Discuss premalignant lesions of gastrointestinal tract
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Searching PubMed
premalignant lesions gastrointestinal tract review
I now have extensive material from authoritative textbooks. Let me compile the comprehensive answer.
Premalignant Lesions of the Gastrointestinal Tract
Premalignant (precancerous) lesions of the GI tract are conditions in which the mucosa undergoes structural or histological change that carries a statistically higher risk of malignant transformation than normal tissue. They span the entire length of the gut - esophagus, stomach, small intestine, and colorectum - and share a common theme: genetic/epigenetic accumulation of mutations often visible histologically as dysplasia.
1. ESOPHAGUS
A. Barrett's Esophagus (BE)
Barrett's esophagus is specialized columnar metaplasia replacing the normal squamous epithelium of the distal esophagus, occurring in the setting of chronic GERD. It is the single most important premalignant lesion of the esophagus, as it is the obligate precursor of esophageal adenocarcinoma.
Pathogenesis:
- Chronic gastroesophageal reflux damages squamous epithelium
- A process of "cellular reprogramming" driven by BARX1 and other developmental factors causes squamous-to-columnar metaplasia incorporating intestinal mucosa (goblet cells)
- Metaplastic Barrett cells first acquire a p53 mutation, then proceed via two molecular routes:
- Traditional pathway: stepwise accumulation in CDKN2A/p16, KRAS, and finally p53 loss
- Genome-doubled pathway (more rapid): p53-mutant cells undergo whole-genome doubling followed by genomic instability and oncogene amplification - thought to explain rapid cancer progression missed on surveillance
Dysplasia in BE:
- Dysplasia = histological expression of the genetic changes; categorized as low-grade dysplasia (LGD) or high-grade dysplasia (HGD)
- Endoscopically, dysplasia may appear as ulcerations, nodules, mucosal irregularities - but can be invisible to the naked eye
- Seattle biopsy protocol: four-quadrant biopsies every 1-2 cm of columnar-lined esophagus
- Advanced imaging: Narrow Band Imaging (NBI), chromoendoscopy, confocal laser endomicroscopy, volumetric laser endomicroscopy (VLE)
Management:
- Screening EGD indicated for patients with ≥10 years of GERD, even if symptoms are mild
- Periodic surveillance EGD with biopsies for all confirmed BE patients
- LGD: both periodic surveillance and endoscopic eradication therapy (EET) are acceptable
- HGD or intramucosal cancer: EET is the procedure of choice; esophagectomy only in unusual circumstances
- EET modalities: Radiofrequency ablation (RFA) - most common; Cryotherapy; Endoscopic mucosal resection (EMR); Endoscopic submucosal dissection (ESD)
- Harrison's Principles of Internal Medicine 22E, p. 1026; Yamada's Textbook of Gastroenterology 7e
B. Esophageal Squamous Dysplasia
- The precursor lesion of esophageal squamous cell carcinoma (ESCC), the most common esophageal malignancy worldwide
