Discuss the primary management of Facial Trauma patient. give a deepdive answer about above topic with contents and references
Reading File
Finding Sources
Finding Sources
Searching PubMed
"facial trauma" AND "management"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the deep-dive answer.
Primary Management of Facial Trauma: A Deep Dive
Table of Contents
- Background and Importance
- Anatomy and Pathophysiology
- Primary Survey (ABCDE)
- A - Airway Management
- B - Breathing
- C - Circulation / Hemorrhage Control
- D - Disability (Neurologic)
- E - Exposure
- Secondary Survey and Clinical Examination
- Imaging
- Specific Fracture Management
- Frontal Bone Fractures
- Orbital Fractures (Blow-out)
- Zygomaticomaxillary Complex Fractures
- Nasal Fractures
- Naso-orbito-ethmoid (NOE) Fractures
- Le Fort Fractures (I, II, III)
- Mandibular Fractures
- Soft Tissue Injuries
- Associated Injuries
- Definitive / Operative Repair Principles
- Special Populations and Psychosocial Considerations
- Summary Algorithm
- References
1. Background and Importance
The face is a complex structure essential to breathing, eating, speaking, and non-verbal communication. Its appearance carries deep implications for self-esteem, social interaction, and psychological well-being. Facial trauma patients experience long-term sequelae including unemployment, drug and alcohol abuse, marital difficulties, and negative body image. Multiple studies confirm high rates of anxiety, depression, and post-traumatic stress disorder after facial injuries.
Four main specialties share responsibility for definitive care: ophthalmology, plastic and reconstructive surgery, otolaryngology, and oral and maxillofacial surgery. Early specialist consultation is strongly encouraged. However, the emergency physician's first goal is always addressing life-threatening problems.
Epidemiologically, the proportion of facial injuries from interpersonal violence is increasing, while motor vehicle collision (MVC) injuries are decreasing due to seatbelt and airbag use. A careful history is mandatory, and abuse should always be considered -- particularly in women, children, and the elderly.
- Rosen's Emergency Medicine: Concepts and Clinical Practice, 10e, p. 404
2. Anatomy and Pathophysiology
The facial skeleton consists of vertical and horizontal buttresses joined at suture lines:
- Stronger vertical buttresses: zygomaticomaxillary buttress (laterally) and frontal process of the maxilla (medially)
- Weaker horizontal buttresses: superior orbital rims, orbital floor, hard palate
- The orbit is composed of seven bones; the inferior and medial walls are particularly fragile
The orbit's fragility explains why frontal, lateral, and oblique forces predictably produce fractures at these sites. The posterior portions of the facial bones form the anterior wall of the calvaria, placing facial injuries in proximity to the CNS.
Buried structures susceptible to injury include:
- Lacrimal glands and nasolacrimal duct (drain tears from the conjunctiva into the nasopharynx)
- Parotid gland and Stensen's duct (runs from the gland ~5 cm to enter the mouth opposite the upper second molar)
- Submandibular (Wharton's) ducts and sublingual glands
- Tintinalli's Emergency Medicine: A Comprehensive Study, Table 259-1, p. 1756
3. Primary Survey (ABCDE)
A - Airway Management
This is the most critical step. Up to 44% of patients with severe maxillofacial trauma require endotracheal intubation due to mechanical disruption or massive hemorrhage into the airway.
Key principles:
- Reposition with jaw thrust (before cervical spine clearance) or head tilt/chin lift after clearance
- Grasp an obstructing tongue with gauze or towel clip and pull anteriorly in bilateral mandible fractures
- Remove avulsed teeth and foreign bodies immediately
- Avoid nasal trumpets in severe midfacial injuries - risk of worsening injury or intracranial placement
- Bag-mask ventilation often requires a two-person technique due to loss of normal facial bony architecture
- Allow alert patients without critical associated injury to remain upright with suction in hand
Rapid-sequence intubation (RSI) is the preferred method in trauma. However, always plan for the difficult airway:
- Do not administer paralytics unless effective bag-mask ventilation is confirmed or alternative airway plans are in place
- Awake intubation with sedation + local airway anesthesia can preserve airway reflexes during assessment
- Etomidate and ketamine both provide sedation with preservation of respiratory drive
- Fiberoptic intubation is an option when time allows and hemorrhage is minimal
- Always prepare the neck and have a cricothyrotomy kit ready
- Laryngeal mask airway (LMA) may temporize but does not protect against aspiration
- Avoid nasal intubation to prevent worsening of midface injuries and risk of intracranial placement
Surgical airway (cricothyrotomy) may be necessary, particularly in penetrating gunshot wounds to the face.
- Tintinalli's Emergency Medicine, p. 1757-1758
B - Breathing
Facial trauma in isolation rarely compromises ventilation directly, but co-existing injuries (cervical spine, chest) must be assessed. Pneumothorax and hemothorax are present in up to 20% of patients with penetrating neck/facial trauma. Auscultate for breath sounds; treat tension pneumothorax with immediate needle decompression at the 4th-5th intercostal space in the anterior axillary line.
C - Circulation / Hemorrhage Control
Shock from facial trauma alone is rare -- it occurs only from obvious external bleeding. If the patient is in shock, actively search for other causes (chest, abdomen, pelvis, long bones).
Blood supply to the face comes primarily from the sphenopalatine and greater palatine branches of the external carotid artery, with extensive anastomoses from the internal carotid (anterior/posterior ethmoidal arteries).
Management steps:
- Apply direct pressure to external wounds; avoid blind clamping (risk of nerve injury, cerebral ischemia)
- Control posterior nasal epistaxis early with nasal tampon, dual balloon device, or Foley catheter with anterior layered gauze packing
- Be careful with nasal packing in severe midfacial fractures to avoid intracranial placement
- Manual reduction of significantly displaced nasal fractures and Le Fort injuries may occasionally be needed to stop arterial bleeding
- For persistent life-threatening hemorrhage: immediate operative vessel ligation or fracture reduction
- Arterial embolization (branches of external carotid artery) is effective but carries small stroke risk
- Life-threatening hemorrhage can occur in up to 10% of midface fracture patients
- Tintinalli's Emergency Medicine, p. 1757
D - Disability (Neurologic)
The incidence of associated brain injury is directly related to the mechanism and severity of facial fractures. Evaluate GCS, pupils, and lateralizing signs. Traumatic brain injury is a common co-existing injury and may impair the patient's ability to protect their airway.
E - Exposure
A thorough head-to-toe examination follows stabilization. Facial injuries should not distract from searching for other life-threatening injuries.
4. Secondary Survey and Clinical Examination
The secondary survey begins only after life-threatening injuries have been managed. Use three screening questions:
- "How is your vision?" - any visual complaint mandates thorough ocular exam
- "Is your face numb?" - check for forehead (supraorbital nerve), lower eyelid/cheek (infraorbital nerve), or chin (mental nerve) anesthesia suggesting specific fractures
- "Do your teeth fit together normally?" - malocclusion indicates mandibular or maxillary fractures; condyle injury produces TMJ-area pain
Inspection:
- Lateral view: dish face with Le Fort III fractures
- Frontal view: donkey (elongated) face with Le Fort II or III fractures
- Bird's eye view: exophthalmos suggesting retrobulbar hematoma
- Worm's view: enophthalmos (blow-out fracture) or malar flattening (zygomatic arch fracture)
- Raccoon eyes (bilateral periorbital ecchymosis) and Battle's sign (mastoid ecchymosis) -- develop over hours, suggest basilar skull fracture
Palpation:
- Systematic palpation of the entire facial skeleton detects the majority of fractures
- Intraoral palpation of the zygomatic arch (lateral to posterior maxillary molars)
- Assess for Le Fort fractures by gently rocking the hard palate while stabilizing the forehead
Eye Examination:
- Examine before significant swelling occurs (use lid retractors if needed)
- Document corrected visual acuity
- Examine: pupil (teardrop sign = globe rupture), hyphema, afferent pupillary defect (APD), extraocular motility, lens dislocation
- Binocular diplopia = muscle entrapment; monocular diplopia = lens dislocation
- Limitation on upward gaze = inferior/medial orbital wall fracture with inferior rectus entrapment
- Tintinalli's Emergency Medicine, Table 259-2, p. 1758-1759
5. Imaging
CT scanning is the gold standard for facial trauma evaluation.
