What are the main question and answers for a pediatric head injury burn or suturing case
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching the Web
pediatric burn assessment Rule of Nines Lund Browder child TBSA depth classification
Searching the Web
pediatric laceration suturing technique wound closure questions answers medical student exam
Searching the Web
Parkland formula burns pediatric TBSA fluid resuscitation Lund Browder vs Rule of Nines
Layers of the scalp
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is a complete breakdown of the layers of the scalp, sourced directly from Gray's Anatomy for Students and Roberts & Hedges' Clinical Procedures in Emergency Medicine.
Layers of the Scalp - Mnemonic: SCALP
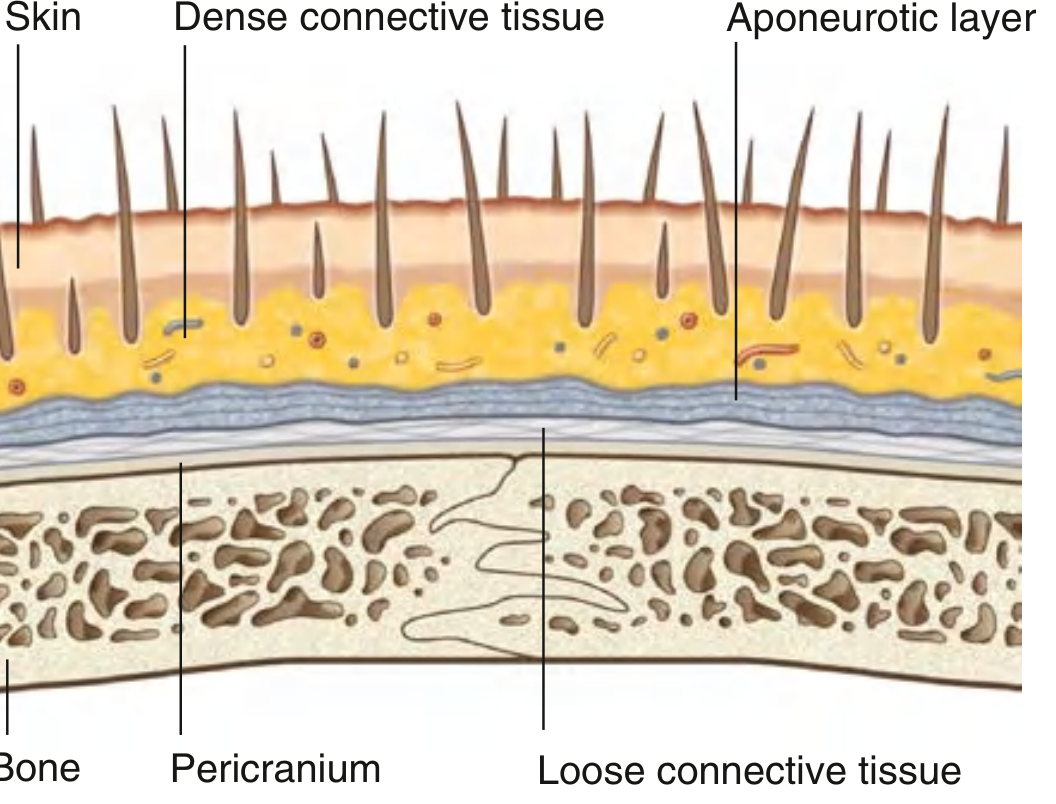
1. S - Skin
- The outermost layer
- Similar to skin elsewhere but bears hair follicles over most of its surface
- Contains sebaceous glands and sweat glands
2. C - Connective Tissue (Dense, subcutaneous)
- Lies deep to the skin; anchors skin firmly to the galea below
- Contains all the arteries, veins, and nerves supplying the scalp
- The fibrous septa surrounding vessels hold cut vessels open, preventing normal retraction - this is why scalp wounds bleed profusely
- Clinically: even a small laceration in this layer can cause significant hemorrhage
3. A - Aponeurosis (Galea Aponeurotica / Epicranial Aponeurosis)
- The tendinous sheet connecting the frontal belly (anteriorly) and occipital belly (posteriorly) of the occipitofrontalis muscle
- Together, layers 1-3 are firmly adherent and move as a single unit - called the "scalp proper"
- This is the tissue avulsed in "scalping" injuries
- Clinical key: a wound that gapes open = the galea has been cut. This requires separate suturing of the galea to achieve hemostasis and prevent infection spreading intracranially
4. L - Loose Areolar (Connective) Tissue
- A potential space between the galea and pericranium
- Allows the scalp proper to move freely over the skull
- Contains emissary veins - valveless veins draining through diploic channels into the intracranial venous sinuses
- Called the "danger zone" of the scalp:
- Infections here can spread rapidly across the entire scalp
- Bacteria can be carried via emissary veins to cause meningitis, osteomyelitis, or brain abscess
- Blood from trauma collects here as a subgaleal hematoma
5. P - Pericranium (Periosteum of skull)
- The deepest layer; periosteum covering the outer surface of the calvaria
- Firmly adherent at suture lines of the skull (hence subperiosteal collections are limited by suture lines - as in cephalhematoma)
- Thin and flimsy - cannot hold sutures; often mistaken for the galea clinically
- Can be elevated off the bone except at suture lines
Key Clinical Correlations
| Layer | Clinical Point |
|---|---|
| Dense connective tissue (C) | Reason for profuse scalp bleeding - vessels cannot retract |
| Galea (A) | Gaping wound = galea cut; must suture galea separately |
| Loose areolar tissue (L) | "Danger zone" - infection/blood spreads widely; emissary veins link to dural sinuses |
| Pericranium (P) | Cephalhematoma is subperiosteal - limited by suture lines (vs. caput succedaneum which crosses sutures) |
Blood Supply
The scalp has a rich anastomotic supply from both internal and external carotid systems, entering peripherally and running toward the vertex. Branches include:
- Supratrochlear and supraorbital (from ophthalmic branch of internal carotid)
- Superficial temporal, posterior auricular, and occipital arteries (from external carotid)
Innervation
- Anterior to vertex: branches of CN V (trigeminal) - supratrochlear, supraorbital, zygomaticotemporal, auriculotemporal nerves
- Posterior to vertex: cervical nerves - lesser occipital (C2), greater occipital (C2/C3), third occipital (C3)
- Motor (occipitofrontalis): facial nerve CN VII
Sources: Gray's Anatomy for Students, p. 1062-1063 | Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 814
This is a shared conversation. Sign in to Orris to start your own chat.