Reading File
Running Command
cd /home/daytona/workspace && python3 -c " import pdfplumber pdf_path = '/home/…
Running Command
cd /home/daytona/workspace && python3 -c " from pdf2image import convert_from_pa…
analyse_media
Running Command
cd /home/daytona/workspace && python3 -c " import base64, json with open('/home…
Running Command
cd /home/daytona/workspace && python3 -c " import pytesseract from PIL import Im…
Running Command
cd /home/daytona/workspace && python3 -c " from PIL import Image # Resize and c…
Reading File
Running Command
cd /home/daytona/workspace && python3 -c " from PIL import Image import os # Ma…
Reading File
Now I can see the image clearly. This is a medical/clinical slide showing 4 facial masks (theater-style painted masks) arranged in a 2x2 grid against a black background. This appears to be from a medical context - likely related to facial palsy or Bell's palsy demonstration, or possibly related to Sturge-Weber syndrome, hemifacial conditions, or a neurology/dermatology teaching slide by "Sri Sir."
The slide (labeled SLIDE14-6) shows four white painted theatrical-style faces/masks with:
- Black eyebrows and eyeliner
- Red lips
- Orange/skin-toned coloring
- Each mask appears slightly different - some showing asymmetry, drooping, or distortion of facial features
This is a medical teaching image. Given the context of "SRI SIR SLIDE14-6," this is likely from a dermatology or neurology lecture series. The masks appear to demonstrate facial asymmetry or pathological facial changes - the lower two masks show more distortion/asymmetry compared to the upper two.
This looks like it could be illustrating leprosy facies (leonine facies), facial nerve palsy grading, or scleroderma/morphea facial changes using theatrical masks as a teaching tool.
Here is what the slide contains:
The PDF (SLIDE14-6) is a single-page image showing four painted theatrical/drama masks arranged in a 2x2 grid on a black background. The masks are white with skin-toned (peach/orange) coloring, black eyebrows, black eyeliner, and red lips.
What the image likely illustrates:
This appears to be a medical teaching slide (from "Sri Sir's" lecture series, slide 14-6) using theatrical masks to demonstrate progressive facial changes or facial asymmetry seen in a clinical condition. The four masks show:
- Top left & top right: More symmetrical, intact-looking faces
- Bottom left: Shows a long black line/streak running from the eye down to the lip area (possibly illustrating a scar, nerve line, or "en coup de sabre" morphea)
- Bottom right: Shows more distortion, with the face appearing more damaged/irregular
Most likely clinical context: This slide is likely demonstrating linear morphea (en coup de sabre) or hemifacial atrophy (Parry-Romberg syndrome) - conditions that cause progressive unilateral facial wasting/disfigurement. The theatrical masks are being used to visualize how facial contour changes over time or across severity grades.
It could also relate to leprosy facies, facial nerve palsy grading (House-Brackmann scale), or scleroderma.
Could you let me know what subject/topic this lecture series covers? That would help me give you a more precise interpretation of what these four masks are illustrating. If you have additional slides from the same series, those would also provide context.
Face developmental anomalies
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive answer. Here is the full explanation:
Facial Developmental Anomalies
About the Slide (SLIDE14-6)
The four theatrical masks in your slide are a teaching tool used to demonstrate facial clefting anomalies - each mask representing a different type or severity of cleft defect affecting the lip, jaw, and palate. The masks mimic the visual appearance of these conditions on a full face.
