Innate immunity
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content. Let me compile the full, well-organized answer:
Innate Immunity
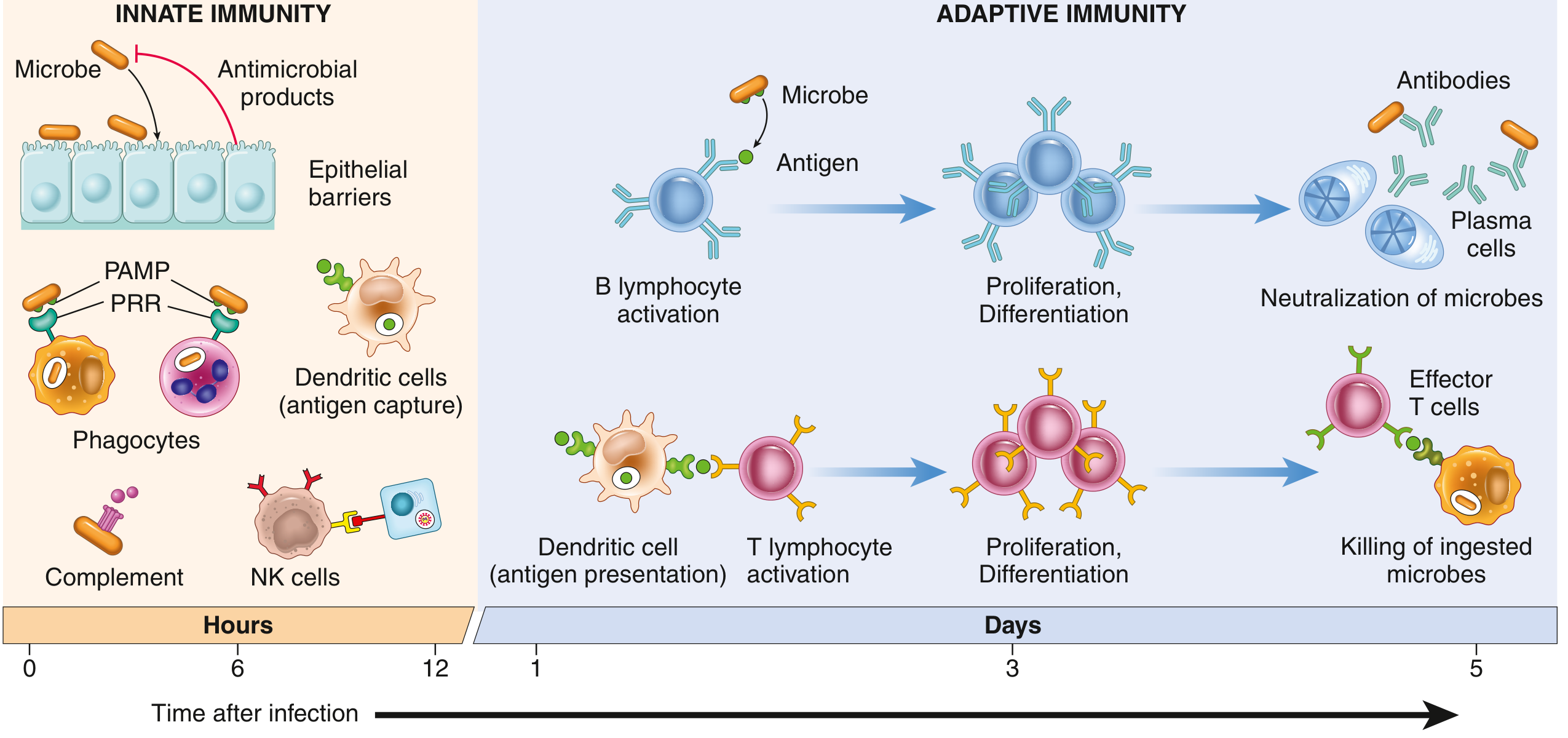
Fig. 5.1 - Principal components and kinetics of innate and adaptive immune responses (Robbins & Kumar Basic Pathology)
Definition
Innate immunity (also called natural or native immunity) refers to intrinsic host defense mechanisms that are always present, ready to react immediately, and constitute the first line of defense. Unlike adaptive immunity, which develops over days in response to specific antigens, innate immunity acts within minutes to hours of infection.
The key distinction is that innate immunity recognizes conserved microbial patterns rather than specific antigens, and it does not generate immunological memory.
Components of Innate Immunity
Innate immunity consists of two broad arms:
| Arm | Includes |
|---|---|
| Cellular | Macrophages, neutrophils, NK cells, dendritic cells, innate lymphoid cells (ILCs), mast cells |
| Humoral | Complement system, mannose-binding lectin (MBL), C-reactive protein (CRP), defensins, surfactant |
1. Epithelial Barriers (First Line)
- Skin, respiratory, and GI epithelia act as mechanical barriers to microbial entry
- Epithelial cells secrete antimicrobial peptides such as defensins
- Intraepithelial lymphocytes (especially in the gut) add a cellular defense at these surfaces
2. Phagocytic Cells
Neutrophils are rapidly recruited from blood to sites of infection. They phagocytose and destroy microbes via:
- Reactive oxygen species (respiratory burst via NADPH oxidase)
- Lysosomal enzymes
- Antimicrobial peptides
Macrophages are the dominant phagocytes in tissues. They arise from circulating monocytes and from embryonic precursors (yolk sac / fetal liver). Tissue-specific macrophages include:
- Kupffer cells (liver)
- Microglia (brain)
- Alveolar macrophages (lungs)
Macrophages phagocytose microbes, produce inflammatory cytokines (TNF, IL-1, IL-6, IL-12), and activate the adaptive immune system.