- Often requires specialized imaging for detection: chromoendoscopy with Lugol's iodine solution
- Population-based screening in high-incidence regions (China, Iran, Central Asia) has been shown to reduce ESCC occurrence
- Treatment when detected: EMR, ESD, or RFA
- Harrison's Principles of Internal Medicine 22E, p. 1030
2. STOMACH
A. Chronic Atrophic Gastritis + Intestinal Metaplasia (Correa Cascade)
The progression from normal gastric mucosa to gastric adenocarcinoma follows a well-characterized sequence:
Normal gastric mucosa → Chronic superficial gastritis (H. pylori) → Chronic atrophic gastritis → Intestinal metaplasia → Dysplasia → Carcinoma
Each step in this "Correa cascade" represents a premalignant condition:
- Chronic atrophic gastritis: loss of normal gastric glands, associated with H. pylori infection or autoimmune destruction (pernicious anemia). On endoscopy, disappearance of rugal folds, enhanced mucosal vasculature
- Intestinal metaplasia (IM): replacement of gastric mucosa with intestinal mucosa (goblet cells). Appears as gray-white patches on white-light endoscopy. A classic premalignant lesion. May represent reactivation of developmental intestinal programs
- Gastric dysplasia: the direct precursor to invasive carcinoma; classified as LGD or HGD
H. pylori and preneoplastic progression:
- H. pylori eradication is indicated for patients with preneoplastic lesions (atrophic gastritis or intestinal metaplasia)
- Evidence on regression of IM after H. pylori eradication is mixed; no significant difference in IM regression between treated and untreated H. pylori-negative IM patients at 2 years in RCT data
- A recent systematic review (Dinis-Ribeiro et al., Gut 2024, PMID 39122364) addresses worldwide guidelines for managing gastric intestinal metaplasia
Surveillance:
- Patients with atrophic gastritis/IM: EGD surveillance is recommended
- Testing and treatment for H. pylori is mandatory in all patients found to have premalignant gastric lesions
- Grainger & Allison's Diagnostic Radiology; Goldman-Cecil Medicine; Yamada's Textbook of Gastroenterology 7e
B. Gastric Adenomas (Gastric Polyps)
- True gastric adenomas are premalignant - risk correlates with size and degree of villous architecture
- Patients with Familial Adenomatous Polyposis (FAP) also develop gastric polyps (including fundic gland polyps and duodenal/gastric adenomas)
- Gastric carcinoma may develop remote from a hyperplastic polyp in areas of associated chronic inflammation
- Hyperplastic polyps per se carry low malignant potential but are a marker of the inflammatory milieu
- Schwartz's Principles of Surgery 11E
3. COLORECTUM
The colorectum is the site with the greatest burden of premalignant lesions in the GI tract.
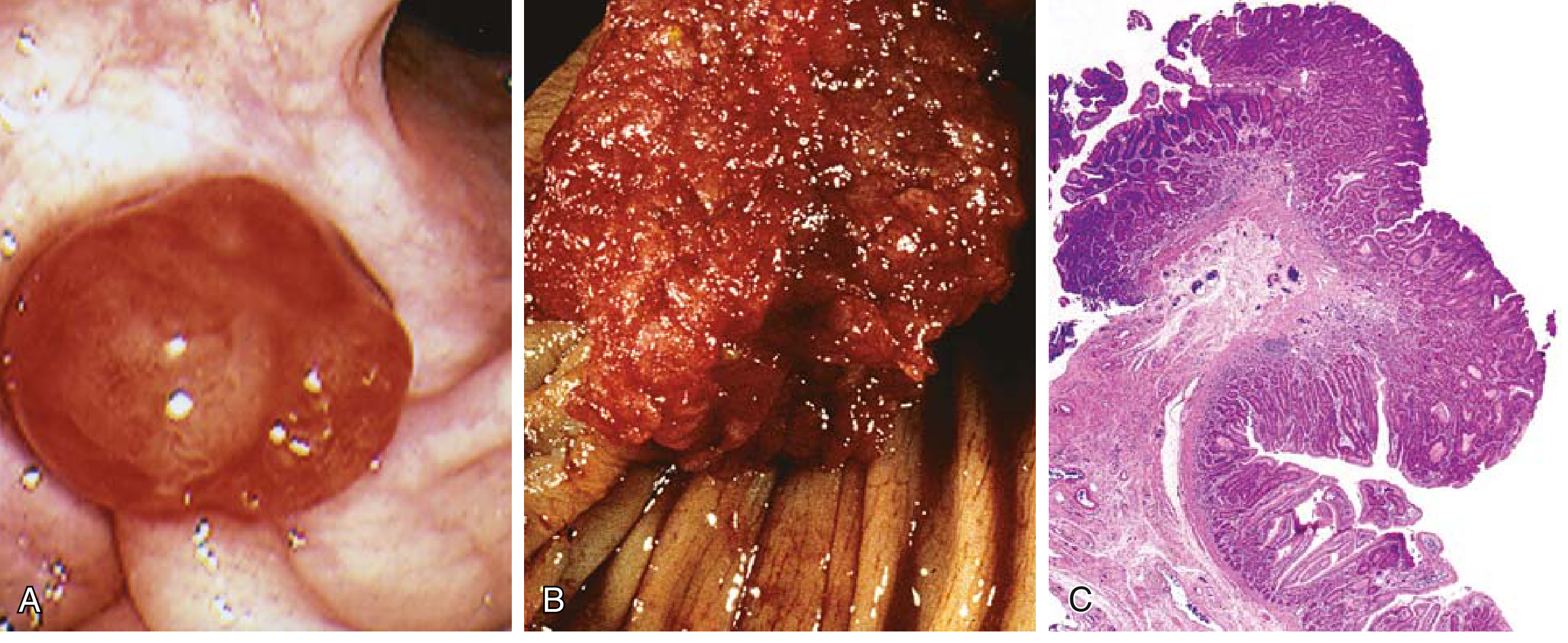
A. Adenomatous Polyps (Conventional Adenomas)
The most important premalignant lesions of the colorectum. The adenoma-carcinoma sequence is the dominant pathway for colorectal cancer (CRC) development, driven by sequential mutations in APC → KRAS → SMAD4 → p53.
