Subacute degeneration of spinal cord with vit b12 deficiency presentation and management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"subacute combined degeneration" AND "vitamin B12"
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have an extensive set of high-quality textbook data. Here is the full, well-organized answer:
Subacute Combined Degeneration (SCD) of the Spinal Cord
What Is It?
Subacute combined degeneration (SCD) is a metabolic myelopathy caused by severe vitamin B12 (cobalamin) deficiency. It is the most common form of metabolic myelopathy. The name "combined" refers to simultaneous degeneration of both the posterior columns (dorsal) and the lateral columns (corticospinal tracts) of the spinal cord - hence the combined posterior + lateral tract syndrome.
Pathophysiology
Two cobalamin-dependent biochemical reactions underlie the neurological damage:
-
Methionine synthesis: Cobalamin is a cofactor for methionine synthase, which converts homocysteine to methionine. Methionine is then converted to S-adenosylmethionine (SAM), which is essential for methylation reactions in the nervous system - including myelin maintenance.
-
Methylmalonyl-CoA conversion: Cobalamin is needed to convert methylmalonyl-CoA to succinyl-CoA. When blocked, methylmalonic acid accumulates.
When cobalamin is deficient, SAM synthesis fails, methylation of myelin basic protein is impaired, and demyelination begins - initially spongiform vacuolar changes, progressing to frank axon destruction. The most severely affected regions are the posterior columns at the cervical and upper thoracic levels, followed by the lateral columns (Fig. 1 below).

Causes of B12 Deficiency
| Mechanism | Examples |
|---|---|
| Pernicious anemia (most classic) | Autoimmune gastritis - anti-parietal cell antibodies, anti-intrinsic factor antibodies - loss of intrinsic factor |
| Dietary deficiency | Strict vegans/vegetarians (B12 is found only in animal products) |
| Food-cobalamin malabsorption | Atrophic gastritis, H. pylori, hypochlorhydria, gastrectomy |
| Drug-induced malabsorption | Prolonged PPI, H2 blockers, metformin use |
| Ileal disease | Crohn's disease, surgical resection of terminal ileum |
| Nitrous oxide (N2O) inhalation | Recreational ("whippets") or operative exposure - N2O irreversibly inhibits methionine synthase; patients who are already B12-deficient can develop SCD after a single brief anaesthetic exposure |
| Intestinal bacterial overgrowth | Competes for B12 |
- Bradley & Daroff's Neurology, p. 1797; Harrison's 22E, p. 3612
Clinical Presentation
Onset and Pattern
- Onset is insidious and subacute
- Symptoms are typically symmetric and diffuse (not focal)
- The myelopathy is usually ascending
Symptoms (Approximate Order of Appearance)
1. Sensory symptoms (earliest and most common)
- Paresthesias (tingling, numbness) in the hands and feet - symmetric, stocking-glove
- Loss of vibration sense and proprioception (posterior column dysfunction)
- Positive Romberg sign