Normal Face Development (Embryological Basis)
The face forms between weeks 4-8 from five facial prominences that grow around the stomodeum (primitive mouth) and must fuse correctly:
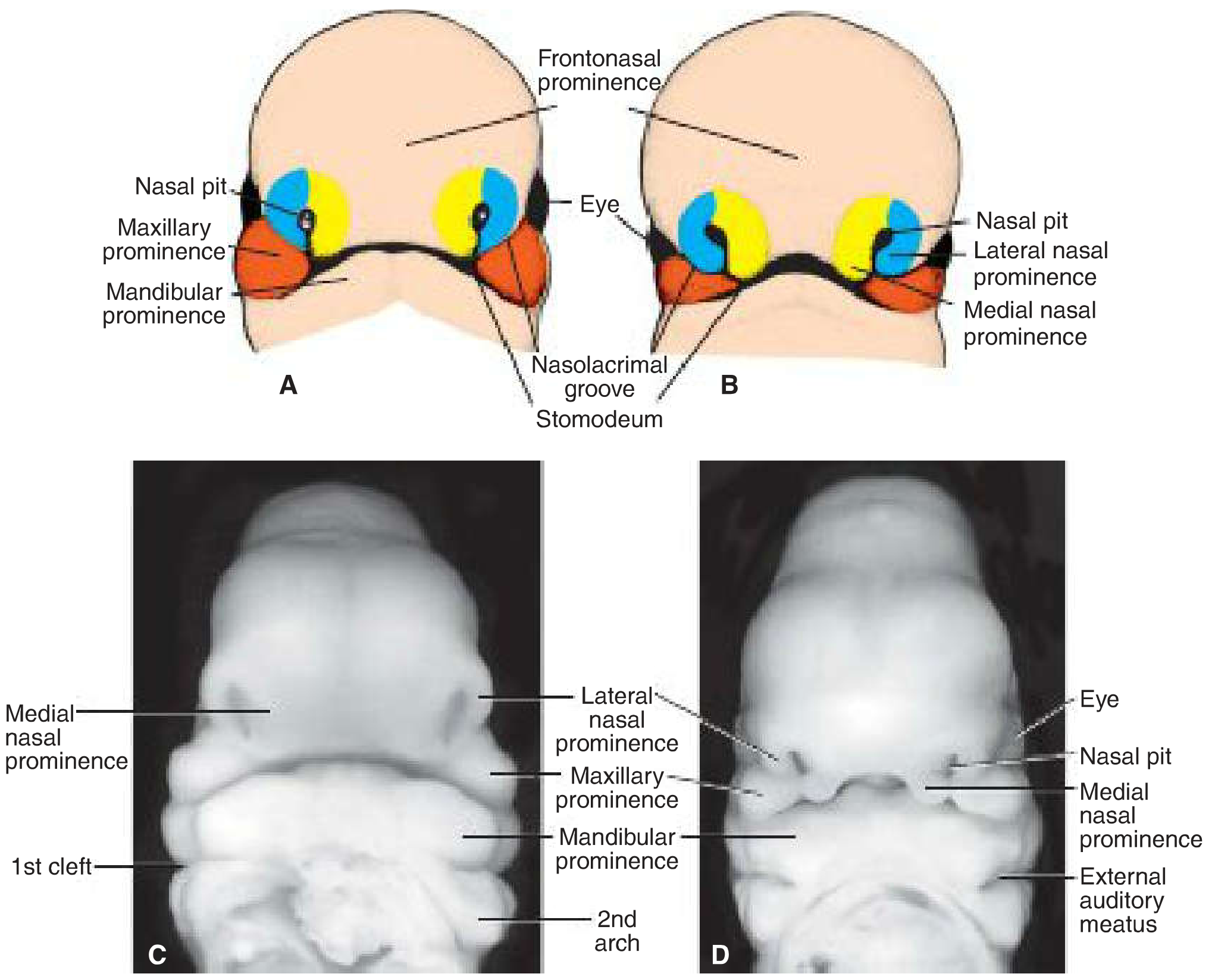
| Prominence | Structures it forms |
|---|---|
| Frontonasal | Forehead, bridge of nose, medial & lateral nasal prominences |
| Medial nasal | Philtrum of upper lip, premaxilla, nasal tip & septum |
| Lateral nasal | Alae of nose |
| Maxillary | Cheeks, lateral upper lip, secondary palate |
| Mandibular | Lower jaw, lower lip |
Fusion of the maxillary prominence with the medial nasal prominence on each side forms the upper lip. Failure of this fusion = cleft lip.
