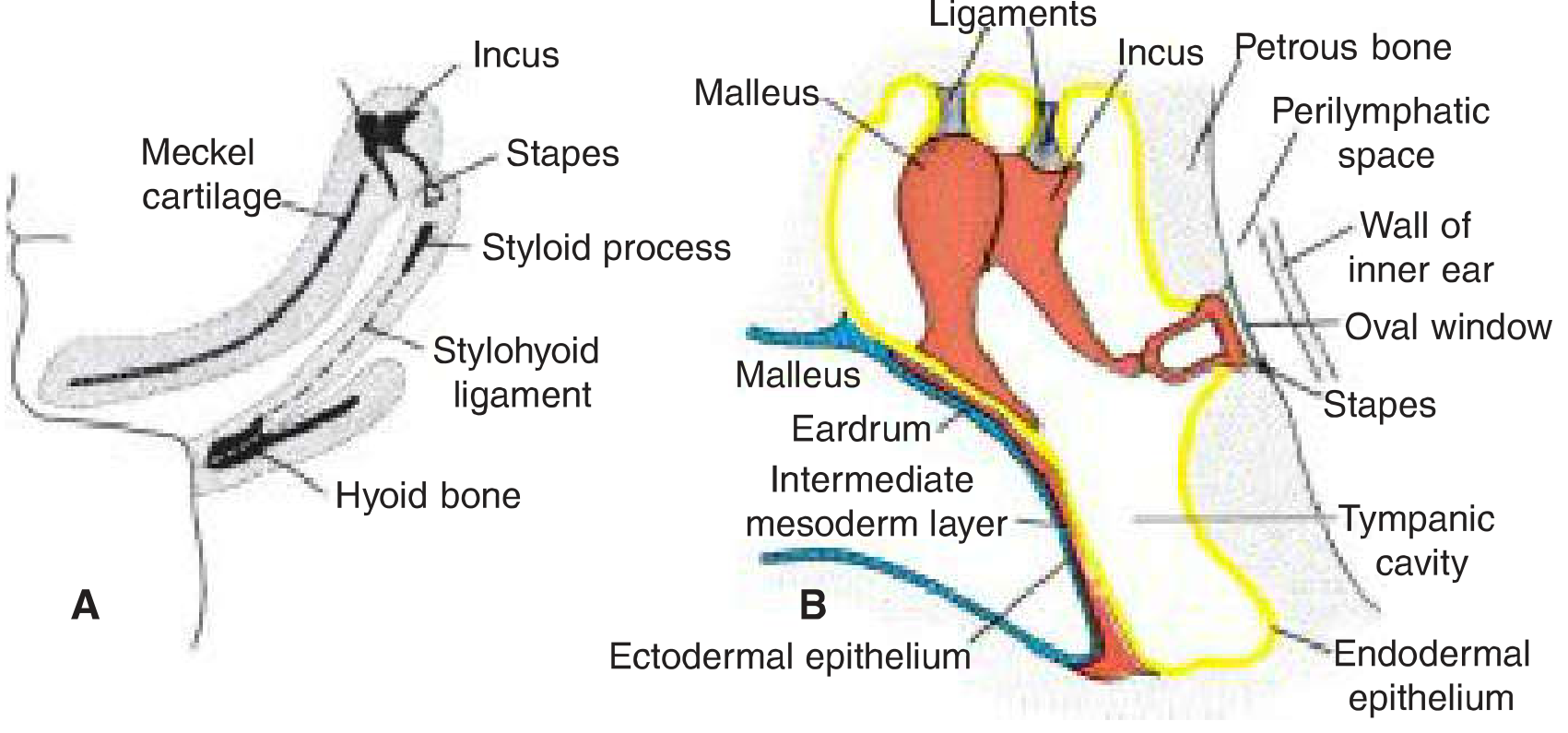
A: Meckel's cartilage (1st arch) giving rise to malleus and incus; Reichert's cartilage (2nd arch) giving rise to stapes. B: Mature configuration showing malleus handle contacting the eardrum, stapes contacting the oval window, tympanic cavity lined by endodermal epithelium.