- Lhermitte's sign may be present (electric shock sensation down the spine on neck flexion)
2. Motor symptoms
- Progressive leg weakness
- Spastic gait (pyramidal tract involvement - lateral columns)
- Ranging from mild clumsiness to frank spastic paraplegia
3. Reflex findings (classic diagnostic clue)
- Loss of deep tendon reflexes (due to peripheral neuropathy) combined with upgoing plantars / Babinski sign (due to corticospinal tract involvement) - this combination of areflexia + Babinski is a highly characteristic finding
- Hyperreflexia may also occur when UMN > LMN involvement
4. Cognitive/psychiatric symptoms
- Mental slowing, depression, irritability
- Confusion, delusions, hallucinations ("megaloblastic madness")
- May occasionally be the presenting feature in advanced disease
5. Visual symptoms
- Bilateral visual loss, optic atrophy, centrocecal scotomata (optic nerve involvement)
- May precede other neurological symptoms
6. Autonomic features
-
Bladder dysfunction (rare)
-
Brainstem/cerebellar signs rarely occur
-
Harrison's 22E, p. 3612; Bradley & Daroff, p. 1797-1798
Investigations
Haematological
- Macrocytic (megaloblastic) anaemia - macrocytosis, hypersegmented neutrophils
- Important: haematological changes may be absent at the time of neurological presentation - their absence does NOT rule out SCD
Biochemistry
| Test | Finding | Notes |
|---|---|---|
| Serum B12 | Low (<200 pg/mL diagnostic; 200-350 pg/mL borderline) | May be falsely normal in myeloproliferative disorders, falsely low in pregnancy |
| Methylmalonic acid (MMA) | Elevated | More specific - elevated in B12 deficiency, NOT folate deficiency |
| Homocysteine | Elevated | Elevated in both B12 AND folate deficiency |
| Anti-intrinsic factor Ab | Positive in pernicious anemia | Low sensitivity (50-70%) but high specificity |
| Anti-parietal cell Ab | Often positive | Nonspecific |
| Serum gastrin | Elevated | Sensitive (~90%) but nonspecific marker of atrophic gastritis |
| Holotranscobalamin | May be low | Better marker of functional B12 deficiency than total B12 |
- MMA + homocysteine are especially useful when serum B12 is in the borderline range (200-350 pg/mL)
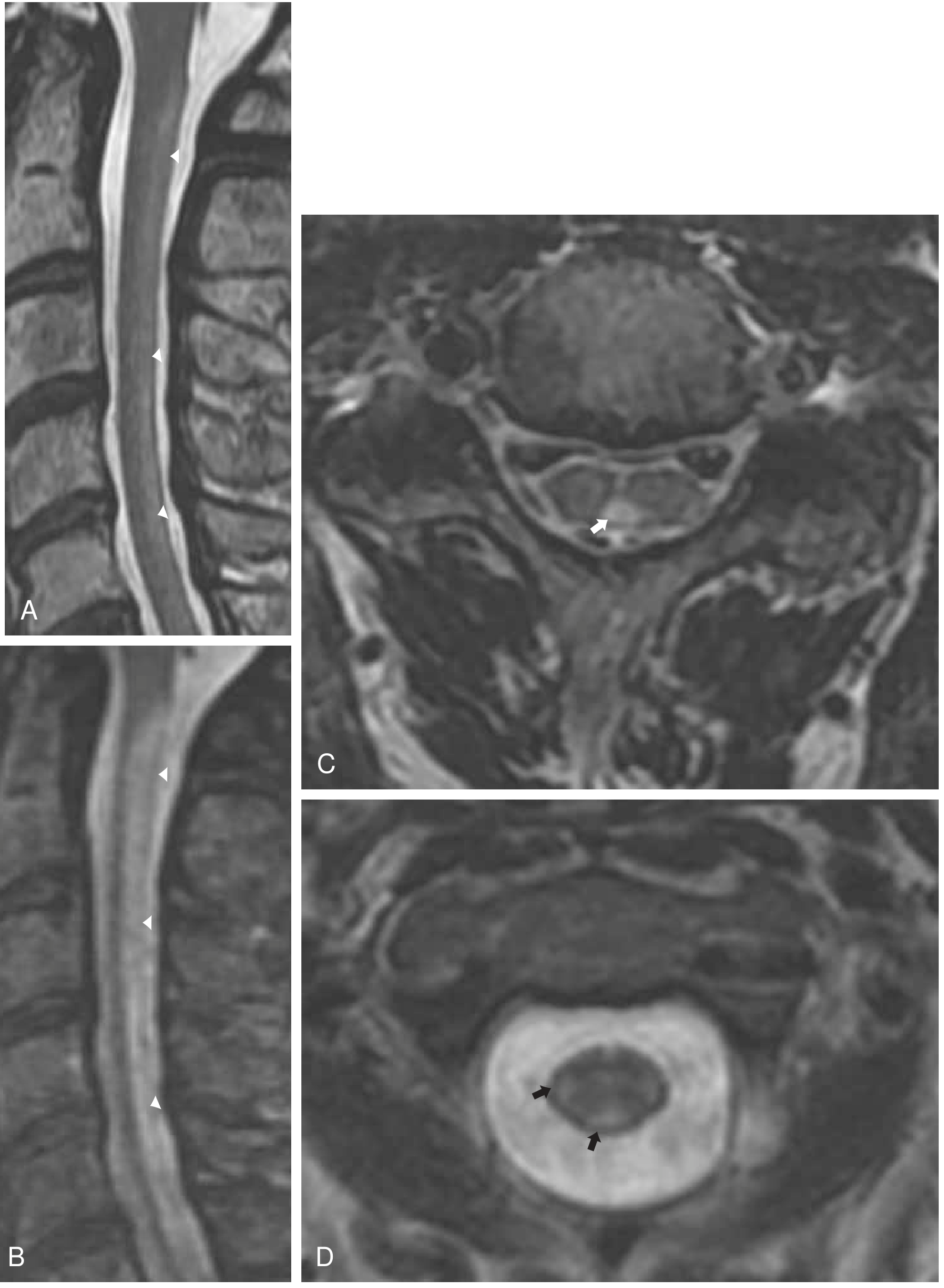
MRI Spinal Cord (imaging of choice)
- T2-weighted: hyperintense signal in the posterior and lateral columns, typically at cervical/upper thoracic levels
- "Inverted V sign" or "trident sign" on axial T2 - posterior column high signal
- T1-weighted: may show hypointensity in dorsal columns, mild cord enlargement
- Gadolinium enhancement may be present (as in Bradley's Fig. 85.1 case)
- MRI may be normal early in the disease
Other Investigations
- Nerve conduction studies: small or absent sural nerve sensory potentials (axonal polyneuropathy in ~50%)
- Somatosensory and visual evoked potentials: may show nonspecific abnormalities
- Diffusion tensor imaging (DTI): more sensitive for white matter changes correlating with cognitive dysfunction
Differential Diagnosis
| Condition | Key Distinguishing Feature |