| Indication | Imaging |
|---|---|
| Obvious facial injury | Directed facial CT (axial + coronal sections) |
| Orbital involvement | Facial/orbital CT with axial and coronal cuts |
| Suspected frontal sinus fracture | Head CT for anterior/posterior tables + intracranial structures |
| Le Fort / panfacial fractures | Thin-section axial + coronal NCCT |
Strategy for evaluating sinus trauma on CT: visually trace each bony outline on consecutive slices in both planes. Indirect signs of fracture include:
- Air-fluid level in a sinus
- Complete sinus opacification with blood
- Gas outside the sinus (pneumocephalus, subcutaneous emphysema, infratemporal fossa gas)
Displaced orbital floor fractures may entrap fat or extraocular muscles, causing enophthalmos or ocular motility dysfunction.
Waters' view X-ray (plain film) can show a "teardrop sign" and sinus opacification in orbital blow-out fractures, but CT provides superior detail for surgical planning.
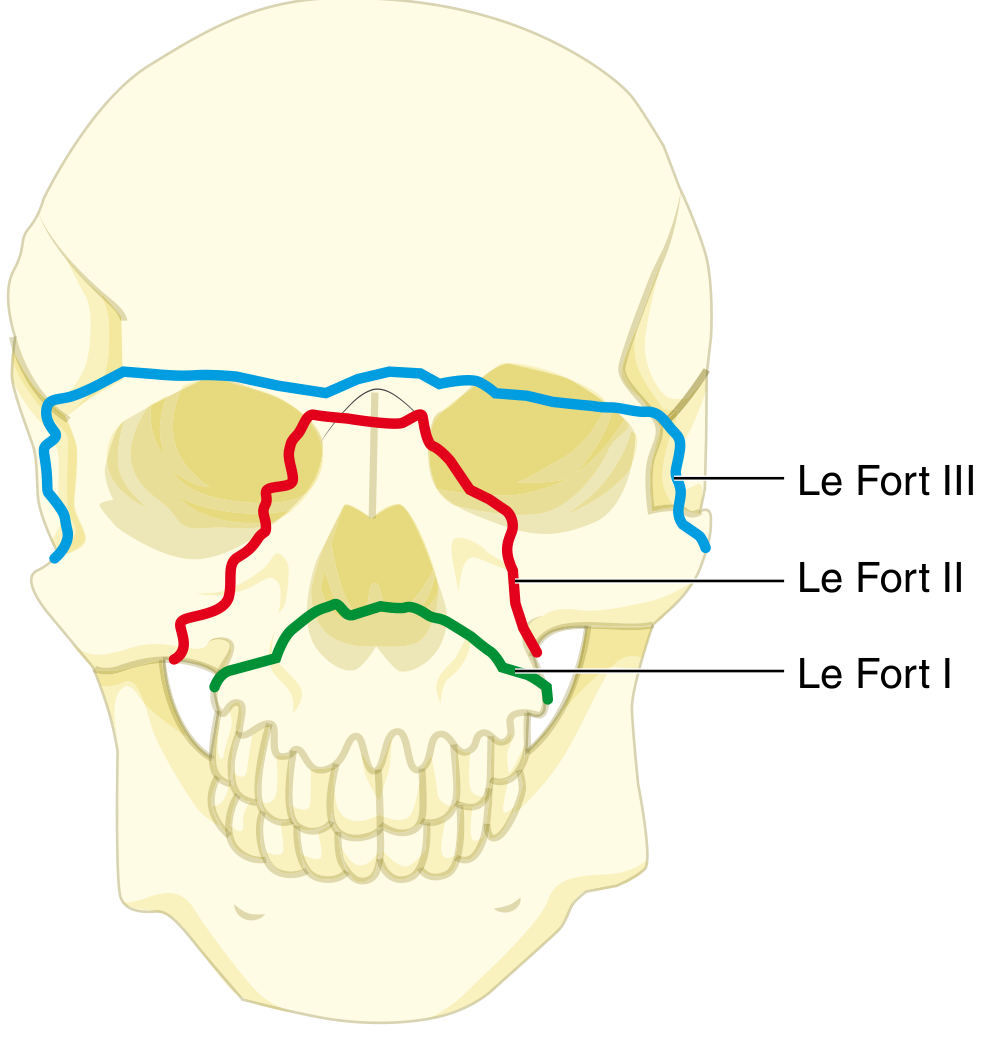
Le Fort I (green) = transverse maxillary fracture. Le Fort II (red) = pyramidal fracture through nasal bones and orbital floors. Le Fort III (blue) = craniofacial disjunction. - Sabiston Textbook of Surgery
- Cummings Otolaryngology Head and Neck Surgery, p. 190
6. Specific Fracture Management
6a. Frontal Bone Fractures
High-energy mechanism (unrestrained MVC, assault with blunt object). The thick frontal bone requires significant force to fracture, making concomitant TBI, additional facial fractures, and C-spine injury likely. Craniofacial injuries present in 56-87% of patients.
- Lacerations typically overlie these fractures -- careful exploration needed
- Crepitus is frequently palpable with any sinus fracture
- Otorrhea = CSF leak until proven otherwise; rhinorrhea similarly
Management by fracture type:
- Isolated anterior table fracture: discharge with nasal/oral decongestants, oral antibiotics (first-generation cephalosporins or amoxicillin-clavulanate), follow-up with facial surgeon
- Depressed fractures: admit for IV antibiotics + operative repair
- Through-and-through (posterior table) fractures: operative repair required to prevent pneumocephalus, CSF leak, mucopyocele, and cranial empyema
- Tintinalli's Emergency Medicine, p. 1760
6b. Orbital Fractures (Blow-out)
Two categories:
- Pure blow-out fracture: only orbital walls involved; force transmitted through the fluid-filled globe fractures the weaker inferior or medial orbital walls - adipose tissue, inferior rectus, or inferior oblique can herniate into the maxillary or ethmoid sinuses
- Impure orbital fractures: involve orbital walls with rim fracture, typically accompanying other facial fractures
Clinical signs:
- Enophthalmos (herniation before significant edema)
- Step-off deformity or crepitus on rim palpation
- Infraorbital anesthesia (orbital floor fracture)
- Diplopia on upward gaze (inferior rectus/oblique entrapment)
- Traumatic telecanthus, epiphora, CSF leak (NOE fractures)
Management:
- Oral amoxicillin-clavulanate, decongestants, instruct patient to avoid nose blowing
- Specialty consultation before discharge (controversy about optimal timing for operative repair)
- Adults: repair may be delayed 1-2 weeks; children need shorter follow-up and earlier repair
Emergencies:
- Retrobulbar hematoma / malignant orbital emphysema creating ocular compartment syndrome: emergency lateral canthotomy (reduces ocular pressure and prevents ischemic optic neuropathy)
- Orbital fissure syndrome: fracture involving superior orbital fissure with injury to CN III and CN V1 - paralysis of extraocular movements, ptosis, periorbital anesthesia
- Orbital apex syndrome: as above plus optic nerve involvement (diminished visual acuity)
- Tintinalli's Emergency Medicine, p. 1760-1761
6c. Zygomaticomaxillary Complex (ZMC / "Tripod") Fractures
The prominent zygoma is frequently fractured. Two patterns:
- Zygomatic arch fracture: anterior-lateral force (fist or blunt object)
- ZMC / tripod fracture: high-energy deceleration with disruption of zygomaticofrontal suture, zygomaticotemporal junction, and infraorbital rim
Clinical findings:
- Flattening of the malar eminence (before swelling obscures it)
- Lateral canthus pulled inferiorly
- Large lateral subconjunctival hemorrhage
- Trismus (masseter spasm or coronoid process impingement)
- Diplopia, infraorbital anesthesia, possible enophthalmos
Because the zygoma forms the inferior and lateral orbital walls and the superior/lateral maxillary sinus roof, ZMC fractures are simultaneously orbital and sinus fractures.
