Horners syndrome
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Horner syndrome"[MeSH Terms]
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have everything needed for a thorough response. Here is the comprehensive answer:
Horner Syndrome (Oculosympathetic Palsy)
Horner syndrome results from disruption of the three-neuron sympathetic pathway to the eye and face. It is named after the Swiss ophthalmologist Johann Friedrich Horner, though the French often call it Bernard-Horner syndrome.
Anatomy of the Sympathetic Pathway
The sympathetic innervation to the eye follows a three-neuron chain:
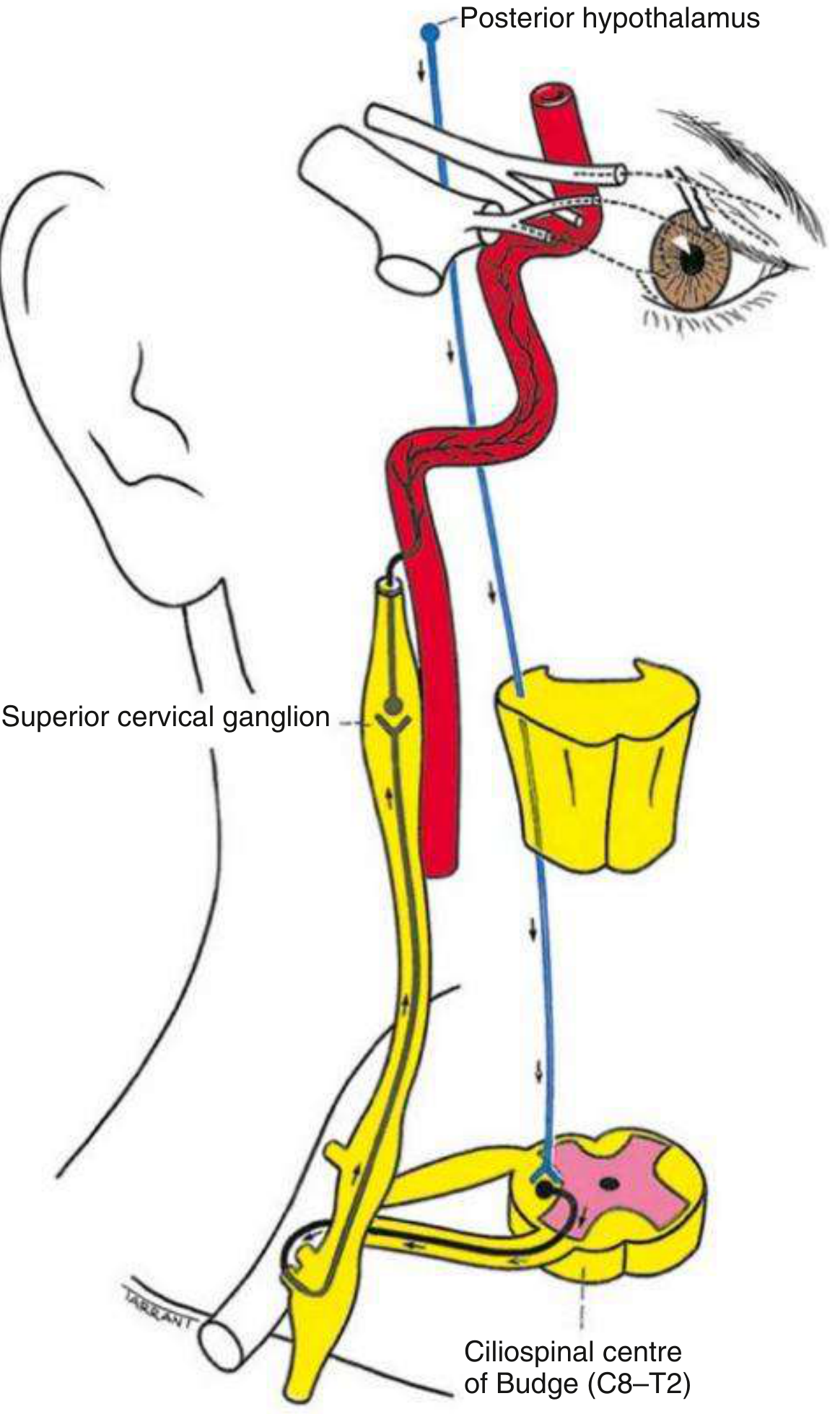
Fig. 19.37 - Anatomical pathway of the sympathetic nerve supply (Kanski's Clinical Ophthalmology, 10th ed.)