|---|---|
| Copper deficiency myelopathy | Clinically identical to SCD; normal B12; low serum copper and ceruloplasmin; associated with bariatric surgery, excess zinc |
| Tabes dorsalis (neurosyphilis) | Lancinating pains, Argyll Robertson pupils, positive VDRL/TPHA |
| HIV vacuolar myelopathy | HIV-positive patient; similar posterior > lateral column pathology |
| Multiple sclerosis | Focal lesions, relapsing-remitting course, CSF oligoclonal bands |
| Cervical spondylosis | Structural compression, no B12 deficiency |
| Adrenomyeloneuropathy | Very long chain fatty acids elevated |
Management
Treatment Regimen (Parenteral - First-line)
Standard IM cobalamin regimen (Harrison's 22E):
- Days 1-7: 1000 μg intramuscular (IM) cyanocobalamin daily (or hydroxocobalamin)
- Weeks 2-5: 1000 μg IM weekly x 4 weeks
- Maintenance: 1000 μg IM monthly indefinitely (if pernicious anemia or irreversible malabsorption)
Oral cobalamin alternative:
- 1000-2000 μg oral cyanocobalamin daily can be used for maintenance (even in pernicious anemia, as ~1-5% passive absorption occurs independently of intrinsic factor)
- Requires close monitoring to confirm adequacy
Monitoring Response to Treatment
- Serum homocysteine and MMA normalize within ~2 weeks of treatment
- Haematological response within weeks
- Neurological improvement is slower - most improvement occurs over the first 6-12 months
- Recovery may be incomplete, especially if diagnosis was delayed
- The key prognostic factor: time between symptom onset and treatment initiation - earlier treatment = better neurological recovery
Prognosis
- Neurological deficits that are present for >3-6 months are less likely to fully recover
- If no improvement occurs at all, consider alternative diagnoses (copper deficiency, HIV myelopathy)
- B12 supplementation does not improve cognitive function in elderly hyperhomocysteinaemic patients without SCD
Management of Underlying Cause
| Cause | Additional Management |
|---|---|
| Pernicious anemia | Lifelong IM B12 supplementation |
| Dietary deficiency (vegan) | Dietary counselling + oral supplementation |
| Drug-induced (metformin, PPI) | Discontinue if possible, or monitor B12 |
| Post-bariatric surgery | Prophylactic B12 + copper supplementation |
| Nitrous oxide abuse | Stop N2O exposure; B12 replacement; psychiatric/addiction support |
| H. pylori-related | Eradication of H. pylori |
- Harrison's 22E, p. 3612; Bradley & Daroff, pp. 1797-1799; Goldman-Cecil Medicine
Important Clinical Pearls
- Neurological SCD can precede anaemia - do not dismiss B12 deficiency because the CBC is normal.
- The combination of absent reflexes + Babinski sign is a classic bedside clue to SCD (peripheral nerve + corticospinal tract involvement simultaneously).
- Nitrous oxide can precipitate fulminant SCD even after a single dental/surgical anaesthetic in a patient who is already mildly B12 deficient.
- Serum B12 alone is unreliable - always check MMA and homocysteine if clinical suspicion is high.