The Incisive Foramen: Key Landmark for Classification
All facial clefts are classified relative to the incisive foramen:
- Anterior clefts (anterior to incisive foramen): cleft lip, cleft upper jaw/alveolus
- Posterior clefts (posterior to incisive foramen): cleft secondary palate, cleft uvula
- Combined: both anterior and posterior components
Types of Facial Clefts
1. Cleft Lip (Cheiloschisis)
Mechanism: Failure of the maxillary prominence to fuse with the merged medial nasal prominences. The labial groove persists, epithelium stretches and breaks down, dividing the lip into medial and lateral parts.
- Unilateral cleft lip - one side fails to fuse (more common; ~1 in 1000 births, 60-80% male)
- Bilateral cleft lip - both sides fail
- A partial bridge of tissue called the Simonart band may connect parts in incomplete clefts
- Severity ranges from a notch in the vermilion border to a complete cleft extending into the nostril
2. Cleft Palate (Palatoschisis)
Mechanism: Failure of the lateral palatine shelves to elevate, meet, and fuse during weeks 7-12. Causes include:
-
Shelves too small
-
Failure to elevate horizontally
-
Inhibition of fusion
-
Tongue fails to drop (micrognathia)
-
Cleft uvula - mildest form (bifid uvula), isolated failure at the posterior tip
-
Partial cleft palate - soft palate only
-
Complete cleft palate - extends through soft and hard palate to incisive foramen
3. Combined Cleft Lip + Cleft Palate
The most severe form. A complete unilateral or bilateral cleft can extend from the lip through the alveolus, through the incisive foramen, and all the way back through the hard and soft palate.
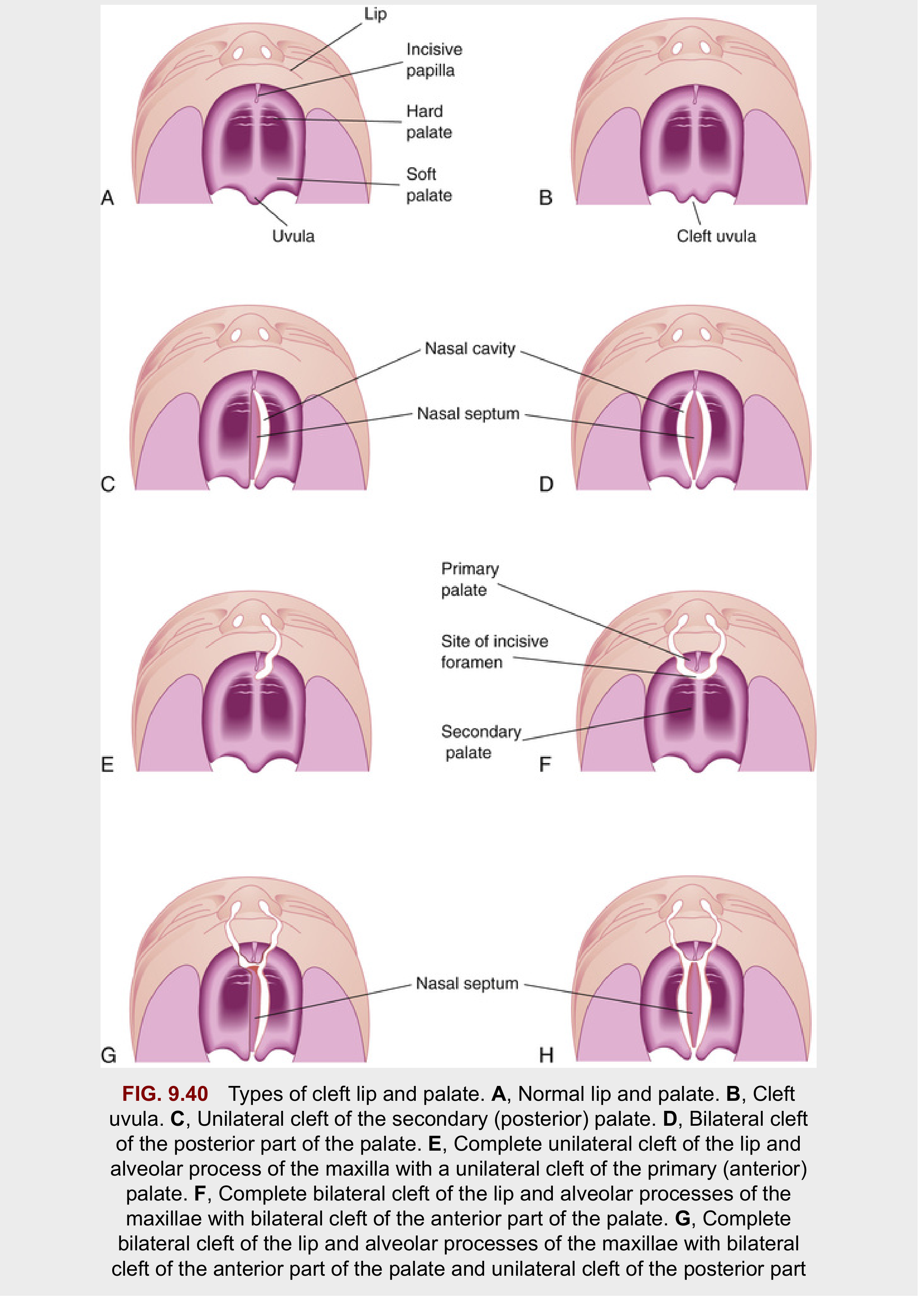
