Coronary artery disease
Reading File
Finding Sources
Finding Sources
Searching PubMed
"coronary artery disease"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compose the full response.
Coronary Artery Disease (CAD)
Definition and Epidemiology
Coronary artery disease (CAD), also called ischemic heart disease (IHD), is the most common form of cardiovascular disease and the leading cause of mortality worldwide. It may present as stable angina pectoris, acute coronary syndromes (ACS), or ischemic heart failure. According to the WHO, IHD accounts for 16.2% of all cardiovascular deaths globally - more than any other cardiovascular condition.
In the United States, CAD causes approximately 365,000+ deaths annually, including ~600,000 first acute MIs, ~200,000 recurrent MIs, and an estimated 170,000 "silent" MIs each year. By 2035, an estimated 45.1% of the US population will have some form of cardiovascular disease, with projected costs exceeding $1.1 trillion. - Sabiston Textbook of Surgery, p. 2482
Coronary Artery Anatomy
The heart is supplied by two main coronary arteries arising from their respective sinuses of Valsalva as the first branches of the aorta:
- Left Coronary Artery (LCA/LMCA): Branches into the left anterior descending (LAD) - supplying the LV free wall and interventricular septum - and the left circumflex artery - running along the AV groove.
- Right Coronary Artery (RCA): Supplies the RV free wall and, via the posterior descending artery (PDA), the inferior wall of the LV. In right-dominant systems (most common), the RCA gives rise to the PDA.
The LAD is often referred to as the "widow maker" because proximal occlusion produces the largest area of infarction. - Sabiston Textbook of Surgery, p. 2485
Risk Factors
Major modifiable risk factors include:
- Hypertension
- Dyslipidemia (elevated LDL, low HDL)
- Diabetes mellitus
- Tobacco use / smoking
- Truncal obesity
- Sedentary lifestyle
- Unhealthy diet
Non-modifiable risk factors:
- Age >40 years
- Male sex (or postmenopausal female)
- Family history of premature CAD
- Genetic predisposition (estimated ~40% heritability)
When all modifiable risk factors are optimal, the lifetime risk of CAD for a 45-year-old is estimated to be <5%. With two or more major risk factors, risk rises to 50% for men and 31% for women. All modifiable risk factors combined account for >90% of the population-attributable risk of acute MI globally. - Goldman-Cecil Medicine, p. 650
Pathophysiology
Atherosclerosis - The Core Process
CAD results from atherosclerosis - a chronic inflammatory process in the arterial wall. The sequence:
- Endothelial injury triggered by hyperlipidemia, hypertension, smoking, or hyperglycemia.
- Lipid accumulation - LDL particles penetrate the endothelium and become oxidized, attracting monocytes that differentiate into macrophages and engulf oxidized LDL, forming foam cells.
- Plaque development - Smooth muscle cells migrate from the media and proliferate. The plaque acquires extracellular matrix components (collagen, proteoglycans), forming a fibrous cap over a lipid-rich necrotic core.
- Plaque instability - Matrix metalloproteinases (MMPs), produced by macrophages and smooth muscle cells, degrade the fibrous cap. Pro-inflammatory cytokines (IL-1β, TNF-α) amplify this process, increasing plaque vulnerability to rupture.
Three Mechanisms Precipitating Acute Coronary Syndromes
- Plaque rupture (most common) - The fibrous cap breaks, exposing the thrombogenic core to circulating blood, triggering thrombus formation and potential vessel occlusion.
- Plaque erosion - The outer endothelial layer is worn away without full rupture; up to one-third of acute MIs result from this mechanism.
- Calcified nodule - Hard calcified deposits fracture through the fibrous cap, potentially causing sudden luminal obstruction.