Management: CT to confirm; specialist (oral-maxillofacial/plastic surgery) consultation; surgical repair for displaced fractures, typically within 1-2 weeks to allow swelling to reduce.
- Tintinalli's Emergency Medicine, p. 1761
6d. Nasal Fractures
The most common facial fractures. Management:
- Ice, analgesia
- Assess for septal hematoma (fluctuant bluish swelling of the septum) - requires immediate drainage to prevent cartilage avascular necrosis and saddle-nose deformity
- Closed reduction: ideally performed within 24-72 hours before significant swelling or after swelling resolves (5-10 days)
- Refer to otolaryngology or plastic surgery
6e. Naso-Orbito-Ethmoid (NOE) Fractures
High-energy central facial fractures involving the nasal bones, ethmoid sinuses, and medial orbital walls. Often accompanied by:
- Lacrimal duct injury
- Dural tears
- Traumatic brain injury
- Traumatic telecanthus
Management: Admission for specialist consultation with facial surgery AND neurosurgery.
6f. Le Fort Fractures
Le Fort fractures represent midface fractures following predictable patterns described by René Le Fort in 1901. All pass through the pterygoid plates.
| Level | Fracture Pattern | Clinical Finding |
|---|---|---|
| Le Fort I | Transverse - separates tooth-bearing maxilla from midface | Mobile hard palate, malocclusion |
| Le Fort II | Pyramidal - through nasal bones, medial orbits, orbital floor | "Donkey face," mobile midface |
| Le Fort III | Craniofacial disjunction - entire midface separates from skull | "Dish face," massive mobility |
Management:
- Secure airway FIRST (these fractures can cause complete upper airway obstruction)
- Control hemorrhage (major risk with Le Fort II/III)
- Manual anterior traction on the mobile maxilla can temporarily reopen the airway
- All require operative repair (open reduction and internal fixation) by maxillofacial/plastic surgery
- Definitive repair may be delayed if needed to address other serious injuries
- Tintinalli's Emergency Medicine, p. 1757; Rosen's Emergency Medicine p. 3437-3468; Cummings Otolaryngology p. 2879-2897
6g. Mandibular Fractures
Common with direct blows; frequently multiple (bilateral mandible fractures may cause posterior displacement of the tongue with complete airway obstruction - a surgical emergency).
Classification by location: symphysis, parasymphysis, body, angle, ramus, condyle, coronoid process
Clinical features:
- Malocclusion (very reliable sign)
- Pain at TMJ region = condyle injury
- Step-off on gingival surface
- Mental nerve anesthesia (fractures near the mental foramen)
Management:
- Mandibular fractures can paradoxically make intubation easier than expected (loss of normal bony resistance)
- Grasp an obstructing tongue anteriorly with suture or gauze
- Definitive: open reduction and internal fixation (ORIF) or intermaxillary fixation (IMF)
7. Soft Tissue Injuries
Abrasions: Clean debris meticulously (topical lidocaine before vigorous scrubbing); delay in removing embedded material leads to epithelialization and permanent tattoo. Cover with thin antibiotic ointment.
Lacerations:
- Explore for depth, foreign bodies, and underlying fractures after adequate anesthesia
- Use nerve blocks (field or facial) to minimize wound edge distortion
- Simple clean wounds closed within 6 hours may not need irrigation
- For wounds <3 cm without gaping: single-layer closure sufficient
- Deeper gaping wounds: buried absorbable subcuticular sutures to close dead space and relieve tension
- Tissue adhesive: faster, less painful, equally effective cosmetically -- but contraindicated for stellate lacerations, animal bites, mucosal/mucocutaneous surfaces, or high-tension areas
Antibiotics: Not required for simple facial wounds. Indicated for:
- Bite wounds
- Devascularized wounds
- Through-and-through buccal mucosa wounds
- Wounds involving ear/nose cartilage
- Extensively contaminated wounds
- Immunocompromised patients
Select antibiotics based on normal flora of the affected site.
- Rosen's Emergency Medicine, p. 3666-3677
8. Associated Injuries
Always evaluate for co-existing injuries based on mechanism:
| Associated Structure | Injury |
|---|---|
| Brain | TBI (direct relationship to mechanism/fracture severity) |
| Cervical spine | C-spine fracture/dislocation (maintain immobilization until cleared) |
| Eyes | Vision loss in up to 6% of maxillofacial trauma patients |
| Lungs | Pneumothorax, hemothorax (especially penetrating) |
| Skull base | CSF leak, cranial nerve injury |
9. Definitive / Operative Repair Principles
The key principle: "Definitive facial treatment may be delayed, if necessary, to address other serious injuries."
Recent evidence (2026 systematic review, PMID 41729299) on early vs. delayed fixation in polytrauma suggests the timing debate continues, with no consensus on superiority of early (within 24 hours) vs. delayed fixation for maxillofacial fractures in polytrauma patients.
Damage control principles applicable to facial trauma:
- Temporizing measures (packing, manual reduction) first to restore physiology
- Definitive ORIF delayed until the patient is hemodynamically stable
- Prioritize correction of hypothermia, coagulopathy, and metabolic acidosis (the "lethal triad")
Surgical options include:
- ORIF with titanium plates/screws (most midface and mandibular fractures)
- Intermaxillary fixation (IMF) for mandibular fractures
- Endoscopic repair for orbital floor blow-outs
- Lateral canthotomy + cantholysis for emergent orbital decompression
- Arterial embolization for uncontrolled midface hemorrhage
- Sabiston Textbook of Surgery, p. 304-316
10. Special Populations and Psychosocial Considerations
Children: Facial bones are not fully mineralized and fracture patterns differ; injury may affect subsequent craniofacial growth; shorter follow-up windows and earlier repair needed for orbital injuries.
Elderly: Even low-energy mechanisms (fall from standing) can cause significant injury.
Abuse screening: Mandatory for women, children, and elderly when mechanism does not match injury pattern. Report all suspected abuse to appropriate authorities.
Psychological rehabilitation: Multiple studies show associations between facial trauma and anxiety, depression, and PTSD. Several screening tools are available. Some institutions use multidisciplinary evaluations, support groups, and online resources.
11. Summary Algorithm
FACIAL TRAUMA PATIENT
|
Primary Survey (ABCDE)
|
A: Airway -- RSI preferred
Difficult airway? → Awake intubation, ketamine/etomidate
Failed? → Cricothyrotomy
|
B: Breathing -- rule out pneumothorax
|
C: Circulation -- direct pressure, nasal packing
Persistent hemorrhage? → OR / Embolization
|
D: Disability -- GCS, pupils, C-spine precautions
|
E: Exposure -- head-to-toe survey
|
Secondary Survey (only after primary is stable)
3 screening questions (vision, numbness, bite)
Systematic head-to-toe facial exam
|
Imaging: CT Face (gold standard)
|
Fracture-Specific Management:
- Frontal bone → Antibiotics ± OR
- Orbital blow-out → Canthotomy if compartment syndrome
- ZMC → Specialist + delayed OR
- Nasal → Drain septal hematoma; reduce 24-72h
- NOE → Admit neurosurgery + facial surgery
- Le Fort → Urgent airway then OR
- Mandible → Airway, then ORIF/IMF
|
Soft Tissue: Irrigate, débride, close; antibiotics selectively
|
Disposition: Admit complex/depressed fractures
Discharge simple isolated anterior fractures with follow-up
|
Psychosocial screening and rehabilitation referral
12. References
-
Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 9th ed. Chapter 259 (Facial Trauma), Table 259-1 and Table 259-2, pp. 1756-1762.