(A = normal; B = cleft uvula; C = unilateral posterior palate cleft; D = bilateral posterior cleft; E = complete unilateral cleft lip+jaw with anterior palate cleft; F = complete bilateral cleft lip+jaw with bilateral anterior palate cleft; G & H = most severe combined forms)
4. Median Cleft Lip (Rare)
Mechanism: Incomplete merging of the two medial nasal prominences in the midline (different from lateral cleft lip which involves the maxillary prominence). Associated with brain defects (holoprosencephaly) and cognitive impairment. Caused by:
- Mutations in SHH (Sonic Hedgehog) gene
- Altered cholesterol biosynthesis
- Teratogens like alcohol in week 3
5. Oblique Facial Cleft
Runs from the lip toward the eye along the nasolacrimal groove (between lateral nasal and maxillary prominences). Rare.
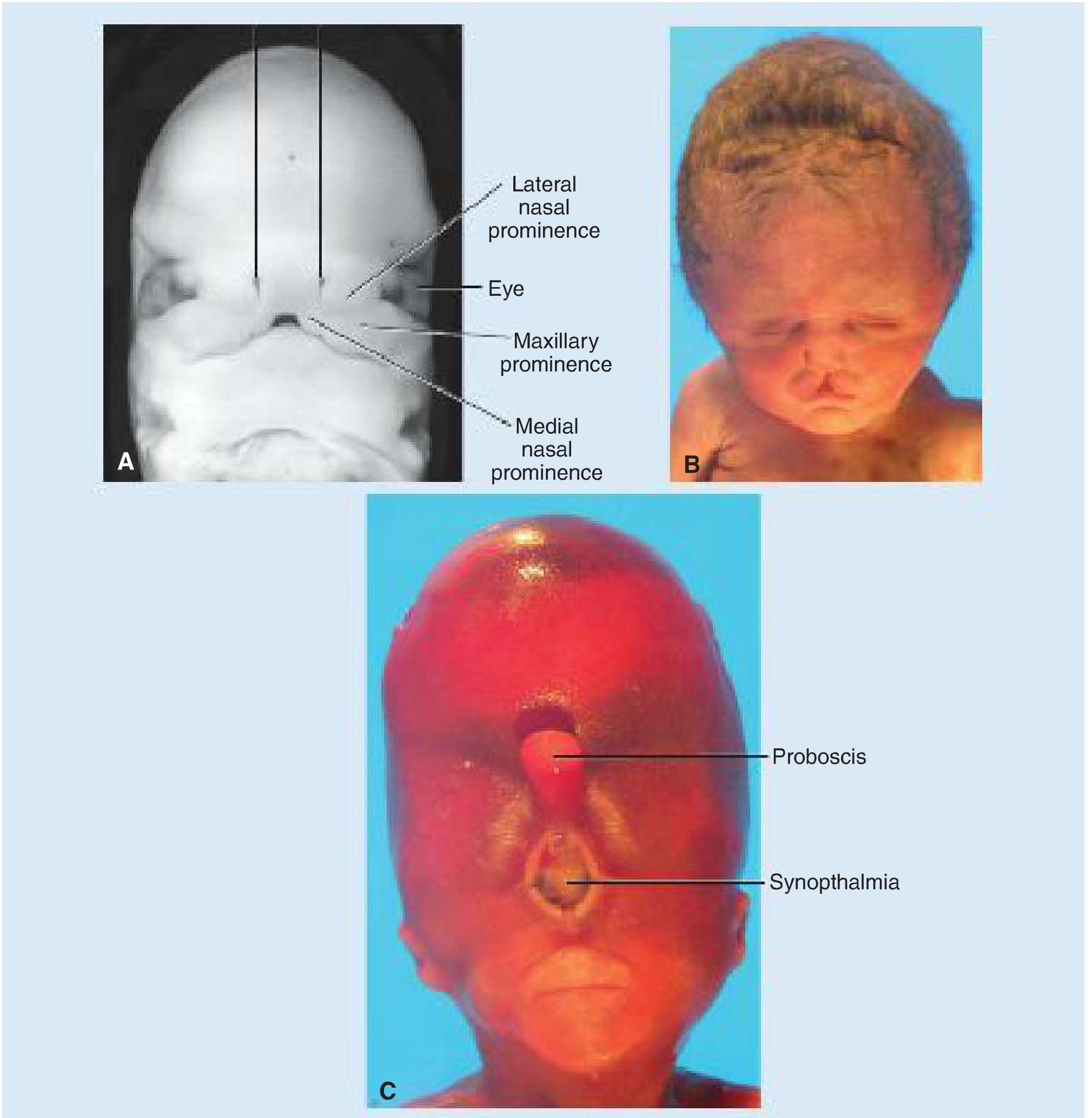
6. Holoprosencephaly with Proboscis + Synophthalmia
The extreme end - massive midline tissue deficiency causing:
- Fusion of both eyes into one (synophthalmia/cyclopia)