Epidemiology:
- ~25% of Americans have adenomatous polyps by age 50; up to 50% of 70-year-olds
- <5% of adenomatous polyps are expected to progress to adenocarcinoma
- Development from polyp to invasive cancer typically takes 10-15 years
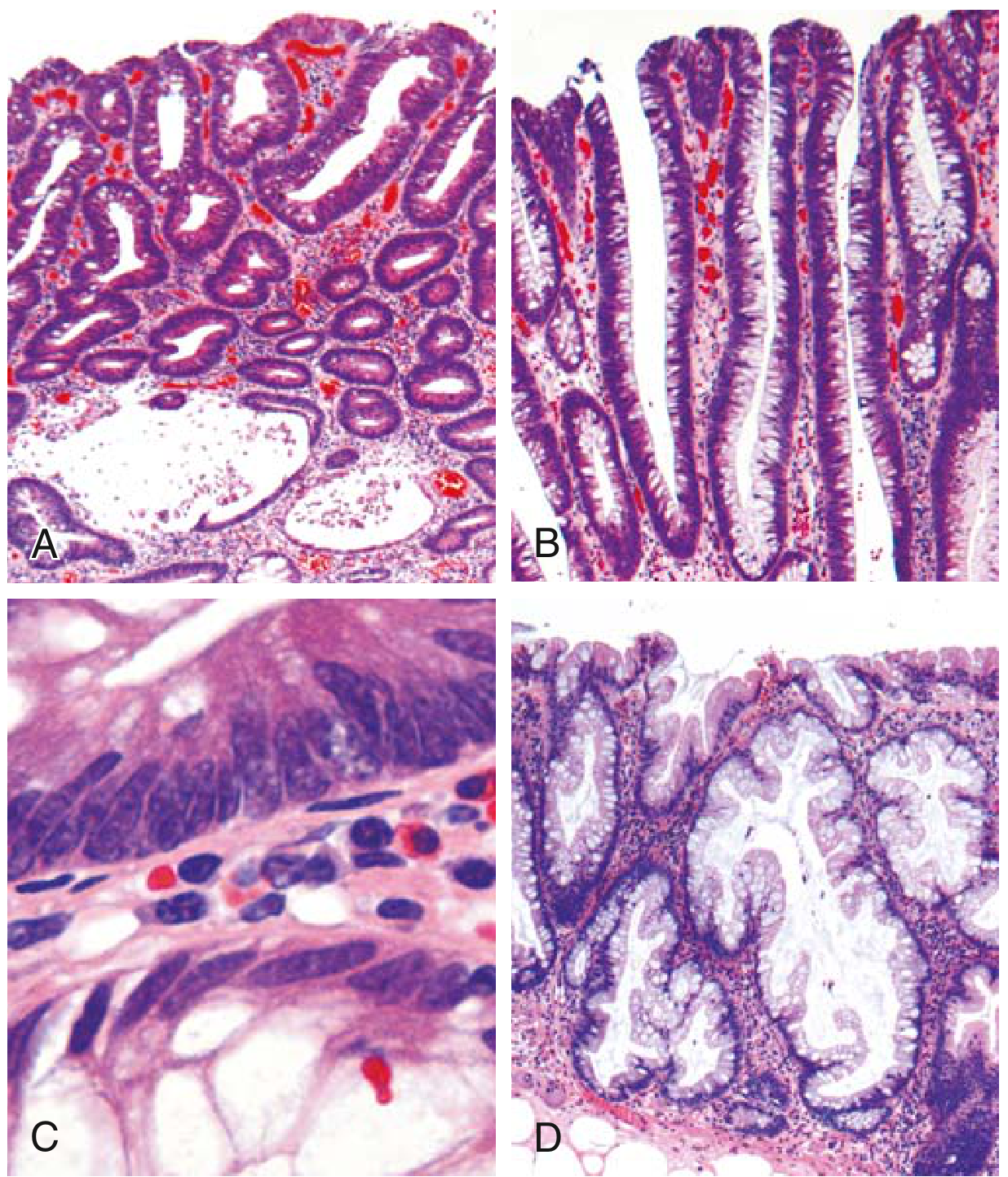
Classification by architecture:
| Type | Architecture | Features |
|---|---|---|
| Tubular adenoma | Small, rounded/tubular glands | Most common, often pedunculated, lower cancer risk |
| Villous adenoma | Long slender villi | Often large, sessile, highest cancer risk |
| Tubulovillous | Mixed | Intermediate risk |
| Sessile serrated adenoma (SSA) | Serrated throughout crypt base + lateral growth | Similar malignant potential to conventional adenomas despite lack of typical dysplasia |
Histology of dysplastic epithelium (Fig. 13.34C): increased nuclear-to-cytoplasmic ratio, hyperchromatic elongated nuclei, nuclear pseudostratification
Risk factors for malignant transformation:
- Size: Adenomas <1 cm - cancer extremely rare; adenomas >4 cm - up to ~40% contain invasive cancer
- Architecture: Villous adenomas develop cancer 3× more often than tubular adenomas
- High-grade dysplasia: Second major risk factor
Molecular pathways in CRC from adenomas:
- Chromosomal instability (CIN) pathway - most common; early APC loss, then KRAS/BRAF, then p53 loss
- Mismatch repair (MMR) deficiency/microsatellite instability (MSI-high) - underlying mechanism of Lynch syndrome; tumors sensitive to immune checkpoint inhibitors
- CpG island methylation (CIMP) - often right-sided, associated with MLH1 methylation; can be MSI-high or MSS