3. Dendritic Cells (DCs)
DCs serve as sentinels in epithelia, lymphoid organs, and most tissues. They:
- Capture and present antigens to T lymphocytes (linking innate to adaptive immunity)
- Express pattern recognition receptors (PRRs) to detect danger signals
- Secrete cytokines that direct adaptive immune responses
- Are not directly involved in microbial killing (unlike macrophages)
4. Natural Killer (NK) Cells
NK cells are innate lymphocytes that kill:
- Virus-infected cells (which downregulate MHC-I to evade T cells - NK cells detect this "missing self")
- Tumor cells
They function via:
- Perforin/granzyme pathway
- Fas-FasL interactions
- Antibody-dependent cellular cytotoxicity (ADCC)
NK cells also produce IFN-gamma, which activates macrophages.
5. Innate Lymphoid Cells (ILCs)
ILCs are tissue-resident lymphocytes that lack T-cell antigen receptors. They are activated by cytokines, not antigens. Classified into three groups:
- ILC1 - produces IFN-gamma (mirrors Th1 function)
- ILC2 - produces IL-4, IL-5, IL-13 (mirrors Th2; important in allergy and parasitic defense)
- ILC3 - produces IL-17, IL-22 (mirrors Th17; important at mucosal barriers)
6. Plasma Proteins
- Complement: Activated via the alternative pathway (spontaneous C3 hydrolysis) or lectin pathway (MBL binds mannose on microbes) - both are part of innate immunity
- Mannose-binding lectin (MBL): Binds mannose-rich carbohydrates on bacteria/fungi, acts as an opsonin and activates complement
- C-reactive protein (CRP): Acute-phase protein that coats microbes (opsonization) and activates complement
- Lung surfactant: Protects against inhaled microbes
Pattern Recognition Receptors (PRRs)
PRRs are the molecular basis of innate immune recognition. They recognize conserved structures called pathogen-associated molecular patterns (PAMPs) and host damage signals called damage-associated molecular patterns (DAMPs).
Key features of PAMPs:
- Shared among related microbes
- Essential for microbial survival - so microbes cannot easily mutate these structures to escape immunity
- Not found in mammalian cells
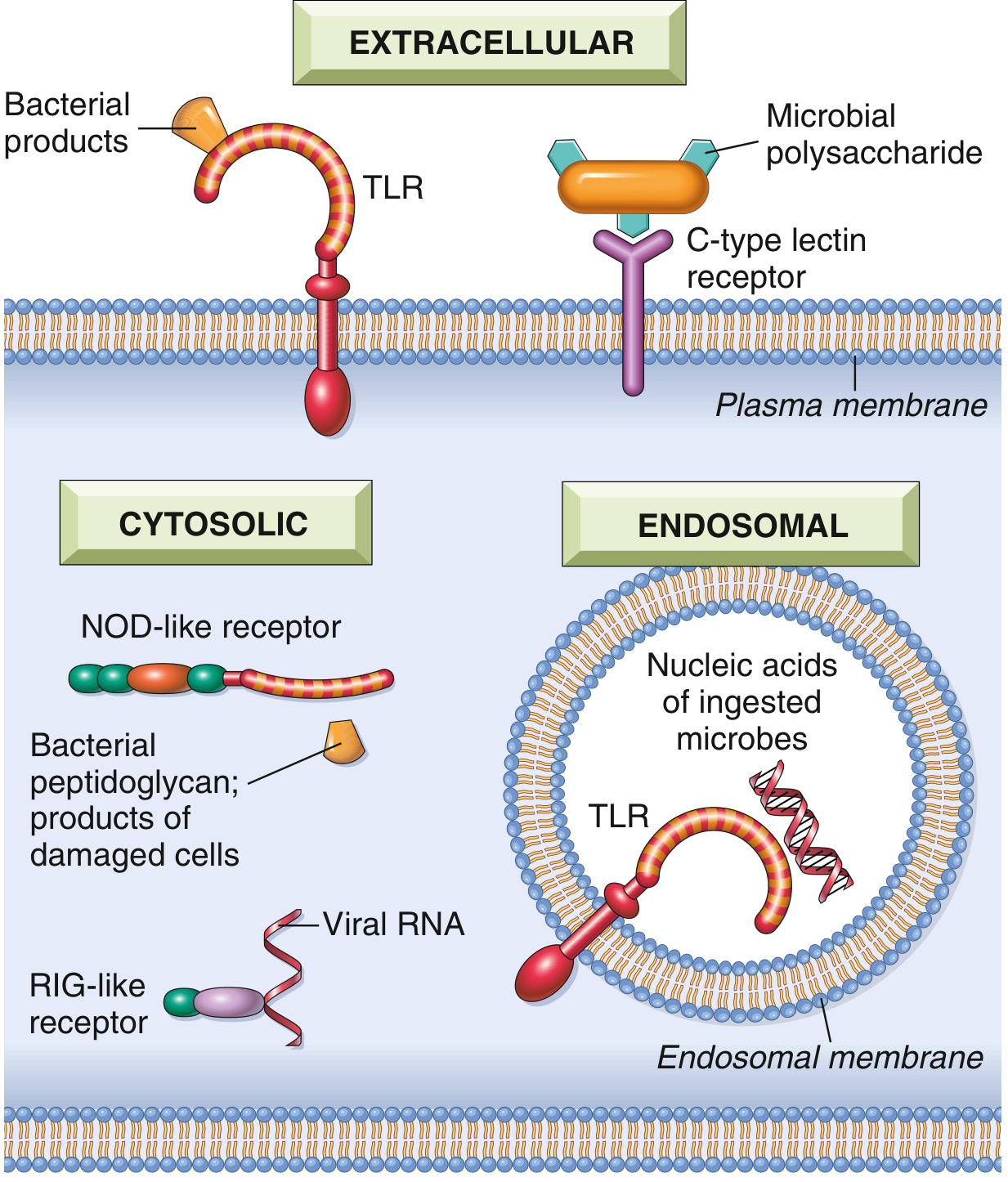
Cellular locations of pattern recognition receptors (Robbins & Kumar Basic Pathology)
PRRs are found in three cellular compartments:
a. Toll-Like Receptors (TLRs)
The best-characterized PRRs. Mammals have 10 TLRs.