-
Rosen's Emergency Medicine: Concepts and Clinical Practice, 10th ed. Chapter 34 (Facial Trauma) by Ryanne J. Mayersak, pp. 401-426.
-
Cummings Otolaryngology: Head and Neck Surgery, 7th ed. Chapter on Facial Trauma and CT in Facial Trauma, pp. 190-197.
-
Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice, 21st ed. Damage Control Surgery section, pp. 304-316.
-
Current Surgical Therapy, 14th ed. Chapter: Airway Management in the Trauma Patient.
-
Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 1, Chapter on Facial Fractures.
-
Chen J, Vuong K, Balogh ZJ. "Early versus delayed fixation of maxillofacial fractures in polytrauma: a systematic review." Eur J Trauma Emerg Surg. 2026 Feb 23. PMID: 41729299
-
Wong ZY, Richards M, Wormald JCR. "Surgical site infection and patient-reported outcomes in surgically treated soft tissue facial injury: A meta-analysis." J Plast Reconstr Aesthet Surg. 2024 Aug. PMID: 38945111
-
Vaddamanu SK et al. "Impact of zygomaticomaxillary complex fracture on masticatory muscle dysfunction and pain: systematic review and observational meta-analysis." J Oral Facial Pain Headache. 2025 Sep. PMID: 41070564
Recent Evidence Note: A 2026 systematic review (PMID 41729299) on early versus delayed fixation of maxillofacial fractures in polytrauma found no current consensus favoring either approach, meaning individualized decision-making based on the patient's overall physiologic status remains the standard of care.
Discuss the primary management of Facial Trauma patient. give a deepdive answer about above topic with contents and references give the answer from the perspective of an oral and maxillofacial surgeon
Finding Sources
Finding Sources
Searching PubMed
"maxillofacial trauma" AND "surgical management"
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"mandibular fracture" AND "fixation"
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive OMFS-specific data from Bailey & Love, Scott-Brown's, and Schwartz's. Let me compile the full deep-dive answer from the oral and maxillofacial surgeon's perspective.
Primary Management of Facial Trauma: An Oral & Maxillofacial Surgeon's Perspective
Table of Contents
- Introduction and the OMFS Role
- Anatomy Relevant to OMFS Practice
- Initial Assessment - the OMFS Contribution to the Primary Survey
- Secondary Survey: The OMFS Craniomaxillofacial Examination
- Investigations and Imaging
- Dental and Dentoalveolar Injuries
- Soft Tissue Management
- Mandibular Fractures
- Midface (Maxillary / Le Fort) Fractures
- Zygomatic Complex Fractures
- Orbital Fractures
- Frontal Bone and Naso-orbito-ethmoid Fractures
- Panfacial Fractures
- Special Situations
- Post-operative Care and Rehabilitation
- Recent Evidence
- References
1. Introduction and the OMFS Role
From the oral and maxillofacial surgeon's perspective, the initial management of facial trauma requires a structured, systematic approach that balances the need for immediate life-saving interventions with the longer-term goals of restoring function and facial aesthetics. The OMFS occupies a unique position in the trauma team: trained in both medicine and dentistry, the specialty is the primary provider for mandibular, midface, and dentoalveolar injuries, and co-manages orbital, zygomatic, and frontal injuries alongside ophthalmology, neurosurgery, and plastic surgery.
OMFS involvement is typically triggered at the trauma call. However, even when another specialty leads the primary resuscitation, the OMFS should be contacted early -- because definitive management of bony injuries is time-sensitive and delays beyond 24-48 hours increase the risk of malunion, malocclusion, and secondary deformity.
2. Anatomy Relevant to OMFS Practice
The Facial Buttress System
The facial skeleton is organized into a system of vertical and horizontal buttresses that provide structural integrity and guide fracture patterns:
- Vertical buttresses (stronger): zygomaticomaxillary (lateral), nasomaxillary (medial), and pterygomaxillary (posterior)
- Horizontal buttresses (weaker): superior orbital rim, orbital floor, hard palate
All Le Fort-level fractures pass through the pterygoid plates posteriorly - a key anatomical constant.
The "Four-Legged Stool" of the Zygoma
The zygomatic bone is best conceptualized as having four "legs":
- The zygomatic arch (anteroposterior direction)
- The zygomatic process joining the frontozygomatic (FZ) suture (vertical)
- The infraorbital rim (horizontal)
- The zygomaticomaxillary buttress (vertical)
This model predicts fracture patterns and guides plating strategy.
Occlusion as a Surgical Guide
Unlike other facial surgeons, the OMFS uniquely uses pre-injury dental occlusion as the primary anatomic landmark for reducing maxillofacial fractures. The patient's own teeth and the pre-injury "bite" serve as the template for restoring facial form and function. Even a 1 mm discrepancy in occlusion detected by the patient is clinically significant.
3. Initial Assessment - the OMFS Contribution to the Primary Survey
The OMFS works within the ATLS framework. Life-threatening problems take absolute priority.
Airway
The OMFS is trained to manage the complicated maxillofacial airway. Critical principles:
- Bilateral posterior mandible fractures can cause posterior tongue displacement and complete upper airway obstruction - a surgical emergency. Grasping the tongue with suture or gauze and pulling anteriorly may be immediately life-saving.
- Midfacial fractures (Le Fort II/III) can cause complete separation of the midface from the skull base, with downward/backward rotation of the hard palate occluding the nasopharynx. Manual anterior traction on the mobile maxilla may temporarily restore the airway.
- Significant hemorrhage from the pterygoid plexus, sphenopalatine, and ethmoidal arteries can flood the pharynx. Up to 44% of severe maxillofacial trauma patients require intubation.
- Rapid-sequence intubation is preferred; always have cricothyrotomy equipment immediately available.
- Avoid nasotracheal intubation in suspected midface fractures -- risk of intracranial tube placement through a fractured cribriform plate.
- Submental intubation (passing the endotracheal tube through the floor of the mouth) is an OMFS-specific airway technique used in panfacial fractures where nasotracheal intubation is contraindicated and tracheostomy is undesirable -- it allows establishment of occlusion intraoperatively without compromising the airway.
Hemorrhage Control
- Pack the nasal cavity (posterior pack via Foley catheter + anterior layered gauze) for posterior epistaxis
- Apply direct pressure to external wounds; never blindly clamp vessels
- Maxillary fractures may be associated with significant bleeding from the pterygoid plexus
- Persistent arterial hemorrhage unresponsive to packing may require interventional radiology (embolization of external carotid branches) or operative ligation
4. Secondary Survey: The OMFS Craniomaxillofacial Examination
A systematic top-down approach is recommended, examining each anatomical unit in sequence.
History
- Mechanism of injury (predicts fracture patterns and associated injuries)
- Pre-injury dental history: presence of teeth, dentures, pre-existing malocclusion, orthodontic treatment
- Last meal (for anaesthetic planning)
- Tetanus status, medications (anticoagulants), allergies
Three Screening Questions (OMFS-focused)
- "How is your vision?" - any visual change mandates urgent ophthalmic review
- "Does your face feel numb?" - localizes nerve injury (supraorbital, infraorbital, mental nerve distribution)
- "Does your bite feel normal?" - even subtle malocclusion reliably indicates mandibular or maxillary fracture
Systematic Palpation (Top-Down)
Palpate in sequence: supraorbital ridge → lateral orbital wall → inferior orbital rim → zygomatic body → nasal bones → temporomandibular joint → rest of mandible bilaterally.