STEMI (transmural infarction) typically results from complete plaque rupture and total occlusion. NSTEMI arises from partial occlusion or severe flow reduction, often via erosion. - Sabiston Textbook of Surgery, p. 2485
Clinical Spectrum
Stable Angina (Chronic CAD)
- Chest pressure, tightness, or heaviness precipitated by exertion or emotional stress, relieved by rest or nitrates within minutes
- Caused by a fixed obstructive lesion reducing flow during demand states
- Canadian Cardiovascular Society (CCS) Classification grades severity (I-IV)
Acute Coronary Syndromes (ACS)
Unstable atheromatous plaque leads to acute thrombosis:
- Unstable Angina (UA): Rest angina >20 min, new-onset severe angina (CCS ≥3), or crescendo angina - cardiac biomarkers normal
- NSTEMI: Similar presentation; cardiac biomarkers elevated, ST depression or T-wave changes on ECG
- STEMI: Complete occlusion; ST elevation on ECG, positive biomarkers, transmural infarction
MI Classification (Fourth Universal Definition)
| Type | Mechanism |
|---|---|
| Type 1 | Spontaneous - plaque rupture/erosion/fissuring |
| Type 2 | Supply-demand mismatch (e.g., tachyarrhythmia, anemia, hypotension) |
| Type 3 | Sudden cardiac death before biomarker results |
| Type 4 | PCI-related |
| Type 5 | CABG-related |
- Sabiston Textbook of Surgery, p. 2487
Diagnostic Workup
Clinical Assessment
- Detailed history: character, radiation (jaw, left arm), duration, precipitants of chest pain
- Physical examination: S3/S4 gallop, signs of heart failure, bruits
ECG
- Resting ECG: May show ST changes, Q waves (prior MI), LBBB
- ST elevation in contiguous leads: STEMI
- ST depression, T-wave inversions: NSTEMI/UA or ischemia
Cardiac Biomarkers
- High-sensitivity troponin I/T: Preferred biomarker; rises within 1-3 hours, peaks at 12-24 hours, stays elevated for days
- Serial measurements at 0 and 1-3 hours used in accelerated diagnostic protocols
Non-Invasive Imaging
| Test | Use |
|---|---|
| Echocardiography | Wall motion abnormalities, EF assessment, valvular function |
| Exercise treadmill test | Low-risk stable patients; sensitivity ~71%, specificity ~90% |
| Stress echocardiography | If baseline ECG abnormal or unable to exercise |
| Nuclear stress test (MPI) | Myocardial perfusion; involves radiotracer |
| Coronary CT angiography (CCTA) | Excellent negative predictive value; rules out CAD |
| Cardiac MRI | Gold standard for LV volumetry and viability assessment; MRA sensitivity 89%, specificity 72% (95% with contrast) |
Invasive Evaluation
-
Coronary angiography (cardiac catheterization): Defines anatomy, degree of stenosis, and suitability for revascularization - the definitive standard
-
FFR/iFR: Physiologic assessment of lesion significance (>50% stenosis that is functionally significant)
-