| Neuron | Course | Key Relations |
|---|---|---|
| 1st order (central) | Posterior hypothalamus → descends uncrossed through the brainstem → ciliospinal centre of Budge (C8-T2 lateral horn of spinal cord) | Traverses the lateral tegmentum of brainstem |
| 2nd order (preganglionic) | Ciliospinal centre → passes over the apex of the lung and under the subclavian artery → superior cervical ganglion | Closely related to the apical pleura (Pancoast tumour vulnerability) |
| 3rd order (postganglionic) | Superior cervical ganglion → ascends along the internal carotid artery → cavernous sinus → joins CN V1 (ophthalmic) → via nasociliary nerve and long ciliary nerves to the dilator pupillae and Müller's muscle | Facial sudomotor fibres travel along the external carotid artery |
- Kanski's Clinical Ophthalmology, 10th ed., p. 806-807
- Adams and Victor's Principles of Neurology, 12th ed., p. 298
Clinical Features
The classic triad is:
- Miosis - constriction of the pupil due to loss of sympathetic innervation to the dilator pupillae; the sphincter pupillae acts unopposed
- Ptosis - partial drooping (1-2 mm) of the upper eyelid due to paresis of Müller's smooth muscle
- Anhidrosis - reduced or absent sweating of the ipsilateral face (only present if the lesion is below the superior cervical ganglion, since sudomotor fibres run along the external carotid)
Additional features:
- Inferior ptosis (reverse ptosis / elevation of the lower lid) - due to weakness of the inferior tarsal muscle
- Apparent enophthalmos - actually an illusion created by the narrowed palpebral fissure
- Dilation lag - the affected pupil redilates slower than the normal side when lights are suddenly switched off; this is the most sensitive sign
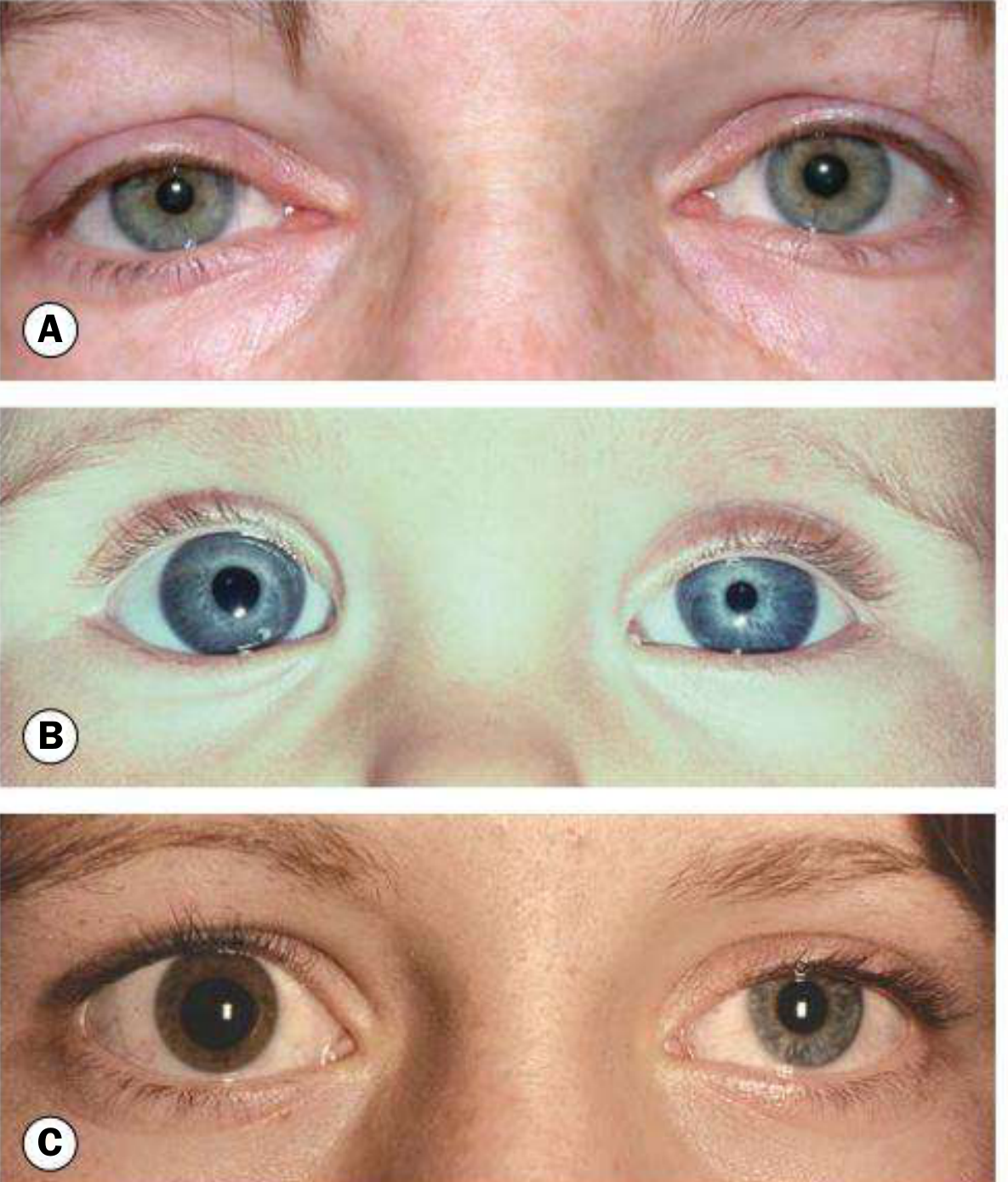
- Hypochromic heterochromia - iris on the Horner side is lighter in colour; seen when congenital or longstanding
Note: anisocoria is accentuated in the dark (opposite of a CN III palsy where anisocoria is worse in bright light). The pupillary light reflex is preserved.