- Plasma membrane TLRs: Detect bacterial products (e.g., LPS detected by TLR4, flagellin by TLR5, lipoteichoic acids by TLR2)
- Endosomal TLRs: Detect viral/bacterial nucleic acids after phagocytosis (e.g., dsRNA by TLR3, ssRNA by TLR7/8, CpG DNA by TLR9)
Signaling: All TLRs signal via a common pathway activating:
- NF-kB - stimulates cytokine synthesis and adhesion molecule expression (drives inflammation)
- Interferon Regulatory Factors (IRFs) - stimulate type I interferon (IFN-alpha/beta) production (antiviral defense)
Loss-of-function TLR mutations cause rare but serious immunodeficiency syndromes.
b. NOD-Like Receptors (NLRs) and the Inflammasome
NLRs are cytosolic receptors that recognize:
- Bacterial peptidoglycan fragments (NOD1, NOD2)
- Products of necrotic cells (uric acid, ATP)
- Ion disturbances (K+ loss)
- Various PAMPs
Several NLRs (particularly NLRP3) assemble a multiprotein complex called the inflammasome, which:
- Activates caspase-1
- Caspase-1 cleaves pro-IL-1beta and pro-IL-18 into their active forms
- Can also trigger pyroptosis (inflammatory cell death)
Clinical importance:
- Gain-of-function NLR mutations cause autoinflammatory syndromes - respond to IL-1 antagonists
- NLRP3 activation by urate crystals underlies inflammation in gout
- NLRP3 activation by cholesterol crystals may contribute to atherosclerosis
c. RIG-Like Receptors (RLRs)
Cytosolic sensors for viral RNA (RIG-I, MDA5). Detect viral RNA generated during replication and trigger type I interferon production.
d. Cytosolic DNA Sensors (cGAS-STING Pathway)
- cGAS (cyclic GMP-AMP synthase) detects cytosolic dsDNA
- Produces cGAMP, which activates STING (Stimulator of Interferon Genes)
- Leads to type I IFN production
- Activated by viral DNA, bacterial DNA, and aberrant self-DNA (nuclear damage)
- Defects in this regulation cause interferonopathies (e.g., Aicardi-Goutieres syndrome)
e. C-Type Lectin Receptors (CLRs)
- On macrophages and DCs
- Recognize microbial polysaccharides (bacterial and fungal cell walls)
- Stimulate phagocytosis and inflammatory responses
- Important in defense against fungi (e.g., Dectin-1 recognizes beta-glucan on Candida)
f. G Protein-Coupled Receptors
- On neutrophils and macrophages
- Recognize N-formylmethionyl peptides (fMLP) from bacterial proteins (bacteria initiate protein synthesis with fMet; mammalian cells do not)
- Drive leukocyte chemotaxis toward bacteria
Reactions of Innate Immunity
1. Inflammation
Innate recognition triggers:
- Cytokine release (TNF, IL-1, IL-6, IL-12, CXCL8/IL-8)
- Complement activation (C3a, C5a - anaphylatoxins)
- Recruitment and activation of neutrophils and macrophages
- Vascular changes (vasodilation, increased permeability)
- Fever (via IL-1, IL-6, TNF acting on hypothalamus)
2. Antiviral Defense
Type I interferons (IFN-alpha/beta) produced in response to viral PAMPs:
- Act on infected and uninfected cells
- Upregulate antiviral enzymes (e.g., RNase L, protein kinase R)
- Degrade viral nucleic acids and inhibit viral replication
- Upregulate MHC-I expression (enhancing cytotoxic T cell recognition)
Innate Immunity and the Link to Adaptive Immunity
Innate immunity does not just defend directly - it primes and shapes the subsequent adaptive immune response:
| Innate Signal | Effect on Adaptive Immunity |
|---|---|
| IL-12 from macrophages/DCs | Promotes Th1 differentiation |