- Copper deficiency myelopathy is the main mimic and must be excluded in cases where B12 is normal (check serum copper, ceruloplasmin; ask about bariatric surgery, zinc supplements).
- Folate deficiency can produce a similar picture but MMA will be normal (only homocysteine is elevated).
Recent review (2025): Bernetti et al., Brain Sci 2025 - "A Comprehensive Overview of Subacute Combined Degeneration: MRI Diagnostic Challenges and Treatment Pathways" (PMID: 41008332) provides updated MRI criteria and management pathways confirming current practice.
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Bradley & Daroff's Neurology in Clinical Practice | Goldman-Cecil Medicine | Robbins & Kumar Basic Pathology
Subacute degeneration of spinal cord with vit b12 deficiency presentation and management
I covered this topic in detail just a moment ago. Here's the full summary from authoritative textbooks (Harrison's 22E, Bradley & Daroff, Goldman-Cecil):
Subacute Combined Degeneration (SCD) of the Spinal Cord
What Is It?
SCD is a metabolic myelopathy caused by severe vitamin B12 (cobalamin) deficiency. It is the most common form of metabolic myelopathy. The term "combined" refers to simultaneous degeneration of the posterior columns AND lateral columns (corticospinal tracts) of the spinal cord.
Pathophysiology
Two cobalamin-dependent reactions are disrupted:
-
Methionine synthesis: Cobalamin is a cofactor for methionine synthase (homocysteine → methionine). Methionine → S-adenosylmethionine (SAM), essential for myelin methylation reactions. When SAM fails, myelin maintenance breaks down.
-
Methylmalonyl-CoA conversion: Blocked when cobalamin is absent → methylmalonic acid (MMA) accumulates.
The result is spongiform vacuolar demyelination, progressing to axon destruction. Most severely affected: posterior columns at cervical and upper thoracic levels, then lateral columns. Anterior columns are involved only in advanced disease.
Causes of B12 Deficiency
| Mechanism | Examples |
|---|---|
| Pernicious anemia (classic) | Autoimmune gastritis - loss of intrinsic factor; anti-IF and anti-parietal cell antibodies |
| Dietary deficiency | Strict vegans (B12 found only in animal products) |
| Food-cobalamin malabsorption | Atrophic gastritis, H. pylori, hypochlorhydria |
| Post-surgical | Gastrectomy, bariatric surgery, terminal ileum resection |
| Drug-induced | Prolonged PPI, H2 blockers, metformin |
| Ileal disease | Crohn's disease |
| Nitrous oxide (N2O) | Recreational ("whippets") or operative - irreversibly inhibits methionine synthase; even brief anaesthetic exposure can precipitate SCD in already-deficient patients |
| Bacterial overgrowth | Competes for luminal B12 |
Clinical Presentation
Onset
- Insidious, subacute
- Symptoms are symmetric and diffuse (not focal)
Symptom Sequence
1. Sensory (earliest)
- Paresthesias (tingling, numbness) in hands and feet - symmetric, stocking-glove
- Loss of vibration sense and proprioception (posterior column)
- Positive Romberg sign
- Lhermitte's sign (electric shock down spine on neck flexion) may be present
2. Motor
- Progressive leg weakness, spastic gait (lateral column/corticospinal tract)
- Ranges from mild clumsiness to frank spastic paraplegia
3. Classic reflex sign (key diagnostic clue)
- Absent deep tendon reflexes (peripheral neuropathy) + upgoing plantars/Babinski sign (corticospinal tract) coexisting = hallmark of SCD
4. Cognitive/Psychiatric
- Mental slowing, depression, irritability, confusion
- Delusions, hallucinations ("megaloblastic madness") - may be the presenting feature in advanced cases
5. Visual
- Bilateral visual loss, optic atrophy, centrocecal scotomata (optic nerve involvement)
- May precede other symptoms
6. Rare features
- Bladder/autonomic dysfunction
- Brainstem/cerebellar signs
- Reversible coma
Investigations
Haematology
- Macrocytic megaloblastic anaemia, hypersegmented neutrophils
- Important: haematological changes may be absent at neurological presentation - a normal CBC does NOT exclude SCD
Biochemistry
| Test | Finding | Notes |
|---|---|---|
| Serum B12 | Low (<200 pg/mL) | Borderline 200-350 pg/mL; may be falsely normal in myeloproliferative disease |
| Methylmalonic acid (MMA) | Elevated | More specific - elevated in B12 deficiency, NOT folate deficiency |
| Homocysteine | Elevated | Elevated in both B12 and folate deficiency |
