Grades of atelectasis of ear and its management
Reading File
Finding Sources
Finding Sources
Searching PubMed
atelectasis ear tympanic membrane grading management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
I now have all the key content and images. Let me compile the comprehensive answer.
Atelectasis of the Ear (Middle Ear Atelectasis) - Grades and Management
Definition
Middle ear atelectasis refers to retraction of the tympanic membrane (TM) into the middle ear space due to longstanding eustachian tube (ET) dysfunction. Negative middle ear pressure causes the TM to collapse inward onto the ossicles and promontory. It represents a spectrum from simple retraction to full adhesive otitis media.
Key distinction:
- Atelectasis: TM retracted onto promontory/ossicles but the middle ear mucosal lining is still intact and the TM is NOT adherent to the medial wall
- Adhesive otitis media (Stage IV): Middle ear space totally obliterated, TM adherent to ossicles/promontory, mucosal surfaces lost
Sadé & Berco Classification (1976) - The Standard Grading System
This is the most widely used system, adapted by Cummings Otolaryngology:
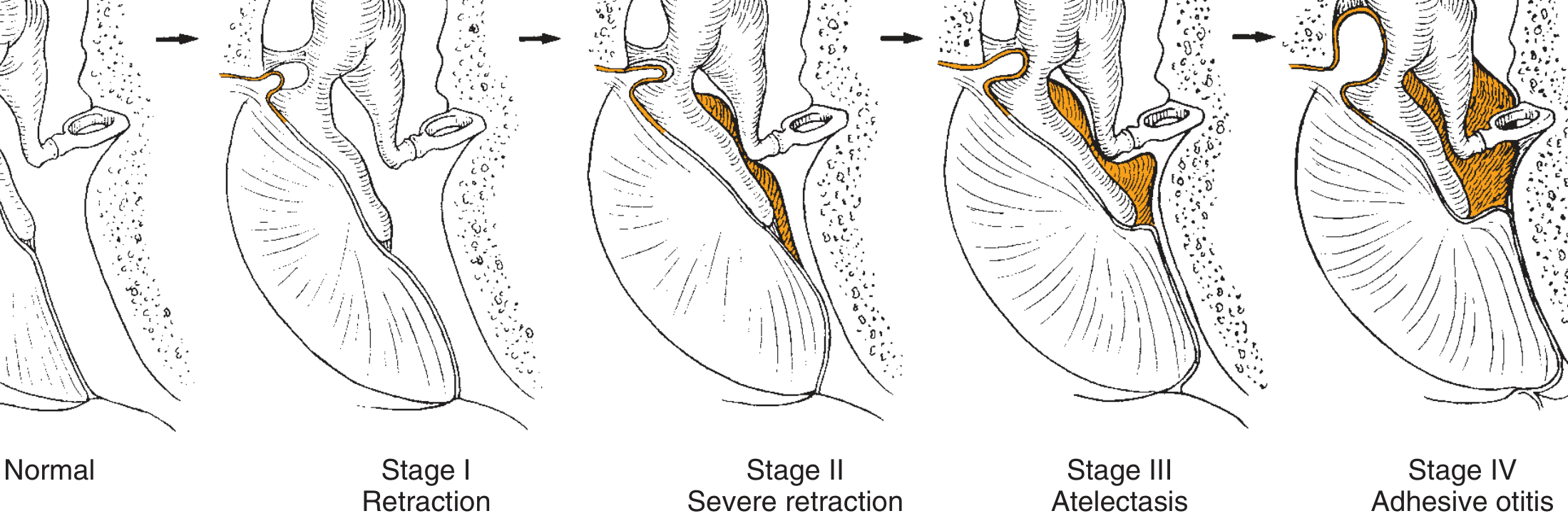
Fig. 140.3 from Cummings Otolaryngology: The four stages of middle ear atelectasis. (Adapted from Sadé J, Berco E, 1976)
| Stage | Description | Features |
|---|---|---|
| Stage I | Retracted TM | TM retracted but not touching incus; mild inward displacement |
| Stage II | Retraction with contact onto the incus | TM touches the incus/ossicular chain; still not adherent |
| Stage III | Middle ear atelectasis | TM retracted onto the promontory; middle ear space partially/completely obliterated but mucosa intact and TM is non-adherent |
| Stage IV | Adhesive otitis media | TM completely adherent to ossicles and promontory; middle ear space totally obliterated; mucosal surfaces lost |
- Cummings Otolaryngology Head and Neck Surgery, p. 2682-2683
Otoscopic appearance

Fig. 140.1 - Middle ear atelectasis with effusion (Cummings Otolaryngology)
Pathophysiology
The primary cause is eustachian tube dysfunction leading to:
- Loss of middle ear ventilation
- Development of negative pressure as middle ear mucosa absorbs nitrogen
- The posterior-superior pars tensa and pars flaccida are most vulnerable - they have thinner, more sparsely distributed collagen and increased vascular supply
- Inflammation and infection further damage collagenous support
- Progressive TM weakening and inward retraction
The atelectatic TM is histologically characterized by hyperkeratosis, edema and inflammation of the lamina propria, and loss of collagen organization.