| IL-4 from mast cells/ILC2 | Promotes Th2 differentiation |
| IL-6 + IL-23 from DCs | Promotes Th17 differentiation |
| Costimulatory molecules (CD80/86) upregulated by TLR signals | Required for T cell activation |
| Dendritic cell migration to lymph nodes | Presents antigen to naive T cells |
Without these innate signals, adaptive immune responses are weak or fail to occur - which is why innate immunity is truly foundational.
Clinical Correlations
| Defect | Disease |
|---|---|
| TLR signaling pathway mutations | Recurrent bacterial/viral infections |
| NLRP3 gain-of-function | Autoinflammatory syndromes (CAPS) |
| NLRP3 activation by urate | Gout |
| cGAS-STING dysregulation | Interferonopathies (Aicardi-Goutieres) |
| NK cell deficiency | Severe herpesvirus infections |
| Complement deficiency (C3) | Recurrent encapsulated bacterial infections |
| MBL deficiency | Increased susceptibility to infections, especially in early childhood |
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Chapter 6
- Robbins & Kumar Basic Pathology, Chapter 5
- Cellular and Molecular Immunology (Abbas, Lichtman & Pillai)
- Janeway's Immunobiology, 10e
innate immunity immunology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Here is the comprehensive immunology-focused coverage of innate immunity, drawn from Janeway's Immunobiology 10e, Cellular and Molecular Immunology (Abbas, Lichtman & Pillai), and Robbins & Kumar:
Innate Immunity - Immunology
Overview: Innate vs. Adaptive Immunity
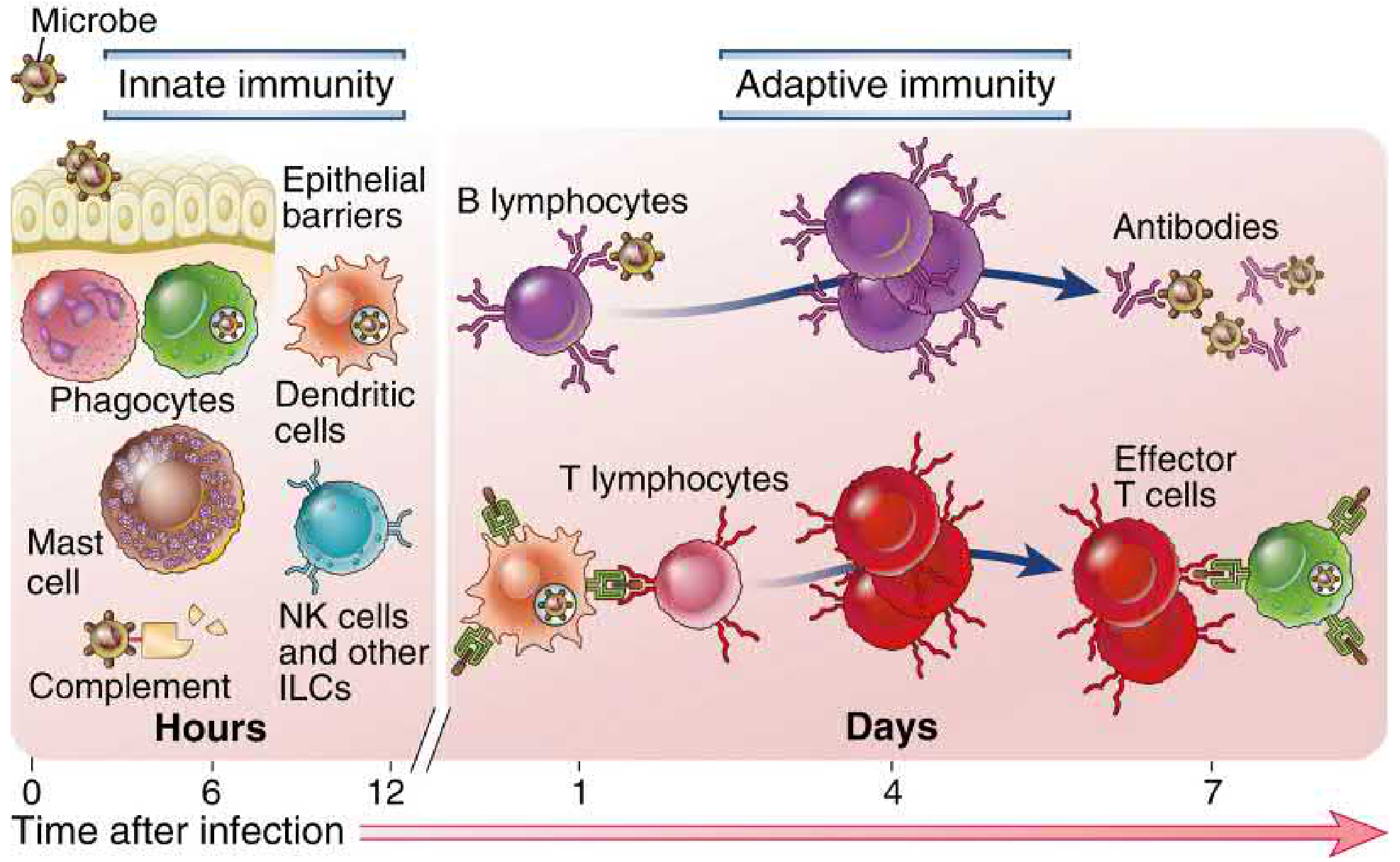
Fig. 1.1 - Innate immunity acts within hours; adaptive immunity develops over days (Cellular and Molecular Immunology)
Defense against microbes is mediated by two sequential, coordinated systems. Innate immunity (also called natural or native immunity) provides the immediate response - mechanisms that are in place before infection ever occurs. Adaptive immunity develops later but is more powerful and antigen-specific.
| Feature | Innate Immunity | Adaptive Immunity |
|---|---|---|
| Timing | Minutes to hours | Days to weeks |
| Specificity | Groups of related microbes (shared PAMPs) | Single specific antigens (epitopes) |
| Receptor diversity | Low; encoded in germline genes | Extremely high; generated by somatic recombination (V(D)J) |
| Memory | Limited | Yes - long-lasting |
| Self-nonself discrimination | Yes | Yes |
| Key cells | Phagocytes, DCs, NK cells, ILCs, mast cells | B cells, T cells, plasma cells |
| Key secreted molecules | Complement, lectins, defensins, cytokines | Antibodies |
"Innate immunity is essential for defending against microbes in the first few hours or days after infection, before adaptive immune responses have developed." - Cellular and Molecular Immunology
Cellular Origin: From Bone Marrow to Effector
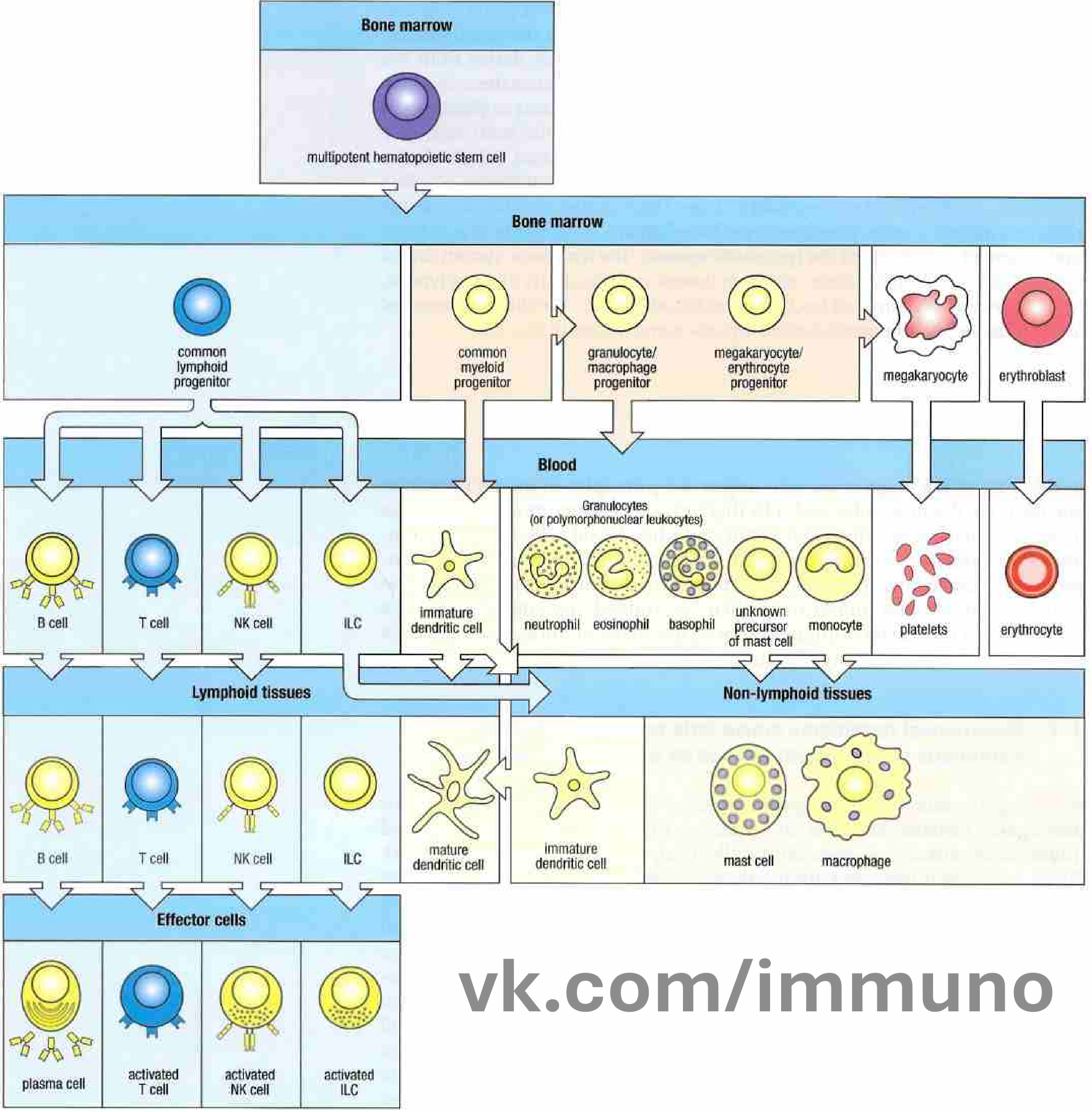
Fig. 1.3 - All immune cells arise from multipotent hematopoietic stem cells in the bone marrow (Janeway's Immunobiology 10e)
Innate immune cells arise from two progenitor lineages:
- Common Myeloid Progenitor (CMP): Gives rise to macrophages, neutrophils, eosinophils, basophils, mast cells, and dendritic cells - the dominant cells of innate immunity
- Common Lymphoid Progenitor (CLP): Gives rise to NK cells and ILCs (innate lymphoid lineages), alongside adaptive B and T cells
Components of Innate Immunity