| Anti-intrinsic factor Ab | Positive | Low sensitivity (50-70%) but specific for pernicious anemia |
| Anti-parietal cell Ab | Often positive | Nonspecific |
| Serum gastrin | Elevated | Sensitive (~90%) but nonspecific marker of atrophic gastritis |
- MMA + homocysteine are critical when serum B12 is borderline (200-350 pg/mL) or when nitrous oxide abuse is suspected (B12 may be normal)
MRI Spine (Imaging of Choice)
- T2-weighted: hyperintense signal in posterior and lateral columns, cervical/upper thoracic levels - "inverted V" or "trident sign" on axial views
- T1-weighted: hypointensity in dorsal columns; may show mild cord swelling
- Gadolinium enhancement may occur
- MRI can be normal early in disease
Other
- Nerve conduction studies: absent/small sural sensory potentials in ~50% (axonal polyneuropathy)
- Somatosensory/visual evoked potentials: nonspecific abnormalities
- Diffusion tensor imaging: more sensitive for cognitive-correlating white matter changes
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Copper deficiency myelopathy | Clinically identical; normal B12; low serum copper/ceruloplasmin; bariatric surgery, excess zinc history |
| Tabes dorsalis | Lancinating pains, Argyll Robertson pupils, positive syphilis serology |
| HIV vacuolar myelopathy | HIV-positive; similar column pathology |
| Multiple sclerosis | Focal lesions, relapsing course, CSF oligoclonal bands |
| Cervical spondylosis | Structural compression on MRI |
| Folate deficiency | Identical picture but MMA normal; only homocysteine elevated |
Management
B12 Replacement Regimen
Parenteral (first-line, especially with malabsorption):
- Week 1: 1000 μg IM cyanocobalamin (or hydroxocobalamin) daily x 5-7 days
- Weeks 2-5: 1000 μg IM weekly x 4 weeks
- Maintenance: 1000 μg IM monthly indefinitely
Oral (alternative/maintenance):
- 1000-2000 μg oral cyanocobalamin daily - effective even in pernicious anemia due to ~1-5% passive gut absorption (independent of intrinsic factor)
- Requires close monitoring to ensure adequacy
Monitoring Response
| Marker | Timeline |
|---|---|
| Serum MMA + homocysteine | Normalize in ~2 weeks |
| Haematological response | Within weeks |
| Neurological improvement | Mostly over first 6-12 months |
- Recovery may be incomplete, especially if diagnosis was delayed
- Key prognostic factor: shorter time from symptom onset to treatment = better neurological recovery
Treat the Underlying Cause
| Cause | Additional Management |
|---|---|
| Pernicious anemia | Lifelong IM B12 |
| Dietary deficiency (vegan) | Dietary counselling + oral supplementation |
| Metformin/PPI-induced | Discontinue if possible; monitor B12 |
| Post-bariatric surgery | Prophylactic B12 + copper supplementation |
| Nitrous oxide abuse | Stop N2O; psychiatric/addiction support |
| H. pylori | Eradication therapy |
Key Clinical Pearls
- Neurological SCD can precede anaemia - a normal CBC does not rule out B12 deficiency
- Absent reflexes + Babinski sign together = classic SCD bedside clue (simultaneous LMN + UMN signs)
- Nitrous oxide can precipitate fulminant SCD after a single anaesthetic in a mildly deficient patient
- Serum B12 alone is unreliable - always check MMA and homocysteine if clinical suspicion is high
- Copper deficiency myelopathy is the principal mimic when B12 is normal
- Folate deficiency mimics SCD but MMA is normal; homocysteine alone is elevated
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Bradley & Daroff's Neurology in Clinical Practice | Goldman-Cecil Medicine | Recent review: Bernetti et al., Brain Sci 2025 - PMID 41008332
When to give oral vs IM in scd
Finding Sources
Searching PubMed
"vitamin B12 deficiency" AND "oral" AND "intramuscular" treatment
Reading File
Reading File
Reading Article
PMID: 38231320
Here's the complete, evidence-based answer:
Oral vs. IM B12 in SCD - When to Use Which
The Underlying Rationale
The key is understanding how oral B12 works in deficiency states:
- Normal absorption requires intrinsic factor (IF) from gastric parietal cells - this pathway is blocked in pernicious anemia and malabsorption
- But a second, IF-independent passive absorption pathway exists throughout the entire gut, absorbing ~1-5% of any oral dose
- At a dose of 1000-2000 μg orally, that 1-5% = 10-20 μg absorbed - enough to replete stores over time
This is why high-dose oral therapy works even in pernicious anemia - it bypasses the intrinsic factor problem entirely through mass action.