Oral Cavity Examination - the OMFS Hallmark
The oral cavity examination is uniquely emphasized by OMFS:
- Suction blood and secretions first; use a good light source
- Inspect for: mucosal lacerations, bruising, floor-of-mouth haematoma (pathognomonic for mandibular fracture), and palatal lacerations
- Dental examination: document all present teeth, avulsed teeth, luxated teeth, and fractures. Account for all missing teeth or tooth fragments - aspiration is a major risk and chest X-ray is required if any tooth is unaccounted for
- Occlusion assessment: altered occlusion (malocclusion) is the most reliable clinical sign of mandibular or maxillary fracture. The patient can detect even a 1 mm change. An anterior open bite suggests Le Fort-level midface fracture
- Step deformity on the gingival surface = mandibular fracture until proven otherwise (can be confused with a missing tooth by the inexperienced)
- Inferior alveolar nerve assessment: paraesthesia of the lower lip and chin = injury to the inferior alveolar nerve within the mandibular canal, or at the mental foramen
Retrobulbar Haemorrhage - OMFS Must Not Miss
A retrobulbar haemorrhage is an acute surgical emergency leading to blindness via pressure on the retinal artery and ischaemic optic nerve damage. Clinical signs:
- Tense proptosis
- Increasing periorbital pain
- Reduced visual acuity
- Loss of pupillary response
- Early sign: altered perception of red colour
Emergency treatment: lateral canthotomy and inferior cantholysis (can be performed by OMFS) to decompress the orbit immediately.
5. Investigations and Imaging
Standard Radiographs
| Suspected Injury | Recommended Views |
|---|---|
| Mandibular fracture | OPT (orthopantomogram) + PA mandible |
| Midface fracture | Occipitomental (OM) at 10° and 30° |
| Zygomatic fracture | OM views - look for maxillary sinus opacification |
| Cervical spine | AP/lateral cervical spine |
| Chest | PA chest (for aspirated teeth) |
Two views at right angles are mandatory to avoid missing any fracture on mandibular imaging (OPT + PA mandible). A lateral mandibular view may be substituted in uncooperative patients.
CT Scanning - Gold Standard
- Thin-section axial and coronal NCCT with 3D reconstruction is the gold standard for all significant facial trauma
- Mandatory for: suspected orbital fracture, high-impact injuries, Le Fort fractures, panfacial fractures
- 3D CT reformatting allows excellent visualisation of maxillofacial bony structures and is invaluable for surgical planning
- If head injury is suspected, include brain CT in the same acquisition
Specialist Tests
- Hess chart (orthoptic assessment) in all patients with diplopia - differentiates muscle entrapment from inflammatory muscle dysfunction
- Visual acuity testing (Snellen) before orbital examination
- Dental radiographs (periapical films) for dentoalveolar injuries
- Bailey and Love's Short Practice of Surgery, 28th ed., p. 430
6. Dental and Dentoalveolar Injuries
This is an area where the OMFS has unique expertise over all other specialties.
Classification
- Avulsion: tooth completely displaced from socket - dental emergency
- Luxation: tooth displaced but still attached to socket/periodontal ligament
- Intrusion: tooth driven apically into the socket
- Crown/root fractures: may or may not involve the pulp
- Alveolar fractures: segment of tooth-bearing bone displaced as a unit
Avulsed Tooth Management
The priority is replantation as quickly as possible. The extra-alveolar dry time is the strongest predictor of periodontal ligament cell survival.
- Ideal storage medium (if replantation not immediately possible): Hank's balanced salt solution, cold milk, or saline; the patient's buccal vestibule (saliva) is acceptable
- Do not scrub or dry the root surface
- Replant immediately, splint with a flexible splint for 7-14 days
- Open apex teeth in children: replantation should always be attempted
- Antibiotics (amoxicillin or doxycycline) and tetanus prophylaxis
Alveolar Fractures
Reduce the displaced segment under local anaesthesia and stabilize with an arch bar or acrylic splint for 4-6 weeks.
7. Soft Tissue Management
Facial Lacerations
- Examine the facial nerve function before administering local anaesthesia in all facial lacerations
- Nerve injuries lateral to a vertical line through the lateral canthus of the eye are repairable and should be repaired primarily under magnification and GA
- Nerve injuries medial to this line rarely need primary repair due to extensive facial nerve branching
Parotid Duct Injuries
The OMFS has specific responsibility for parotid duct injuries:
- The parotid (Stensen's) duct lies along the middle third of a line from the tragus of the ear to the midpoint between the upper lip and the alar base
- Injury is confirmed by injecting methylene blue through the duct opening intraorally (adjacent to the upper molar teeth) and observing leakage in the wound bed
- Repair under magnification over a cannula inserted through the intraoral duct opening; the buccal branch of the facial nerve closely parallels the duct and may also be injured
Animal and Human Bites
- Clean thoroughly, close primarily in layers
- Antibiotics according to local microbiology guidelines
- Human bites: consider HIV and hepatitis serology
- Significant tissue loss: staged reconstruction
General Wound Management Principles
- Use field blocks or facial nerve blocks rather than local infiltration (preserves wound edge anatomy)
- Irrigation in simple, clean wounds within 6 hours is generally not required
- For gaping wounds deeper than dermis: buried absorbable subcuticular sutures to eliminate dead space
- Tissue adhesive is acceptable for simple surface closure but contraindicated for mucosal surfaces and bite wounds
- Antibiotic prophylaxis is NOT required for simple facial wounds
- Bailey and Love's Short Practice of Surgery, 28th ed., p. 431
8. Mandibular Fractures
Mandibular fractures are among the most common facial fractures and represent the core of OMFS operative practice.
Anatomy and Fracture Patterns
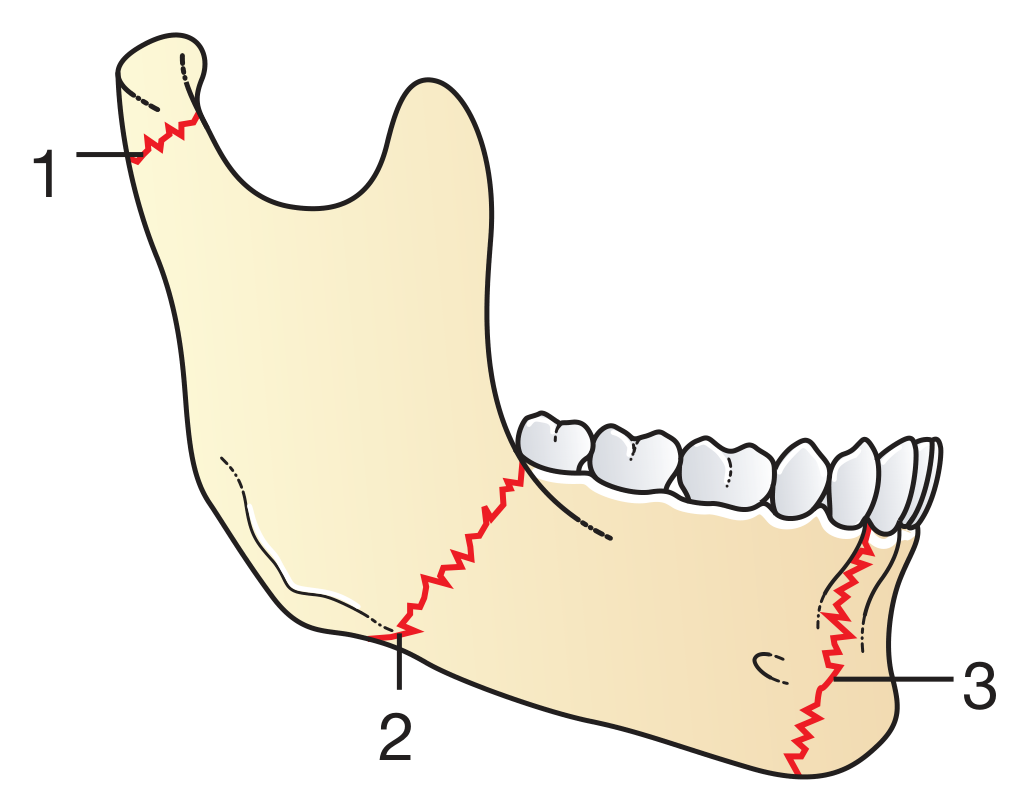
Fractures of the mandible: (1) condylar neck - the most common site, (2) angle of mandible, (3) mental foramen region. - Bailey and Love's, 28th ed.