1. Physical and Chemical Barriers
The first line of defense - prevent microbial entry before any immune response is needed:
- Skin epithelium: Physical barrier; low pH; fatty acids on surface
- Mucosal epithelia (GI, respiratory, urogenital): Tight junctions; mucus trapping; ciliary clearance (mucociliary escalator)
- Antimicrobial molecules:
- Defensins: Small cationic peptides that disrupt microbial membranes. Produced by epithelial cells and neutrophils (alpha-defensins in crypts of Lieberkuhn)
- Lysozyme: Cleaves bacterial peptidoglycan (present in saliva, tears, mucus)
- Lactoferrin: Sequesters iron needed for bacterial growth
- Secretory IgA (bridges innate structure with adaptive product): Prevents microbial attachment at mucosal surfaces
2. Phagocytic Cells
Macrophages
Macrophages are long-lived, tissue-resident phagocytes present in virtually all tissues. They arise from:
- Embryonic precursors (yolk sac / fetal liver) - populate tissues before birth
- Adult bone marrow monocytes - circulate in blood and differentiate into macrophages upon entering tissues
Tissue-specific macrophages:
| Tissue | Macrophage Name |
|---|---|
| Liver | Kupffer cells |
| Brain | Microglia |
| Lung | Alveolar macrophages |
| Bone | Osteoclasts |
| Kidney | Mesangial cells |
| Skin | Langerhans cells (immature DC-like) |
Functions:
- Phagocytosis and killing of microbes (respiratory burst, lysosomal enzymes)
- Production of inflammatory cytokines: TNF, IL-1, IL-6, IL-12, IL-23, CXCL8
- Activation of complement via secreted pattern recognition molecules
- Antigen presentation to T cells (link to adaptive immunity)
- Tissue repair and resolution of inflammation
Neutrophils (Polymorphonuclear Leukocytes)
Short-lived (~hours in tissues) but the most abundant phagocyte in blood. First to arrive at infection sites.
Killing mechanisms:
- Respiratory burst: NADPH oxidase generates superoxide → H₂O₂, hypochlorous acid (HOCl via myeloperoxidase)
- Degranulation: Azurophilic granules release elastase, cathepsin G, defensins
- Neutrophil Extracellular Traps (NETs): Chromatin + antimicrobial proteins expelled to trap and kill extracellular pathogens
Monocytes
Circulate in blood as precursors; enter tissues and differentiate into macrophages or monocyte-derived DCs. Two populations:
- Classical monocytes (CD14hi CD16-): Patrolling, highly phagocytic
- Non-classical monocytes (CD14lo CD16+): More inflammatory, patrolling vasculature
3. Dendritic Cells (DCs)
DCs are the primary sentinel cells that bridge innate and adaptive immunity. Discovered by Ralph Steinman (Nobel Prize 2011).
Key features:
- Immature DCs in tissues: Phagocytic, sample their environment constantly via macropinocytosis
- Mature DCs after pathogen encounter: Migrate to lymph nodes, downregulate phagocytosis, upregulate MHC-II and costimulatory molecules (CD80, CD86) to activate naïve T cells
- Rich expression of PRRs - prime detectors of PAMPs and DAMPs
DC subtypes:
| Type | Function |
|---|---|
| Conventional DC1 (cDC1) | Cross-present to CD8+ T cells; produce IL-12; anti-viral/anti-tumor |
| Conventional DC2 (cDC2) | Present to CD4+ T cells; promote Th2/Th17 responses |
| Plasmacytoid DC (pDC) | Specialized producers of massive type I IFN in response to viral nucleic acids |
4. Mast Cells and Basophils
Tissue-resident (mast cells) and circulating (basophils) granular cells.