Decision Framework: IM vs. Oral
Give IM When:
| Situation | Reason |
|---|---|
| Active neurological disease (SCD) - induction phase | Need rapid, reliable, high serum levels; don't risk subtherapeutic absorption during critical early treatment window |
| Severe deficiency (very low B12, florid megaloblastic anemia) | Fastest repletion; no reliance on gut integrity |
| Pernicious anemia - initial treatment | IF completely absent; while oral eventually works, IM guarantees adequate levels during induction |
| Gastrectomy / bariatric surgery | Gastric IF secretion abolished |
| Terminal ileum resection or severe Crohn's | Main absorption site surgically absent |
| Patient non-compliance or unreliable oral intake | IM guarantees delivery |
| Oral supplementation tried but levels not responding | Switch to monthly IM if serum B12 fails to rise with oral therapy |
| Severe vomiting or dysphagia | Cannot reliably absorb oral |
| Nitrous oxide-precipitated acute SCD | Rapid repletion needed |
Give Oral (High-Dose) When:
| Situation | Reason |
|---|---|
| Dietary deficiency (vegans, elderly with poor intake) | No absorption defect; oral is simple and effective |
| Food-cobalamin malabsorption (atrophic gastritis, H. pylori, PPI/metformin use) | Passive absorption still intact; oral 1000 μg/day works well |
| Maintenance therapy after initial IM induction in pernicious anemia | Once stores replete and neurological status stable, oral 1000-2000 μg/day is an acceptable, evidence-based alternative to monthly IM |
| Patient preference (needle phobia, poor venous access) | RCTs support equivalence for maintenance |
| Mild-moderate deficiency without neurological disease | Convenient, non-inferior |
Regimen Summary
| Phase | Route | Dose |
|---|---|---|
| Induction (neurological disease present) | IM | 1000 μg daily x 5-7 days |
| Consolidation | IM | 1000 μg weekly x 4 weeks |
| Maintenance - if malabsorption/PA | IM or Oral | IM: 1000 μg monthly; Oral: 1000-2000 μg daily |
| Dietary deficiency - all phases | Oral | 1000-2000 μg daily |
(Goldman-Cecil: start 1000-2000 μg SC/IM daily x 1 week, then weekly x 1 month, then oral 1000 μg daily indefinitely)
What the Evidence Says
Systematic Review & Network Meta-Analysis (Abdelwahab et al., Ir J Med Sci 2024 - PMID 38231320) - 13 studies, 4275 patients:
- IM ranked highest for raising serum B12 levels (MD +94 pg/mL vs oral), but the difference was not statistically significant
- No significant difference between IM, oral, and sublingual for haemoglobin correction or homocysteine normalisation
- Conclusion: all three routes effectively increase B12 levels; IM is top-ranked but not clinically superior for biochemical endpoints
Pragmatic RCT (Sanz-Cuesta et al., BMJ Open 2020 - PMID 32819927): Oral was non-inferior to IM in primary care B12 deficiency.
Key caveat: Most RCT data focus on biochemical endpoints (serum B12, haemoglobin) in mixed populations. There are no large RCTs specifically in SCD comparing oral vs IM for neurological recovery - which is why most neurology guidelines still recommend IM for induction when neurological disease is present, prioritising reliability over convenience.
Bottom Line
| Induction in SCD | Maintenance in SCD | Dietary deficiency | |
|---|---|---|---|
| IM | ✅ First choice | ✅ Acceptable | Not needed |
| Oral 1000-2000 μg/day | ⚠️ Only if IM not feasible | ✅ Evidence-based alternative | ✅ First choice |
The main clinical rule: never gamble on gut absorption when the spinal cord is at stake during the acute/induction phase. Once neurological stability is achieved and stores are replete, a switch to closely monitored high-dose oral therapy is reasonable.
- Sources: Goldman-Cecil Medicine | Bradley & Daroff's Neurology | Symptom to Diagnosis (4th Ed) | Abdelwahab et al. 2024 (PMID 38231320)
This is a shared conversation. Sign in to Orris to start your own chat.