The mandible is a curved bone with three points of weakness:
- Condylar neck (most common fracture site)
- Angle of mandible (second most common)
- Mental foramen region (parasymphysis)
Because of the curved ring-like architecture, contralateral double fractures are common (e.g., right angle + left condyle, right parasymphysis + left condyle). Always systematically look for a second fracture.
Clinical Signs (OMFS Focus)
- Malocclusion - the most reliable sign
- Floor-of-mouth haematoma - pathognomonic for mandibular fracture
- Step deformity on the alveolar ridge
- Inferior alveolar nerve paraesthesia (lower lip/chin) - implies fracture at or near the mental foramen or inferior alveolar canal
- Trismus (pain-limited mouth opening, masseter/medial pterygoid spasm)
- Abnormal mandibular mobility on bimanual palpation
Investigations
- OPT (orthopantomogram) + PA mandible (two views at 90°)
- CT with 3D reconstruction for complex or condylar fractures
Management by Fracture Type
Undisplaced/Minimally Displaced Fractures
Conservative management:
- Antibiotics (amoxicillin/co-amoxiclav) on admission
- Analgesia
- Soft diet for 4 weeks (bone healing time)
- Close outpatient follow-up to detect treatment failure (increasing pain, worsening malocclusion)
Displaced Fractures - ORIF
Open reduction and internal fixation (ORIF) using titanium miniplates and screws is the standard of care:
- Typically two 2-mm-diameter monocortical screws on each side of the fracture (load-sharing principle: fracture is reduced and load is shared between the bone and plate)
- Complex/comminuted fractures: heavy-profile reconstruction plates with bicortical screws (load-bearing fixation)
- Site-specific plate placement:
- Body/parasymphysis: single plate at the inferior border (Champy's principle); a second plate may be added at the superior border for added stability
- Angle fractures: single plate on the external oblique ridge (Champy's line of osteosynthesis)
- Symphysis: two parallel plates (superior and inferior)
- Performed under GA, with intraoperative IMF to establish correct occlusion before plate fixation
- Two to three post-operative IV antibiotic doses given
OPT showing ORIF with titanium miniplates:
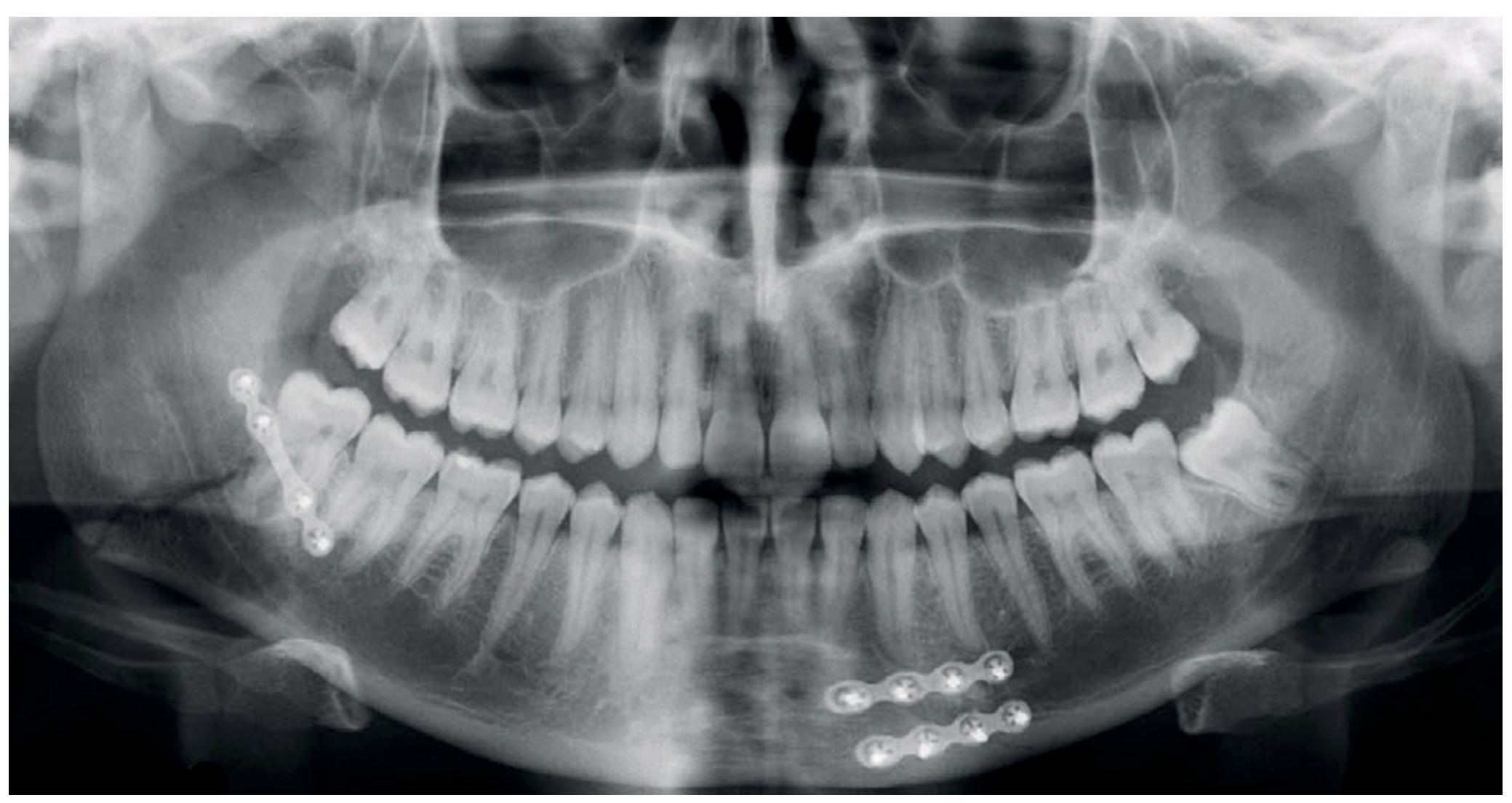
Post-operative OPT demonstrating fixation of a right angle and left parasymphyseal mandibular fracture with titanium miniplates and screws. - Bailey and Love's, 28th ed.
Intermaxillary Fixation (IMF)
- Becoming less common due to advances in rigid osteosynthesis
- Still indicated for severely comminuted fractures where plate fixation is technically unreliable
- Methods: arch bars + wire IMF, IMF screws (Stryker), cap splints (especially in paediatric dentition)
- Major drawback: prolonged IMF (4-6 weeks) is associated with gingival and dental disease, significant weight loss, and malnutrition; risk of aspiration in emergency situations
Temporary (Bridling Wire)
For heavily displaced fractures awaiting surgery, a bridle wire around the teeth can temporarily reduce fractures, reduce pain, and facilitate oral intake until definitive ORIF.