- Express FcεRI (high-affinity IgE receptor) - central to allergic responses
- Innate activation: Directly by complement (C3a, C5a), PAMPs via TLRs, and physical stimuli
- Release histamine, tryptase, prostaglandins, leukotrienes, TNF upon degranulation
- Important in defense against parasites and venoms
- Produce cytokines that activate ILC2 (IL-4, IL-13, IL-33)
5. Natural Killer (NK) Cells
NK cells are innate lymphoid effector cells from the CLP lineage. Discovered in the 1970s.
Key concept - "Missing Self" recognition:
- Normal healthy cells express MHC class I → delivers inhibitory signal to NK cells via KIR (Killer Immunoglobulin-like Receptors) and CD94/NKG2A → NK cell is inhibited
- Virus-infected or tumor cells downregulate MHC-I → loss of inhibitory signal → NK cell becomes activated
- Stressed cells upregulate NKG2D ligands (MICA, MICB, ULBP) → activating signal to NK cells
Killing mechanisms:
- Perforin/Granzyme pathway: Perforin forms pores; granzymes (serine proteases) enter and trigger apoptosis
- Fas-FasL interaction → apoptosis of target cell
- ADCC (Antibody-Dependent Cell Cytotoxicity): NK cells express CD16 (FcγRIII); bind antibody-coated target cells and kill
Cytokine production:
- NK cells produce large amounts of IFN-gamma → activates macrophages → enhanced killing of intracellular pathogens
6. Innate Lymphoid Cells (ILCs)
ILCs are tissue-resident lymphocytes from the CLP without antigen-specific receptors. Activated by cytokines, not antigens. Major innate sources of cytokines.
| Group | Activating Cytokines | Signature Cytokines Produced | Mirrors | Function |
|---|---|---|---|---|
| ILC1 | IL-12, IL-18 | IFN-gamma, TNF | Th1 | Anti-viral, anti-intracellular bacteria |
| ILC2 | IL-25, IL-33, TSLP | IL-4, IL-5, IL-13 | Th2 | Anti-helminth, allergic responses, tissue repair |
| ILC3 | IL-1beta, IL-23 | IL-17, IL-22 | Th17 | Mucosal barrier defense, anti-extracellular bacteria/fungi |
NK cells are considered cytotoxic ILCs (sometimes called ILC0 or group 1 cytotoxic ILCs).
7. Soluble Components
Complement System
The complement cascade is a series of plasma proteins activated in three pathways:
| Pathway | Trigger | Innate/Adaptive |
|---|---|---|
| Alternative | Spontaneous C3 hydrolysis on microbial surfaces | Innate |
| Lectin (MBL) | MBL/ficolin binds mannose/GlcNAc on microbes → MASP activation | Innate |
| Classical | C1q binds antibody-antigen complexes | Adaptive (mostly) |
All three converge at C3 convertase → C3 cleavage:
- C3b: Opsonin - coats microbes for phagocytosis (via CR1/CR3)
- C3a/C5a: Anaphylatoxins - mast cell degranulation, neutrophil chemotaxis (C5a is more potent)
- C5b-9 (MAC): Membrane Attack Complex - directly lyses gram-negative bacteria
Acute Phase Proteins
Produced by liver in response to IL-1, IL-6, TNF:
| Protein | Function |
|---|---|
| C-reactive protein (CRP) | Binds phosphocholine on bacteria/fungi; opsonin; activates classical complement |
| Mannose-binding lectin (MBL) | Opsonin; activates lectin complement pathway |
| Serum amyloid A (SAA) | Opsonin; recruits neutrophils/monocytes |
| Fibrinogen | Clotting; limits spread of infection |
| Hepcidin | Sequesters iron to limit bacterial growth |
Cytokines of Innate Immunity
| Cytokine | Source | Action |
|---|---|---|
| TNF | Macrophages, mast cells | Inflammation, fever, septic shock (at high levels) |
| IL-1β | Macrophages (inflammasome) | Fever, acute phase response, inflammation |
| IL-6 | Macrophages, DCs | Acute phase protein induction, T cell differentiation |
| IL-12 | Macrophages, DCs | NK cell activation, Th1 polarization |
| CXCL8 (IL-8) | Macrophages, epithelial cells | Neutrophil chemotaxis |
| IFN-alpha/beta | pDCs, virally infected cells | Antiviral state; MHC-I upregulation |
| IFN-gamma | NK cells, ILC1 | Macrophage activation |
Pattern Recognition Receptors (PRRs)
The molecular basis of innate immune recognition. PRRs detect conserved microbial structures (PAMPs) and endogenous danger signals from damaged cells (DAMPs).
Key principles (Janeway's "Danger Hypothesis"):
- PAMPs are evolutionarily conserved - essential for microbial survival, so microbes cannot easily mutate them
- ~100 different PRRs recognize thousands of molecular patterns
- PRRs are germline-encoded (non-rearranging) - unlike adaptive immune receptors
PRR Families and Their Locations:
Cellular compartments of PRRs - extracellular, endosomal, and cytosolic (Robbins & Kumar Basic Pathology)
A. Toll-Like Receptors (TLRs)
Discovered first in Drosophila melanogaster by Jules Hoffmann; homologs in mammals identified by Charles Janeway and Bruce Beutler (Nobel Prize 2011).
Mammals have 10 functional TLRs (TLR1-10 in humans). They are type I transmembrane proteins with extracellular leucine-rich repeat (LRR) domains and cytoplasmic TIR domains.