Fig. 18.16 C & D (The Developing Human) — Development stages showing ossicles within the tympanic cavity and their relationship to the otic vesicle:
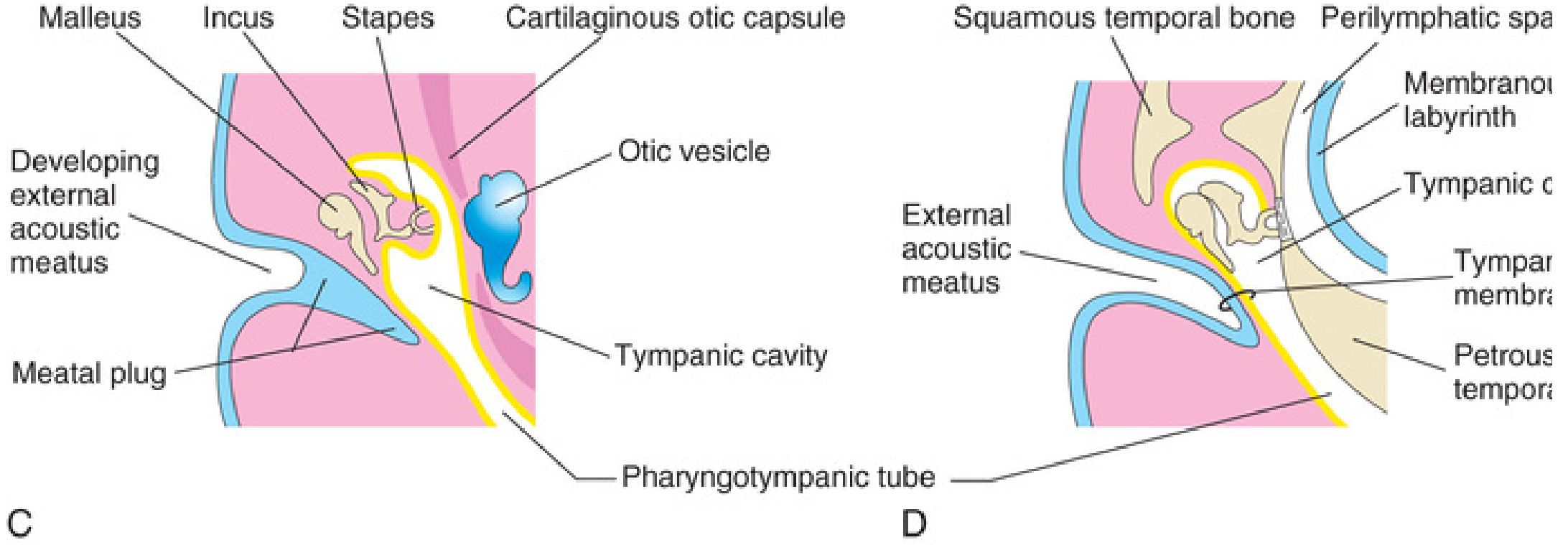
C: Ossicles embedded in mesenchyme within the developing tympanic cavity, adjacent to the otic vesicle. D: Final configuration with ossicular chain spanning the tympanic cavity.
Postnatal Changes
- Mastoid antrum appears at ~21 weeks gestation; at birth the mastoid tip is poorly developed → facial nerve is more superficial and vulnerable
- Mastoid air cells grow in the first 2–3 years of life and pneumatize the developing mastoid process
- The Eustachian tube doubles in length from birth to adulthood
Clinical Relevance
Ossicular anomalies are suspected when a child has conductive hearing loss with a normal otoscopic examination. Syndromic associations include:
- Apert/Crouzon syndrome — ankylosis of malleus and incus to the lateral wall, deformed stapes
- BOR (Branchiootorenal) syndrome — fused malleoincudal complex
- CHARGE syndrome — ossicular malformations
- Nager syndrome — external auditory canal atresia with ossicle malformations
Sources:
- Langman's Medical Embryology, 14e — pp. 374–375
- The Developing Human: Clinically Oriented Embryology — pp. 1148–1149
- KJ Lee's Essential Otolaryngology, 11e — p. 994
Ossicular anomalies
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
I have comprehensive material. Let me compile the full answer.
Ossicular Anomalies
Ossicular anomalies are broadly classified as congenital or acquired, and further as fixation (restricted movement), discontinuity/disruption (loss of chain integrity), or absence/malformation (structural defects).
Clinical Clue
Suspect an ossicular anomaly whenever a patient presents with conductive hearing loss and a normal otoscopic examination.