- Shambaugh Surgery of the Ear, p. 2253-2268
Audiological Consequences
- Stages I-II: Minimal hearing loss
- Stage III: Conductive hearing loss up to 25 dB (as long as round window remains aerated and shielded)
- Stage IV / round window involvement: Air-bone gaps of 40-50 dB (loss of round window protection)
Red Flags / Warning Signs for Progressive Disease
- Deep retraction pocket where the medial extent cannot be visualized
- Conductive hearing loss
- Recurrent otorrhea
- Polypoid tissue or crusts covering a pocket
- "Trail sign" - a line of keratin extending from the pocket along the posterior EAC wall (may indicate cholesteatoma)
- These pockets are considered precursors to cholesteatoma
Management - By Stage
Stage I (Mild Retraction)
- Observation with routine microscopic exams to assess for progression
- Treat underlying ET dysfunction: manage allergy, adenoid disease, GERD
- Encourage autoinflation (Valsalva, Otovent balloon)
- Topical agents: acetic acid drops, mineral oil to prevent debris accumulation
- Monitor for progression
Stage II (Contact with Ossicles)
- All of the above
- Consider ventilating tube (tympanostomy tube) insertion - can reverse early atelectasis
- Sadé (1976) showed ventilating tubes improved atelectatic ears
- Laser myringotomy has also been used
Stage III (True Atelectasis)
- Tympanostomy tube insertion (may be difficult due to thinned lamina propria leading to early extrusion)
- Myringoplasty for reinforcement of the atelectatic TM, especially if hearing loss present
- Cartilage tympanoplasty - cartilage provides structural support resisting negative pressure
- Simple excision of the damaged TM segment (allows re-healing with thicker, stronger scar tissue)
- Laser-assisted contraction myringoplasty (Ostrowski & Bojrab technique) - addresses redundant/weakened atelectatic TM
Stage IV (Adhesive Otitis Media)
- Tympanoplasty (with or without ossiculoplasty)
- Cartilage tympanoplasty - preferred for reconstruction
- Tympanoplasty + mastoidectomy for complicated disease
- Ossicular chain reconstruction if erosion present (most commonly: long process of incus and stapes superstructure)
Note: Postoperative recurrence is not uncommon with any of these techniques, and thinning of the lamina propria makes tympanostomy tube retention tenuous.
- Shambaugh Surgery of the Ear, p. 2289-2296; Cummings Otolaryngology, p. 2683
Summary Table
| Stage | Description | Management |
|---|---|---|
| I | Simple retraction | Observation, autoinflation, treat ET dysfunction |
| II | Contact with incus | Ventilating tube, laser myringotomy |
| III | Atelectasis (non-adherent) | VT, myringoplasty, cartilage grafting, laser myringoplasty |
| IV | Adhesive otitis media (adherent) | Tympanoplasty ± mastoidectomy, ossicular reconstruction |
Key principle: The goal at every stage is to restore middle ear ventilation and prevent progression to cholesteatoma. Cartilage tympanoplasty provides the most durable repair because cartilage resists negative pressure far better than fascia or perichondrium alone.
Sources: Cummings Otolaryngology Head and Neck Surgery (Chapter 140); Shambaugh Surgery of the Ear; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2
This is a shared conversation. Sign in to Orris to start your own chat.