Location and Ligands:
| TLR | Location | Ligand | Pathogen |
|---|---|---|---|
| TLR1/2 (heterodimer) | Plasma membrane | Triacyl lipopeptides | Gram+ bacteria, mycobacteria |
| TLR2/6 (heterodimer) | Plasma membrane | Diacyl lipopeptides, LTA | Gram+ bacteria, mycoplasma |
| TLR4 | Plasma membrane | LPS (+ MD-2, CD14) | Gram- bacteria |
| TLR5 | Plasma membrane | Flagellin | Flagellated bacteria |
| TLR3 | Endosome | dsRNA | Viruses |
| TLR7 | Endosome | ssRNA | RNA viruses |
| TLR8 | Endosome | ssRNA | RNA viruses |
| TLR9 | Endosome | CpG unmethylated DNA | Bacteria, DNA viruses |
| TLR11/12 | Plasma membrane | Profilin, flagellin | Toxoplasma, bacteria |
TLR Signaling:
- All TLRs signal via adaptor proteins containing TIR domains
- MyD88 (used by all TLRs except TLR3) → NF-κB → pro-inflammatory cytokines (TNF, IL-6, IL-12)
- TRIF (used by TLR3, TLR4) → IRF3/IRF7 → Type I IFN (IFN-α/β) production
Clinical relevance:
- TLR4 mutations: Increased susceptibility to gram-negative sepsis
- TLR loss-of-function: Rare but serious immunodeficiency syndromes
- LPS signaling through TLR4 is the key driver of septic shock
B. NOD-Like Receptors (NLRs) and the Inflammasome
Cytosolic pattern recognition receptors. ~22 members in humans.
NOD1 and NOD2:
- NOD1: Detects DAP (diaminopimelic acid) from gram-negative bacteria
- NOD2: Detects MDP (muramyl dipeptide) from both gram+ and gram- bacteria
- Signal via RIPK2 → NF-κB activation
- NOD2 mutations: Associated with Crohn's disease (impaired barrier immunity)
The Inflammasome:
Several NLRs (especially NLRP3, also NLRC4, AIM2) form a multiprotein complex:
NLRP3 + ASC + pro-caspase-1 → INFLAMMASOME
↓
Caspase-1 (active)
↙ ↘
pro-IL-1β → IL-1β Gasdermin D cleavage
pro-IL-18 → IL-18 ↓
PYROPTOSIS
(inflammatory cell death)
NLRP3 activating signals:
- Crystals: Monosodium urate (gout), calcium pyrophosphate (pseudogout), cholesterol crystals (atherosclerosis)
- Particulates: Silica, asbestos, amyloid fibrils (Alzheimer's)
- Metabolic signals: Fatty acids (obesity, metabolic syndrome)
- Potassium efflux, ROS, lysosomal damage
Clinical importance:
- Gain-of-function NLRP3 mutations: Cryopyrin-associated periodic syndromes (CAPS) - treated with IL-1 antagonists (anakinra, canakinumab)
- Gout: NLRP3 activated by urate crystals
- Type 2 diabetes: NLRP3 activation by islet amyloid polypeptide (IAPP)
- Atherosclerosis: Cholesterol crystal activation of NLRP3
C. RIG-I-Like Receptors (RLRs)
Cytosolic RNA sensors that detect viral RNA during replication.
| Receptor | Ligand |
|---|---|
| RIG-I (Retinoic Acid-Inducible Gene I) | 5'-triphosphate dsRNA, short dsRNA (most RNA viruses) |
| MDA5 (Melanoma Differentiation-Associated protein 5) | Long dsRNA, picornaviruses |
| LGP2 | Regulates RIG-I and MDA5 signaling |
Signaling:
RIG-I/MDA5 activation → binds MAVS (Mitochondrial Antiviral Signaling protein, also called IPS-1/VISA) on outer mitochondrial membrane → TBK1 → IRF3/IRF7 phosphorylation → Type I IFN (IFN-α/β) production
Many viruses evade this pathway by encoding proteases that cleave MAVS (e.g., hepatitis C NS3/4A protease).
D. cGAS-STING Pathway
Cytosolic DNA sensor - most recently characterized innate pathway.
cGAS (cyclic GMP-AMP Synthase): Detects cytosolic dsDNA (from viruses, bacteria, or aberrant self-DNA)
Signaling:
Cytosolic dsDNA → cGAS activated
↓
cGAMP synthesis (2'3'-cGAMP)
↓
STING (on ER membrane) activated
↓
TBK1 → IRF3 → IFN-α/β
also → NF-κB → inflammation
Sources of activating cytosolic DNA:
- Viral DNA (HSV, HIV, CMV)
- Bacterial DNA (Mycobacterium tuberculosis, Listeria)
- Mitochondrial DNA released by stressed cells
- Nuclear DNA from cells with DNA damage
Clinical relevance:
- Interferonopathies (Aicardi-Goutieres syndrome): Mutations in DNases that clear cytosolic self-DNA → chronic cGAS-STING activation → excessive IFN production
- STING gain-of-function: STING-associated vasculopathy with onset in infancy (SAVI)
- cGAS-STING is a therapeutic target for autoimmunity, cancer immunotherapy, and antiviral drugs
E. C-Type Lectin Receptors (CLRs)
Transmembrane receptors on macrophages and DCs that recognize microbial carbohydrates:
| Receptor | Ligand | Function |
|---|---|---|
| Dectin-1 | β-1,3-glucan (fungi) | Key receptor for antifungal immunity; activates SYK signaling |
| Dectin-2 | α-mannans (fungi, bacteria) | Pro-inflammatory cytokines |
| Mannose receptor (MRC1) | Mannose, fucose, GlcNAc | Phagocytosis; antigen presentation |
| DC-SIGN (CD209) | Mannose-rich glycans | Pathogen capture; HIV attachment |
| Mincle | Trehalose dimycolate (M. tuberculosis) | Macrophage activation |
Dectin-1 deficiency: Susceptibility to mucocutaneous candidiasis and invasive fungal infections.