OCT/IVUS: Intracoronary imaging for plaque characterization and stent optimization
-
SYNTAX score: Quantifies coronary complexity; guides PCI vs. CABG decision
-
STS risk score: Predicts surgical risk
-
Sabiston Textbook of Surgery, p. 2487-2490
Management
Medical Therapy (Guideline-Directed Medical Therapy - GDMT)
Antiplatelet therapy:
- Aspirin 75-100 mg daily: cornerstone of secondary prevention
- P2Y12 inhibitors (clopidogrel, ticagrelor, prasugrel): used for dual antiplatelet therapy (DAPT) post-ACS/PCI
- A 2025 Lancet meta-analysis found clopidogrel may be superior to aspirin for secondary prevention in certain CAD patients
- A 2025 BMJ individual patient data meta-analysis supports P2Y12 inhibitor monotherapy after PCI over aspirin monotherapy
Lipid-lowering therapy:
- High-intensity statins (atorvastatin 40-80 mg, rosuvastatin 20-40 mg): first-line
- Add ezetimibe if LDL-C target not reached; a 2024 meta-analysis in BMC Cardiovascular Disorders showed low/moderate statin + ezetimibe is non-inferior to high-intensity statin monotherapy with better tolerability
- PCSK9 inhibitors for high-risk patients not at LDL-C target
Anti-anginal / hemodynamic:
- Beta-blockers: Reduce heart rate and oxygen demand; improve survival post-MI; first-line for stable angina
- Nitrates: Venodilation reduces preload; sublingual GTN for acute relief
- Calcium channel blockers: Used if beta-blockers contraindicated or for vasospastic angina
- Ranolazine: Late sodium current inhibitor; add-on therapy for refractory angina
- Ivabradine: Heart rate reduction in specific patients
Other cardioprotective agents:
- ACE inhibitors/ARBs: Especially post-MI with reduced EF, diabetes, or hypertension
- Mineralocorticoid receptor antagonists: Post-MI with EF <40%
- Anticoagulation: For AF with CAD - warfarin or DOAC; management of antithrombotic therapy in this scenario has been addressed by a 2025 JACC meta-analysis
Risk factor modification:
- Smoking cessation, blood pressure control (target <130/80 mmHg), diabetes management (HbA1c control), Mediterranean diet, regular aerobic exercise, weight management
Revascularization
Percutaneous Coronary Intervention (PCI)
- Balloon angioplasty + stenting (DES preferred over BMS)
- STEMI: Primary PCI is the preferred reperfusion strategy; target door-to-balloon time ≤90 minutes
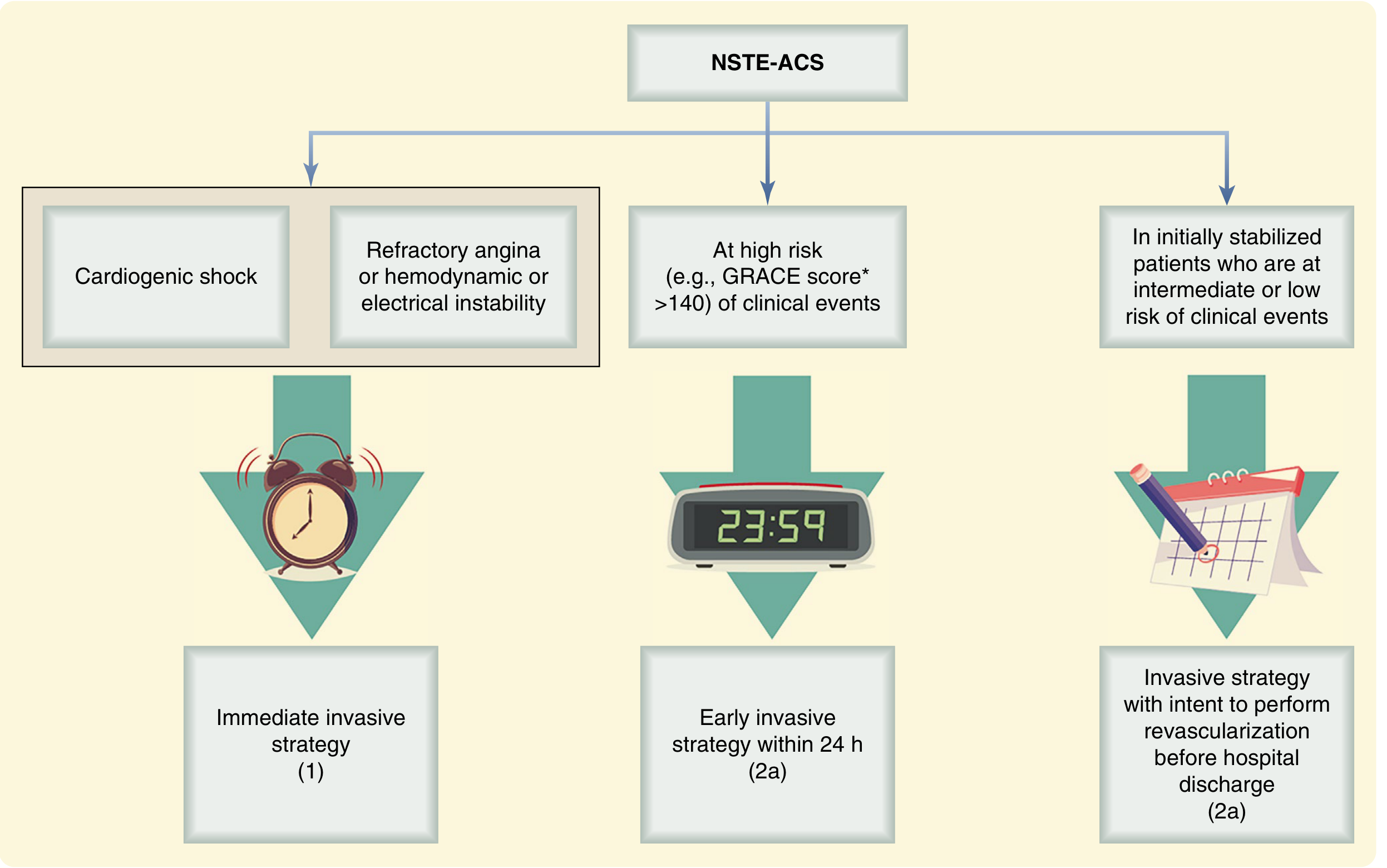
- NSTE-ACS:
- Immediate invasive (<2 hours): cardiogenic shock, refractory angina, hemodynamic/electrical instability
- Early invasive (<24 hours): GRACE score >140
- Invasive before discharge: Low-intermediate risk patients
Coronary Artery Bypass Grafting (CABG)
CABG is preferred over PCI in:
- Left main CAD (≥50% stenosis)
- Three-vessel CAD with reduced EF or diabetes
- Complex multivessel disease (high SYNTAX score)
- Patients undergoing concurrent cardiac surgery (valve repair, etc.)