Optimal Timing
Within 24-48 hours post-injury is ideal. Delays allow progressive swelling, soft tissue fibrosis, early callus formation, and increasing difficulty of reduction.
Condylar Fractures
The condyle is the most commonly fractured part of the mandible. Management is debated:
- Most condylar fractures: closed reduction with IMF elastic guidance + strict soft diet + analgesia
- Displaced condylar neck fractures with significant loss of ramus height, dislocation, or foreign body (tooth/fragment) in joint space: increasingly managed with ORIF
- Surgical approaches: transparotid/retromandibular incision (most common), with advances toward endoscopic-assisted fixation in specialist units
- Bilateral condylar fractures: particular risk of anterior open bite, mandibular height loss, and airway compromise
- Bailey and Love's Short Practice of Surgery, 28th ed., p. 432
9. Midface (Maxillary / Le Fort) Fractures
Le Fort Classification
Maxillary fractures are classified according to the anatomic level described by René Le Fort (1901). All pass through the pterygoid plates.
| Level | Fracture Line | Clinical Hallmark |
|---|---|---|
| Le Fort I (transverse/Guérin) | Extends from pterygoid plates through lateral maxillary sinus wall and piriform aperture. Separates tooth-bearing maxilla from the rest of the face. | Mobile hard palate; malocclusion; "floating palate" |
| Le Fort II (pyramidal) | Extends from pterygoid plates to the infraorbital rim and across the nasal bridge. Involves the entire dentition-bearing maxilla and nasal bones. | Mobile midface; "donkey face" (elongated); infraorbital anaesthesia |
| Le Fort III (craniofacial disjunction) | Extends from pterygoid plates to the zygomatic arch bases, lateral orbit walls, FZ suture, and nasal bridge. The entire midface separates from the skull base. | Dish face; gross midface mobility; CSF rhinorrhoea |
Important caveat: In practice, fractures rarely follow a pure unilateral Le Fort pattern -- combinations and asymmetry are common due to comminution and differing force vectors. A patient may have Le Fort II on one side and Le Fort III on the other.
Clinical diagnosis by OMFS:
- Grasp the maxillary teeth/hard palate with one hand while stabilizing the forehead with the other and gently rock - movement confirms Le Fort-level fracture
- Assess the level of the fracture line by the pattern of movement:
- Palate alone mobile: Le Fort I
- Nose moves with palate: Le Fort II
- Whole midface (including orbits) moves: Le Fort III
Management
- Undisplaced/minimally displaced: soft diet and analgesia (conservative)
- Indications for ORIF: mobile/unstable maxilla, deranged occlusion (especially anterior open bite), loss of facial projection and width causing obvious deformity
- Fixation technique: midface 1.5-mm miniplates and screws placed along the main facial buttresses (optimal bone quality and screw purchase)
- Surgical access: varies with fracture level:
- Le Fort I: upper buccal sulcus incision (degloving the midface)
- Le Fort II/III: coronal incision (forehead flap) + lower eyelid/transconjunctival + upper buccal sulcus
- Occlusion first: establish correct dental occlusion (IMF) before plate fixation - this is the cornerstone of midface repair
- Associated nasal packing may be required for pterygoid plexus hemorrhage
- Bailey and Love's Short Practice of Surgery, 28th ed., p. 433
10. Zygomatic Complex Fractures
Anatomy (the "Four-Legged Stool")
The zygomatic bone articulates at four points, each potentially fractured:
- Zygomatic arch (temporal suture)
- Frontozygomatic (FZ) suture
- Infraorbital rim
- Zygomaticomaxillary buttress
Because the zygoma forms the lateral and inferior walls of the orbit and the superior lateral wall of the maxillary sinus, any displaced ZMC fracture is simultaneously an orbital and sinus fracture.
Clinical Examination
- Periorbital swelling and bruising (subconjunctival haemorrhage with no posterior limit = orbital floor fracture)
- Flattening of the malar eminence (may be masked by swelling - review at 1 week)
- Step deformity at infraorbital rim and/or frontozygomatic suture
- Trismus (masseter spasm or coronoid process impingement by displaced arch)
- Diplopia (orbital floor involvement)
- Infraorbital nerve anaesthesia (cheek, upper lip, nose numbness - infraorbital nerve in the canal)
- Subconjunctival haemorrhage with posterior extent not visible = strongly suggests orbital involvement
Investigations
- OM (occipitomental) views at 10° and 30°: look for maxillary sinus opacification (key radiological sign), step deformity of infraorbital rim, FZ suture diastasis
- CT with 3D reconstruction for displaced fractures, suspected orbital involvement, or when OM views are equivocal
- Hess chart if diplopia is present
Management
- Minimally displaced/no diplopia/no enophthalmos: conservative with explanation, no nose blowing for 2-3 weeks, review at 1 week for reassessment
- Review at 1 week: swelling subsides and true extent of displacement can be assessed
- Displaced fractures: operative reduction with or without fixation
Surgical Approaches to Zygoma
| Approach | Indication | Advantage | Disadvantage |
|---|---|---|---|
| Gillies temporal | Medially displaced body/arch | Distant from fixation site | Skin incision (visible in bald) |
| Dingman (coronal extension) | Medially displaced body | Uses same incision as FZ access | Difficult simultaneous plating and elevation |
| Poswillo hook | Posteriorly displaced (not arch) | Good mechanical advantage, quick | Stab scar on cheek |
| Keen (intra-oral) | Medially displaced/arch | No cutaneous scar | Cannot address FZ diastasis; theoretical oral contamination |
| Coronal | Laterally displaced arch | Only approach for this | Extensive exposure |
Fixation points: After elevation, the zygoma is plated at the FZ suture, infraorbital margin, zygomaticomaxillary buttress, and zygomatic arch. Meticulous periosteal closure over the plates is essential; some surgeons suture ("hitch") the deep tissue superiorly for better soft tissue support.
- Scott-Brown's Otorhinolaryngology, Vol. 1, Table 107.2, p. 1246
11. Orbital Fractures
Types
- Blow-out fracture (pure): only orbital walls; force transmitted through the fluid-filled globe fractures the weaker inferior or medial walls - fat, inferior rectus, or inferior oblique may herniate into maxillary/ethmoid sinus
- Blow-in fracture: rare; fragments driven into orbit, reducing orbital volume, causing proptosis
- Orbital fractures combined with ZMC/Le Fort: "impure" orbital fractures
White Eye Blow-out (Paediatric Emergency)
In children, the elastic bone may produce a trapdoor defect that opens, allows muscle herniation, then snaps shut - trapping the inferior rectus or inferior oblique. The orbit may look deceptively normal on imaging (minimal displacement). The child presents with:
- Restricted upward gaze + diplopia
- Oculocardiac reflex: bradycardia + nausea + syncope (vagal response to muscle traction)
- White, uninjured-looking eye (no subconjunctival haemorrhage)
This is a surgical emergency - irreversible muscle necrosis occurs within hours. Immediate surgical release is required.