- A single tube-like nose (proboscis)
- Single forebrain ventricle
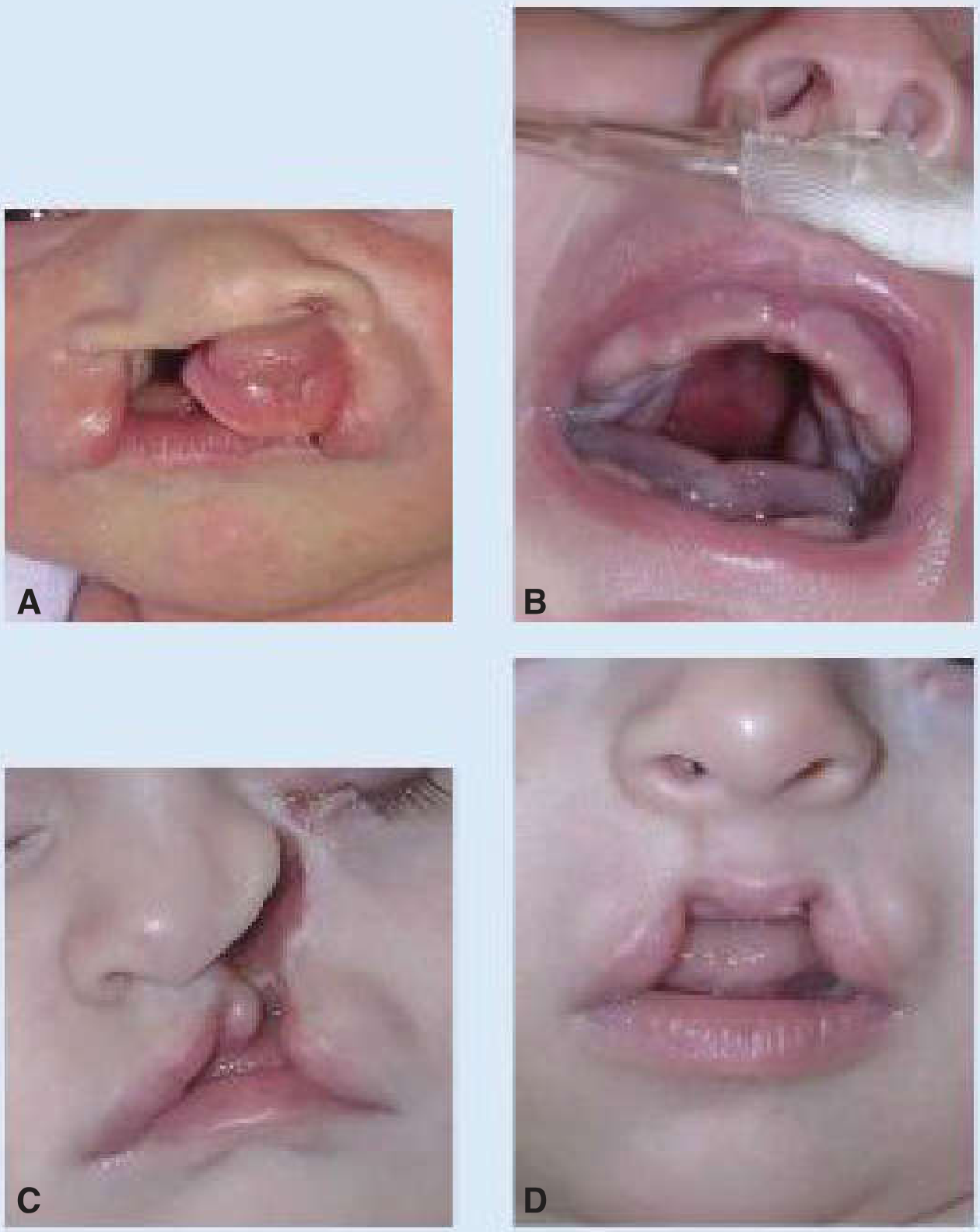
Clinical Photographs
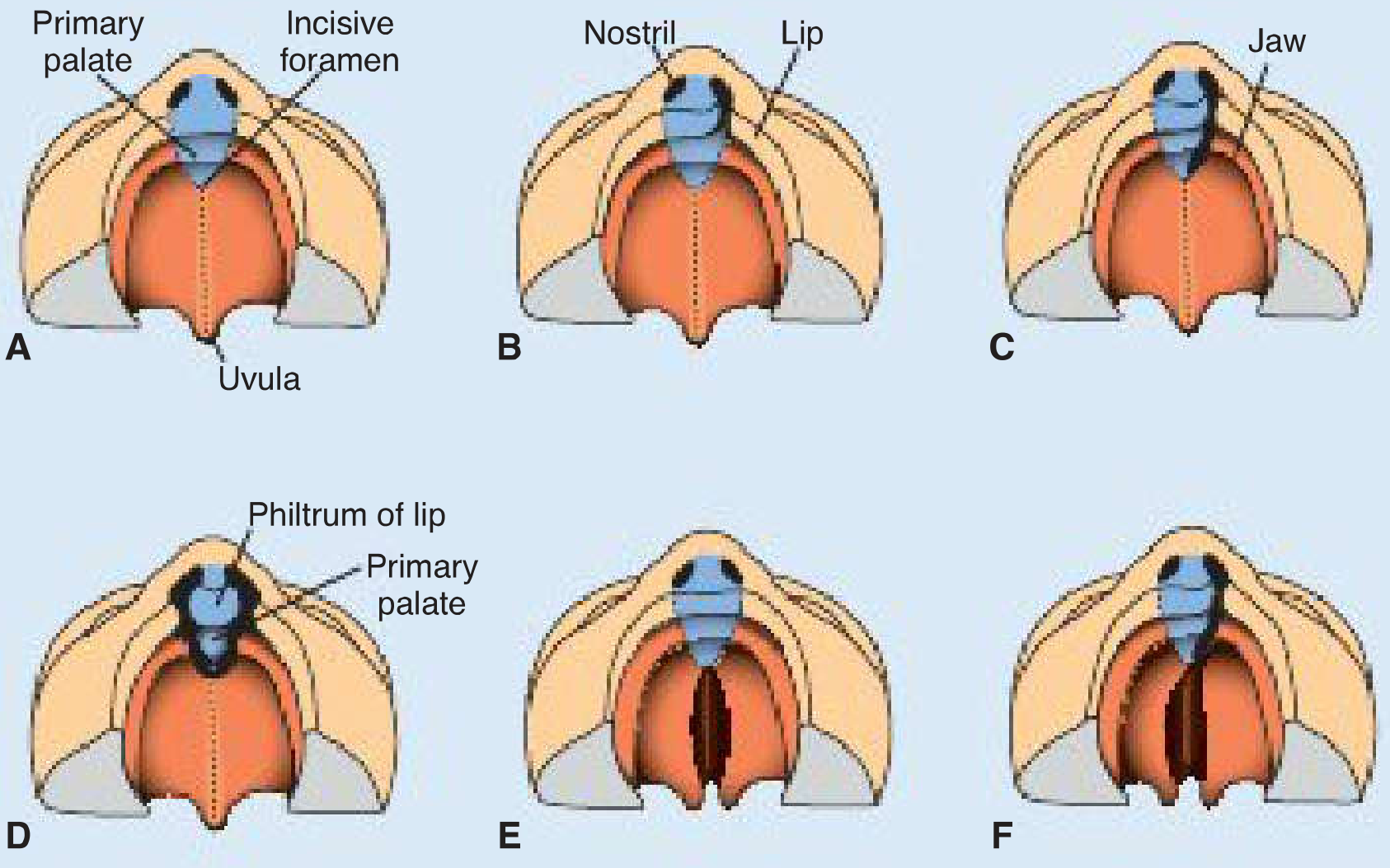
(A = normal; B = unilateral cleft lip into nostril; C = unilateral cleft through lip and jaw; D = bilateral cleft lip; E = isolated cleft palate; F = cleft palate + unilateral anterior cleft lip)
(A = bilateral cleft lip, B = cleft palate, C = oblique facial cleft, D = midline cleft lip)
Epidemiology & Etiology
| Feature | Cleft Lip ± Palate | Isolated Cleft Palate |
|---|---|---|
| Incidence | ~1/700 births | ~1/1500 births |
| Sex | More in males (65%) | More in females (55%) |
| Ethnicity | Highest: Asian, Native American (3.5/1000); Lowest: African American (1/1000) | - |
Risk factors:
- Genetic: Mutations in IRF6 (Van der Woude syndrome - most common associated syndrome, autosomal dominant), MSX1, SHH
- Teratogens: Valproic acid (anticonvulsant), alcohol, cigarette smoking
- Most cases are multifactorial
Summary: The Four Masks in the Slide
The 2x2 arrangement of masks likely represents:
- Top left - Normal face (reference)
- Top right - Unilateral cleft lip (one side)
- Bottom left - Unilateral cleft lip extending to nostril (complete anterior cleft), shown by the long black line running from eye/nostril to lip
- Bottom right - Bilateral or more severe combined cleft (both sides affected, more distorted appearance)
These are teaching masks used to show how facial fusion defects appear on the surface of the face, corresponding to different failure points in the fusion of facial prominences during weeks 4-8 of embryogenesis.
Sources: The Developing Human: Clinically Oriented Embryology, p.537-544; Langman's Medical Embryology, p.322-327
This is a shared conversation. Sign in to Orris to start your own chat.