A preoperative air-bone gap >20–25 dB is consistent with ossicular discontinuity or fixation. — Cummings Otolaryngology, p. 2771
I. Congenital Ossicular Anomalies
A. Syndromic
| Syndrome | Ossicular Finding |
|---|---|
| Apert / Crouzon | Ankylosis of malleus and incus to lateral wall; deformed stapes |
| Beckwith-Wiedemann | Anterior bony fixation of malleus + stapes fixation; CT diagnostic; associated ear lobule crease; chr 11p15 |
| BOR (Branchiootorenal) | Fused malleoincudal complex |
| CHARGE | Abnormally shaped incus and stapes; ossicular chain fixation; absent stapedius tendon; absent stapes footplate |
| DiGeorge (22q11) | Ossicular malformations + Mondini malformation; TBX1 gene mutation |
| Goldenhar (Oculo-auriculo-vertebral dysplasia) | Ossicles fused as one block, often fused to wall of hypoplastic middle ear cavity; may also have absent ossicles; prevalence 1:45,000 |
| Hurler (MPS I) | Thick mucosa in middle ear (Hurler cells); glycosaminoglycans accumulate in ossicles, spiral ganglion, organ of Corti; chr 4p16 (alpha-L-iduronidase mutation) |
| Klippel-Feil | Deformed malleus head; rudimentary incus head; absent/short long process of incus; missing stapes parts or complete absence; fixed stapes footplate (gusher risk at surgery) |
| Nager syndrome | External auditory canal atresia + ossicle malformations; conductive and mixed hearing loss |
B. Nonsyndromic
1. Congenital stapes ankylosis
- Accounts for 50–70% of congenital stapes fixation
- Management: hearing aids initially; stapedectomy when older
2. Congenital stapes fixation with perilymphatic gusher (X-linked)
- Also known as Phelps syndrome / X-linked stapes gusher
- Most common X-linked form of deafness
- Caused by mutation in POU3F4 gene on Xq21
- Stapes is fixed to the oval window → manipulation during surgery risks dead ear due to profuse perilymph leak ("gusher")
- CT: widening of the lateral internal auditory canal; abnormal communication between IAC and cochlea
3. Juvenile otosclerosis
- 15% develop symptoms as children; progressive hearing loss from ~10 years of age
- Usually bilateral (90%); family history in ~50%
II. Acquired Ossicular Anomalies
A. Discontinuity / Erosion
The most commonly encountered ossicular abnormality in chronic otitis media is an absent lenticular process (long process) of the incus — eroded by disease, cholesteatoma, or chronic infection. — Cummings Otolaryngology
| Cause | Mechanism | Typical Finding |
|---|---|---|
| Chronic otitis media | Avascular necrosis of lenticular process | Absent/eroded incus long process |
| Cholesteatoma | Enzymatic bone erosion + pressure | Progressive ossicular destruction, often incus first, then malleus, then stapes |
| Trauma (temporal bone fracture) | Direct disruption | Incudostapedial joint dislocation most common |