F. Other Cytosolic Sensors
- AIM2 (Absent in Melanoma 2): Detects cytosolic dsDNA → forms AIM2 inflammasome → caspase-1 → IL-1β/IL-18. Activated by Francisella tularensis and vaccinia virus
- G protein-coupled receptors (GPCRs): Detect fMLP (N-formylmethionyl peptides from bacterial proteins); drive neutrophil chemotaxis (bacteria use fMet to initiate proteins; mammalian cytoplasmic translation does not)
- Scavenger receptors: SR-A, CD36 - recognize oxidized lipids, apoptotic cells, bacterial LTA; promote phagocytosis
Reactions of Innate Immunity
1. Inflammation
The cardinal response to infection or tissue injury:
Vascular phase:
- Vasodilation → increased blood flow (redness, heat)
- Increased vascular permeability → edema (swelling)
- Driven by: histamine (mast cells), C3a/C5a, bradykinin, prostaglandins
Cellular phase:
- Neutrophil recruitment (minutes-hours): CXCL8, C5a, LTB4
- Monocyte/macrophage recruitment (hours-days): CCL2 (MCP-1)
- Adhesion cascade: Selectins → rolling; integrins (LFA-1/ICAM-1) → firm adhesion → transmigration
Systemic effects (acute phase response):
- Fever: IL-1β, IL-6, TNF act on hypothalamus → PGE2 → elevated set point
- Acute phase proteins: CRP, MBL, fibrinogen, SAA - opsonins, complement activators
- Leukocytosis: IL-1β, G-CSF release neutrophils from bone marrow
- Hepatocyte production of acute phase proteins (upregulation of CRP, fibrinogen; downregulation of albumin, transferrin)
2. Antiviral Defense (Type I Interferon Response)
IFN-α/β are the principal antiviral cytokines of innate immunity:
Produced by: pDCs (IFN-α massive production), all virally infected cells (IFN-β)
Actions on cells (via JAK-STAT signaling):
- Upregulate ISGs (Interferon-Stimulated Genes)
- Activate OAS/RNase L → degrade viral RNA
- Activate PKR (protein kinase R) → phosphorylate eIF2α → halt protein translation
- Upregulate MHC class I → better recognition by cytotoxic T cells
- Activate NK cells → enhanced killing of infected cells
Type III IFNs (IFN-λ): Functionally similar to type I but restricted to mucosal epithelia; important in respiratory and GI antiviral defense.
3. Activation of Adaptive Immunity
Innate immunity generates three critical signals that prime adaptive responses:
| Signal | Source | Effect |
|---|---|---|
| Signal 1 (Antigen) | DCs process and present peptides on MHC-II/-I | T cell TCR engagement |
| Signal 2 (Costimulation) | TLR activation upregulates CD80/CD86 on DCs | CD28 on T cells → T cell activation (without this, T cells become anergic) |
| Signal 3 (Cytokines) | IL-12 → Th1; IL-4 → Th2; IL-6+IL-23 → Th17; IL-10 → Treg | Polarizes T helper subset differentiation |
This explains why adjuvants (which activate TLRs) are required for effective vaccines - they provide Signal 2 that would otherwise only come from natural infection.
Innate Immune Evasion by Pathogens
| Pathogen | Mechanism |
|---|---|
| S. aureus | Protein A binds IgG Fc; CHIPS blocks C5a receptor; catalase neutralizes H₂O₂ |
| M. tuberculosis | Inhibits phagosome-lysosome fusion; LAM blocks IFN-γ signaling |
| Influenza virus | Neuraminidase cleaves mucus; NS1 protein blocks RIG-I signaling |
| HIV | Vpr degrades SAMHD1 (innate restriction factor); Vif degrades APOBEC3G |
| Yersinia spp. | Injects Yop effectors via type III secretion; inactivates TLR signaling |
| Herpes simplex | ICP47 blocks TAP → prevents antigen loading onto MHC-I |
Clinical Correlations and Immunodeficiencies
| Defect | Disease | Consequence |
|---|---|---|
| NADPH oxidase mutations | Chronic Granulomatous Disease (CGD) | Recurrent bacterial/fungal infections; catalase-positive organisms |
| NLRP3 gain-of-function | CAPS (FCAS, MWS, NOMID) | Autoinflammatory; responds to anakinra/canakinumab |
| NOD2 mutations | Crohn's disease | Impaired mucosal innate immunity |
| TLR signaling (IRAK-4, MyD88) | Pyogenic bacterial infections | Gram+ sepsis in infancy |
| NK cell deficiency | Severe herpesvirus infections | HSV, EBV, CMV dissemination |
| Dectin-1/CARD9 mutations | Susceptibility to fungal infections | Candidiasis, aspergillosis |
| cGAS-STING dysregulation | Interferonopathies | Aicardi-Goutieres, SAVI |
| Complement C3 deficiency | Recurrent encapsulated bacteria | Streptococcus pneumoniae, H. influenzae |
| C5-C9 deficiency (MAC) | Neisseria infections | Recurrent meningococcal/gonococcal sepsis |
Summary: The Innate Immune System as an Integrated Network
MICROBE INVADES
↓
Epithelial barriers breached
↓
PAMPs/DAMPs recognized by PRRs on:
• Macrophages / DCs (TLRs, CLRs, NLRs, cGAS)
• Neutrophils (TLRs, GPCRs)
• Epithelial cells (TLRs, RLRs)
↓
┌──────────────────────────────┐
↓ ↓
NF-κB activation IRF3/IRF7 activation
↓ ↓
Pro-inflammatory Type I IFN production
cytokines (TNF, IL-1, (IFN-α/β)
IL-6, IL-12, CXCL8) ↓
↓ Antiviral state
Inflammation NK cell activation
(neutrophil/monocyte ↓
recruitment) Infected cell killing
↓
NK cells, ILCs → effector killing / cytokine amplification
↓
DC maturation + migration to lymph nodes
↓
ADAPTIVE IMMUNITY ACTIVATED
Sources:
- Janeway's Immunobiology 10e - Chapters 1 & 3 (Garland Science/Norton)
- Cellular and Molecular Immunology, Abbas, Lichtman & Pillai - Chapters 1 & 4
- Robbins, Cotran & Kumar Pathologic Basis of Disease - Chapter 6
- Robbins & Kumar Basic Pathology - Chapter 5
This is a shared conversation. Sign in to Orris to start your own chat.