Conduit selection:
- Left internal mammary artery (LIMA) to LAD: gold standard - superior long-term patency
- Bilateral internal mammary artery (BIMA): improves survival, especially in younger patients
- Radial artery, right IMA, saphenous vein graft (SVG) as additional conduits
CABG techniques:
- Conventional on-pump CABG (cardiopulmonary bypass with cardioplegic arrest)
- Off-pump CABG (beating heart)
- Minimally invasive direct CABG (MIDCAB)
- Robotic totally endoscopic CABG
- Hybrid coronary surgery (CABG + PCI)
Anticoagulation for CPB: Heparin 300-400 U/kg; target ACT >400 seconds. - Sabiston Textbook of Surgery, p. 2495-2499
Mechanical Complications of Acute MI
| Complication | Timing | Features |
|---|---|---|
| LV free wall rupture | 3-5 days | Cardiac tamponade, sudden death |
| LV pseudoaneurysm | Days-weeks | Contained rupture; pericardium holds it |
| Ventricular septal defect | 3-5 days | New harsh holosystolic murmur, step-up in O2 saturation at RV level |
| Papillary muscle rupture | 2-7 days | Acute severe mitral regurgitation, pulmonary edema |
Special Populations
- Females: Often present atypically (dyspnea, fatigue, nausea); higher incidence of MINOCA (MI with non-obstructive coronary arteries); INOCA (ischemia with non-obstructive CAD) is more common
- Diabetic patients: Higher restenosis risk post-PCI; often benefit more from CABG
- Renal disease: Contrast-induced nephropathy risk; dose-adjust antiplatelet/anticoagulant agents
- Elderly (>70 years): Higher surgical risk; careful risk-benefit assessment required
- Pregnant patients: Rare; gestational MI managed on individual basis
Secondary Prevention and Cardiac Rehabilitation
Post-revascularization GDMT includes:
- Aspirin indefinitely; DAPT for 6-12 months post-DES implantation
- High-intensity statin therapy with LDL-C goal <55 mg/dL (very high risk)
- Beta-blocker (if EF reduced or post-MI)
- ACE inhibitor/ARB
- Cardiac rehabilitation (exercise training, education, psychological support)
- Lifestyle modification - smoking cessation, diet, weight, blood pressure, diabetes control
Key Recent Evidence (2024-2026)
| Study | Key Finding |
|---|---|
| Clopidogrel vs. aspirin - Lancet 2025 | Clopidogrel superior to aspirin for secondary prevention in CAD |
| P2Y12 vs. aspirin post-PCI - BMJ 2025 | P2Y12 monotherapy after PCI outperforms aspirin monotherapy |
| Statin + ezetimibe vs. high-intensity statin - BMC 2024 | Combination therapy comparable efficacy, better tolerance |
| AF + stable CAD anticoagulation - JACC 2025 | Anticoagulation alone (without antiplatelet) appropriate in stable AF+CAD |
| Coronary artery calcium density - JACC Imaging 2025 | CAC density independently predicts cardiovascular events |
Sources: Sabiston Textbook of Surgery 21e | Goldman-Cecil Medicine | Tintinalli's Emergency Medicine | Fuster and Hurst's The Heart 15e | Harrison's Principles of Internal Medicine 22e | Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.