Indications for Orbital Repair
- Persistent enophthalmos (>2 mm) or hypoglobus after swelling resolves (2-4 weeks)
- Persistent diplopia from muscle entrapment (confirmed by Hess chart and CT)
- Children: white eye blow-out = immediate surgery
- Large floor defect (>50% floor area) even without early symptoms - prophylactic repair to prevent late enophthalmos
Surgical Repair
- Access: transconjunctival (preferred - avoids visible scar, risk of entropion), subciliary, or lower eyelid
- Transconjunctival + cantholysis: excellent exposure, risk of lid malposition
- Transconjunctival + transcaruncular extension: access to medial wall
- Materials: preformed titanium mesh or patient-specific titanium implants (custom-made from CT data) are now the standard; autologous materials (cranial bone graft) are used less commonly
Retrobulbar Haemorrhage
This is a sight-threatening emergency and the OMFS must recognize and manage it urgently:
- Tense proptosis + increasing pain + reduced visual acuity + altered red colour perception
- Do not wait for CT confirmation -- act clinically
- Perform lateral canthotomy and inferior cantholysis immediately (incise the lateral canthal tendon and inferior crus to decompress the orbit)
- IV acetazolamide (500 mg) + IV methylprednisolone may be used as adjuncts
- Escalate immediately to ophthalmology
- Bailey and Love's Short Practice of Surgery, 28th ed., p. 434
12. Frontal Bone and Naso-orbito-ethmoid (NOE) Fractures
Frontal Bone Fractures
Require massive force. Strong association with TBI, C-spine injury, and additional facial fractures (craniofacial injury in 56-87% of cases).
Fracture classification:
- Anterior table only: OMFS management - discharge with decongestants, oral antibiotics (co-amoxiclav), follow-up with facial surgeon
- Posterior table (through-and-through): surgical emergency - neurosurgery + OMFS, operative repair to prevent CSF leak, pneumocephalus, mucopyocele, and empyema
- Frontal sinus obliteration: in some centres, the sinus is cranialized (posterior table removed, sinus obliterated with fat/bone) to prevent long-term mucopyocele
NOE Fractures
Central facial fractures involving nasal bones, ethmoid sinuses, and medial orbital walls. Often associated with:
- Lacrimal system disruption (epiphora)
- Traumatic telecanthus (widening of intercanthal distance due to detachment of medial canthal tendons)
- Dural tears with CSF rhinorrhoea
- Significant TBI
OMFS management: admit, joint care with neurosurgery, repair medial canthal tendons (transnasal canthopexy), reconstruct medial orbital walls, address nasal dorsum.
13. Panfacial Fractures
Panfacial fractures involve multiple facial thirds (upper, middle, and lower face) simultaneously. They represent the most technically demanding reconstructive challenge in OMFS.
Principles of Reconstruction
The standard sequence: "outside-in, top-down" or "bottom-up" approach, depending on the integrity of available stable reference points:
- Restore the skull base and cranial vault as the superior stable reference
- Reconstruct the midface (Le Fort level, orbital skeleton)
- Restore the mandible and dental occlusion
- Refine nasal and zygomatic architecture
The key anatomical reference is occlusion -- restoring the dental occlusion sets the vertical and anterior-posterior facial dimensions.
Airway Challenge
Standard orotracheal intubation prevents assessment of occlusion intraoperatively. Options:
- Nasal intubation (if no midface fracture)
- Submental intubation (OMFS technique): ETT passed through a stab incision in the floor of the mouth to the submental area - preserves both nasal access and the ability to check occlusion intraoperatively
- Tracheostomy (last resort)
Timing
- Definitive repair within 7-14 days (before callus formation makes reduction impossible without osteotomies)
- In polytrauma patients: may be delayed further; damage control surgery principles apply
A 2026 systematic review (PMID: 41729299) found no current consensus favouring early vs. delayed fixation of maxillofacial fractures in polytrauma, supporting individualized decision-making.
14. Special Situations
Paediatric Facial Fractures
- Facial bones are not fully mineralized; fractures may be incomplete (greenstick)
- Condylar fractures are more common proportionally; most are managed conservatively
- White eye blow-out is a paediatric emergency
- IMF with cap splints (covers the teeth) rather than arch bars in the mixed dentition
- Repair of fractures must account for potential impact on facial growth -- metallic plates in the growing face may impede development and plate removal is often planned
- A recent systematic review (PMID: 40515765) supports conservative management with cap splints for many paediatric mandibular fractures
Edentulous Patients
- Without teeth, the OMFS loses the primary landmark for fracture reduction (occlusion)
- Patients' dentures (if available) are used as occlusal splints and reference guides
- Fixation may require more plates/bone graft due to osteoporotic bone quality and reduced alveolar height
The Anticoagulated Patient
- Reverse anticoagulation before ORIF
- Increased risk of haematoma and airway compromise -- may require more aggressive monitoring
15. Post-operative Care and Rehabilitation
- Diet: liquid/soft diet for 4-6 weeks depending on fixation stability
- Oral hygiene: meticulous - chlorhexidine mouthwash, avoid brushing over plates initially
- Antibiotics: typically a short course of amoxicillin or co-amoxiclav post-operatively (3-5 days for most ORIF procedures)
- Physiotherapy: progressive mouth opening exercises (to prevent trismus and TMJ ankylosis) once adequate bone healing
- Follow-up: clinical and OPT review at 4-6 weeks, then 3 months, then 1 year
- Plate removal: titanium plates may be removed if they become symptomatic (cold intolerance, infection, palpability), typically after 12 months. Routine removal is not standard in adults but is more often considered in children.
- Dental rehabilitation: missing or fractured teeth may require endodontic treatment, dental implants, or prosthetic rehabilitation following complete fracture healing
- Psychological support: high rates of anxiety, depression, and PTSD after facial trauma; early screening with validated tools and multidisciplinary psychological support
16. Recent Evidence
| PMID | Study | Key Finding |
|---|---|---|
| 41729299 | Chen et al., Eur J Trauma Emerg Surg, 2026 | No consensus on early vs. delayed fixation in polytrauma; individualized approach warranted |
| 40222387 | Lal et al., J Oral Maxillofac Surg, 2025 | Systematic review/meta-analysis of fixation strategies for double mandibular fractures |
| 38604919 | Savani et al., Br J Oral Maxillofac Surg, 2024 | Comprehensive review of strategies for anterior mandibular fractures |
| 38336352 | Shah et al., J Oral Maxillofac Surg, 2024 | Intraoral vs. extraoral approaches for mandibular fracture repair show equal infection rates |
| 40515765 | Kumari et al., Oral Maxillofac Surg, 2025 | Cap splints remain an effective conservative option for paediatric mandibular fractures |
17. References
-
Bailey and Love's Short Practice of Surgery, 28th ed. Chapter 31 (Maxillofacial Injuries), pp. 428-436. CRC Press.
-
Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1. Chapter 107 (Zygomatic and Orbital Fractures), Table 107.2, pp. 1244-1247.
-
Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 9th ed. Chapter 259 (Facial Trauma), pp. 1756-1762.
-
Rosen's Emergency Medicine: Concepts and Clinical Practice, 10th ed. Chapter 34, pp. 401-426.
-
Schwartz's Principles of Surgery, 11th ed., Vol. 2. Section on Facial Fractures, pp. 2844-2860.
-
Chen J, Vuong K, Balogh ZJ. Early versus delayed fixation of maxillofacial fractures in polytrauma: a systematic review. Eur J Trauma Emerg Surg. 2026. PMID: 41729299
-
Lal B, Alagarsamy R, Chawla J. Outcomes of Different Internal Fixation Strategies for Double Mandibular Fractures: A Systematic Review and Meta-analysis. J Oral Maxillofac Surg. 2025. PMID: 40222387
-
Savani R, Weihsin H, Patel S. Effective strategies in the management of anterior mandibular fractures: a comprehensive systematic review. Br J Oral Maxillofac Surg. 2024. PMID: 38604919
-
Shah A, Perez-Otero S, Tran D. Infection Rates of an Intraoral Versus Extraoral Approach to Mandibular Fracture Repairs are Equal: A Systematic Review and Meta-Analysis. J Oral Maxillofac Surg. 2024. PMID: 38336352
-
Kumari N et al. Conservative management of pediatric mandibular fractures with cap splints: a systematic review. Oral Maxillofac Surg. 2025. PMID: 40515765
This is a shared conversation. Sign in to Orris to start your own chat.