(Kanski's Clinical Ophthalmology, 10th ed.)
Congenital Horner syndrome (left) with heterochromia iridis - Adams and Victor's Principles of Neurology, 12th ed.
Causes by Neuron Level
1st order (central) lesions
- Brainstem stroke - commonly the lateral medullary (Wallenberg) syndrome (PICA territory infarct)
- Brainstem tumour or demyelination
- Syringomyelia
- Cervical spinal cord lesion (trauma, tumour)
- High cervical cord transection (bilateral Horner)
2nd order (preganglionic) lesions
- Pancoast tumour (apical lung carcinoma) - classic high-yield cause
- Carotid or aortic aneurysm/dissection
- Thoracic spinal cord lesion
- Neck lesions: thyroid tumour, enlarged lymph nodes, neck trauma, post-surgical
3rd order (postganglionic) lesions
- Internal carotid artery dissection - painful acute Horner = emergency
- Nasopharyngeal tumour
- Cavernous sinus mass (thrombosis, aneurysm, tumour)
- Otitis media
- Cluster headache (migrainous neuralgia)
Important: Most isolated postganglionic Horner syndromes are microvascular, but this cannot be assumed without investigation. - Kanski's Clinical Ophthalmology, 10th ed.
Congenital
- Perinatal injury to the sympathetic chain in the neck
- A hereditary autosomal dominant form exists, often with heterochromia iridis
Localization Using Anhidrosis Pattern
The sweating pattern helps localize the lesion:
- Common carotid level lesion: loss of sweating over the entire side of the face
- Distal to carotid bifurcation: anhidrosis absent or confined to the medial forehead and side of nose only (since sudomotor fibres branch off with the external carotid artery)
Pharmacological Testing
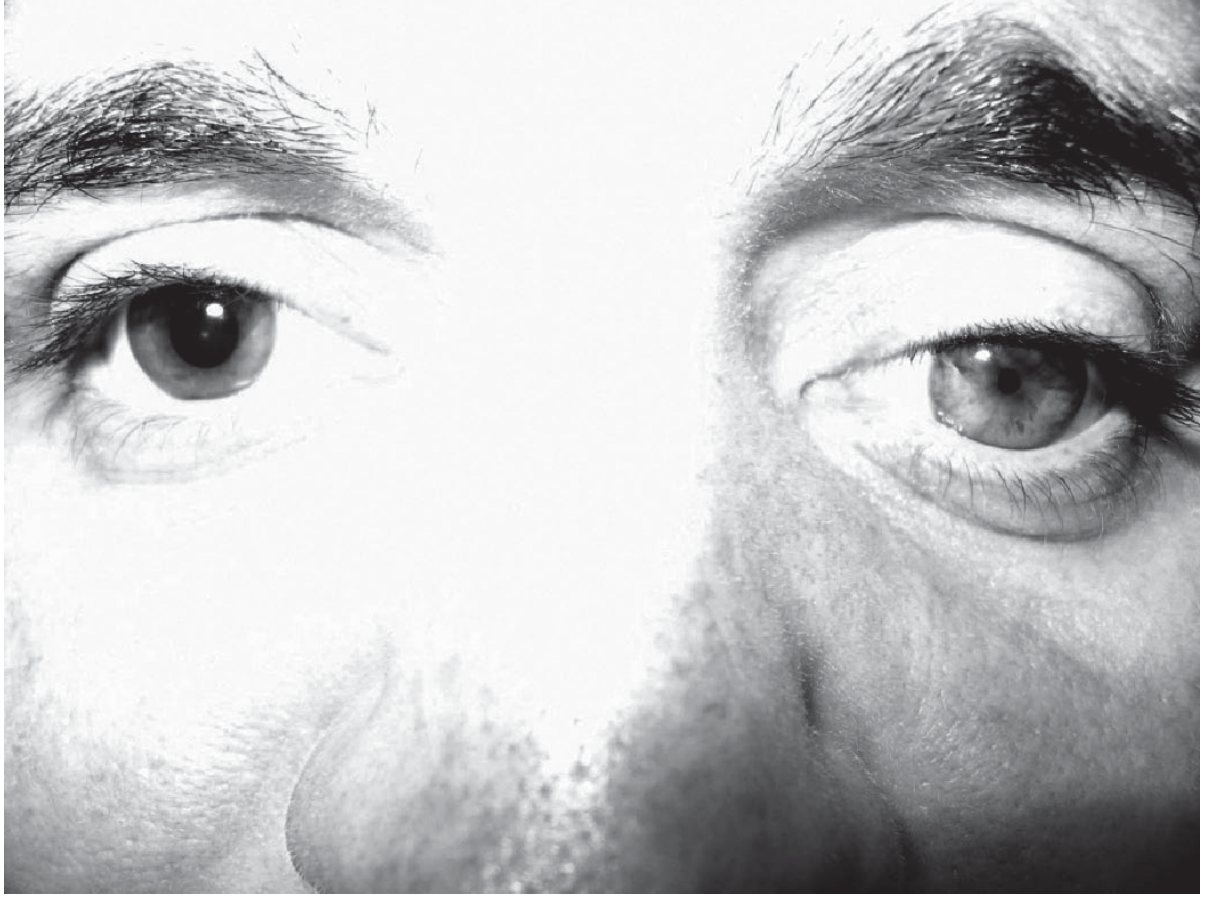
Confirming the diagnosis: Apraclonidine test (preferred)
- Drug: Apraclonidine 0.5% or 1.0% (weak alpha-1 agonist)
- Mechanism: Normally has little dilatory effect, but in Horner syndrome, denervation hypersensitivity upregulates alpha-1 receptors on the dilator pupillae, causing the Horner pupil to dilate and the ptosis to improve
- Result: Horner pupil dilates; normal pupil unaffected - anisocoria reverses
- Read at: 30-45 minutes after instillation
- Sensitivity ~90%, specificity ~100%
- Caution: Do NOT use in infants (crosses the blood-brain barrier). Has a latency of ~7 days before becoming positive. Avoid repeat pharmacological testing for 3-5 days after.

Fig. 19.40 - Apraclonidine test in acquired Horner syndrome from traumatic right ICA dissection (Kanski's Clinical Ophthalmology, 10th ed.)