| Tympanosclerosis | Dystrophic calcification/hyaline deposits from recurrent infection | Fixation of malleus head, incus, or stapes footplate |
B. Fixation
- Tympanosclerosis — calcification may immobilize any ossicle; high recurrence rate after surgery
- Ossicular head fixation — malleus head fixed in epitympanum; managed by atticotomy, releasing bony union, and removing head with malleus nipper or microdrill
III. Classification by Type
| Type | Examples |
|---|---|
| Fixation | Congenital stapes ankylosis, otosclerosis, tympanosclerosis, bony fusion to lateral wall |
| Discontinuity | Trauma, incus erosion in COM/cholesteatoma, incudostapedial joint dislocation |
| Absence/Malformation | Goldenhar (fused block or absent), Klippel-Feil, CHARGE (absent footplate) |
IV. Diagnosis
- CT temporal bone (fine-cut, 0.625 mm, without contrast) — primary imaging modality; assesses ossicular morphology, fixation, bony defects
- Audiometry — air-bone gap >20–25 dB with normal bone conduction and type As or type Ad on tympanometry
- Tympanometry — type As (reduced compliance) → fixation; type Ad (hypercompliant) → discontinuity
- Intraoperative assessment — most accurate for reconstructive planning
V. Management — Ossiculoplasty
Successful reconstruction requires:
- Mobile, well-oriented tympanic membrane
- Normalized middle ear pressure and mucosa
- Eradication of middle ear disease
Reconstruction Options
When stapes superstructure is intact:
- Incus interposition — sculpted autologous incus as a strut between stapes capitulum and malleus handle (preferred if incus is available)
- PORP (Partial Ossicular Replacement Prosthesis) — titanium or biocompatible prosthesis; fitted with a 0.5–0.7 mm cartilage cap to reduce drum erosion and extrusion
When stapes superstructure is absent:
- TORP (Total Ossicular Replacement Prosthesis) — placed from tympanic membrane to stapes footplate in parallel piston motion
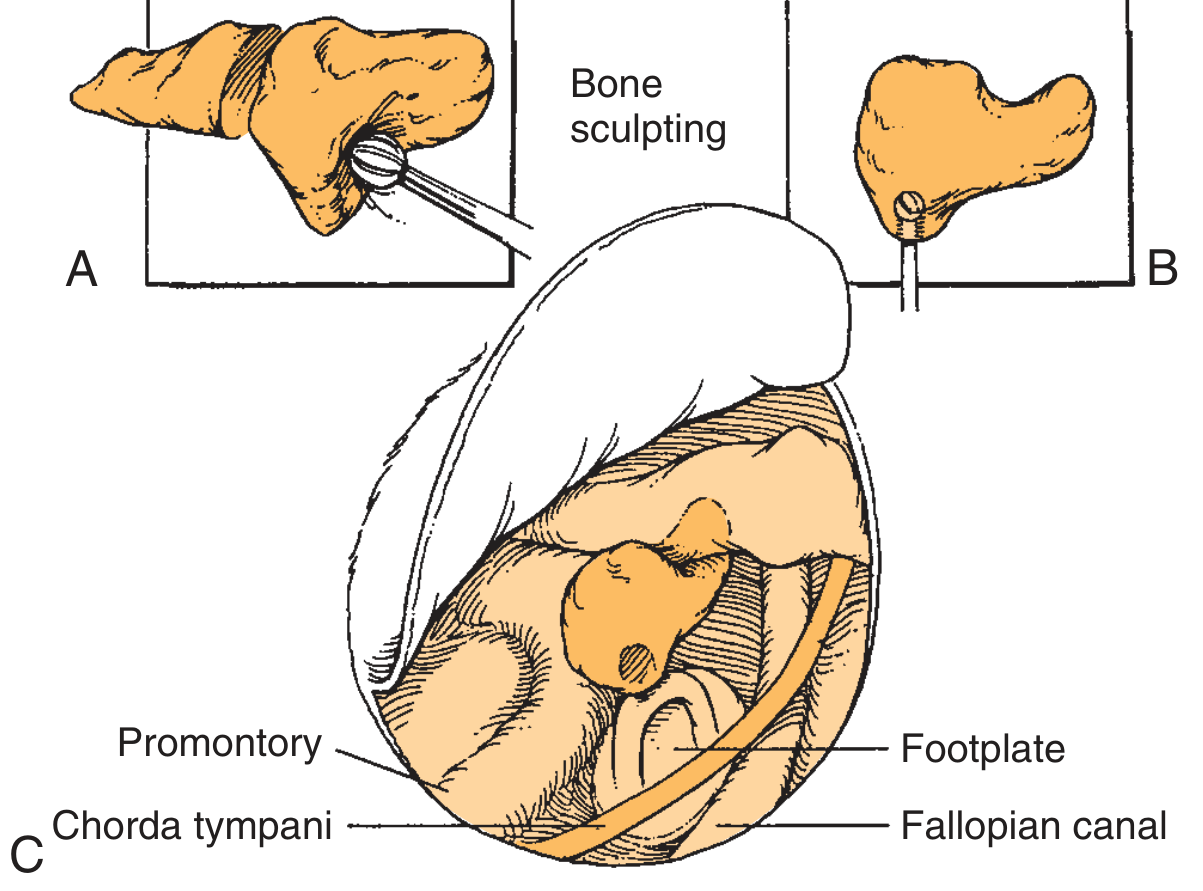
A & B: The incus is sculpted to fit between stapes capitulum and malleus handle. C: Modified incus positioned to restore chain continuity, with key middle ear landmarks (promontory, footplate, chorda tympani, Fallopian canal).
Preoperative Considerations (Cummings Box 145.2)
- Air-bone gap >20–25 dB → consistent with ossicular discontinuity or fixation
- ABG <30 dB preoperatively → approach with caution (small surgical gain may still require amplification)
- Bone (sensorineural) level >30 dB → reconstruction results often unsatisfactory if goal is to avoid amplification
- Bringing the operative ear to within 15 dB of the contralateral ear facilitates binaural input
Sources:
- KJ Lee's Essential Otolaryngology, 11e — pp. 994–996
- Cummings Otolaryngology: Head and Neck Surgery — pp. 2769–2773
- The Developing Human: Clinically Oriented Embryology — p. 1148
This is a shared conversation. Sign in to Orris to start your own chat.