Cocaine test (less commonly used)
- Drug: Cocaine 4%
- Mechanism: Blocks reuptake of norepinephrine at the synapse. With intact sympathetic innervation, the normal pupil dilates. In Horner syndrome, there is no norepinephrine released, so the Horner pupil fails to dilate
- A difference in pupil size of ≥0.8 mm is considered diagnostic
Localizing pre- vs. postganglionic: Hydroxyamphetamine test
- Hydroxyamphetamine causes NE release from nerve terminals
- In 3rd order (postganglionic) lesions, the terminal is degenerated → no NE release → pupil does not dilate
- In 1st or 2nd order lesions, the postganglionic terminal is intact → pupil does dilate
Key Differentials for Anisocoria
| Condition | Anisocoria worse in | Light reflex (affected eye) | Key feature |
|---|---|---|---|
| Horner syndrome | Dark | Normal | Dilation lag; ptosis 1-2 mm |
| CN III palsy | Bright light | Absent (blown pupil) | Ptosis severe; eye deviated down-and-out |
| Adie tonic pupil | Bright light | Poor (sustained light needed) | Associated limb areflexia |
| Argyll Robertson | Both (small, irregular) | Absent | Light-near dissociation; syphilis/diabetes |
| Physiologic anisocoria | Neither (equal in both) | Normal | <0.5 mm difference |
Ciliospinal Reflex
Painful pinch to the neck (C2, C3 afferents) normally activates sympathetic outflow and causes ipsilateral pupillary dilation. In Horner syndrome, this reflex is absent on the affected side. This is a useful bedside test.
Bilateral Horner Syndrome
Rare. Causes include:
- Autonomic neuropathies
- High cervical cord transection
- Bilateral miosis may be subtle - best detected by noting a prolonged dilation lag when light is withdrawn
Emergency Note
An acute painful Horner syndrome must be treated as an emergency. It should raise immediate concern for carotid artery dissection and requires urgent vascular imaging (MRI/MRA or CT angiography of the neck). - Kanski's Clinical Ophthalmology, 10th ed.
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 806-809
- Adams and Victor's Principles of Neurology, 12th ed., pp. 298-299
- Neuroanatomy through Clinical Cases, 3rd ed.
- ROSEN's Emergency Medicine, 9th ed.
- The 2025 ACR Appropriateness Criteria for Horner Syndrome (PMID: 41193044) provides current imaging guidance for workup.
This is a shared conversation. Sign in to Orris to start your own chat.