- Harrison's Principles of Internal Medicine 22E, p. 2614-2623; Robbins & Kumar Basic Pathology
B. Hyperplastic Polyps
- Common epithelial proliferations in the sixth-seventh decades
- Pathogenesis: decreased epithelial cell turnover → "pileup" of goblet cells
- The traditional view was that they are benign with no malignant potential
- However, sessile serrated adenomas (SSAs) - which overlap histologically with hyperplastic polyps - DO carry malignant potential and must be distinguished from simple hyperplastic polyps
- Key distinguishing feature: in SSA, serrated architecture extends through the full crypt length to the base, with crypt dilation and lateral growth; in hyperplastic polyp, serration is confined to the surface
C. Hamartomatous Polyposis Syndromes
These hereditary syndromes carry elevated cancer risk through associated dysplastic changes:
| Syndrome | Gene | GI Features | Cancer Risk |
|---|---|---|---|
| Familial Adenomatous Polyposis (FAP) | APC (5q21-22), autosomal dominant | Hundreds to thousands of colonic adenomas; gastric/duodenal polyps | Near 100% CRC if untreated; prophylactic colectomy required |
| Peutz-Jeghers Syndrome (PJS) | LKB1/STK11, autosomal dominant | Hamartomatous polyps throughout GI tract (especially small intestine) + mucocutaneous hyperpigmentation | Elevated risk of colon, pancreas, breast, lung, ovary, uterine cancers |
| Juvenile Polyposis | SMAD4/BMPR1A | Multiple juvenile polyps, usually rectum | Increased risk of colorectal adenocarcinoma (related to TGFβ/BMP pathway mutations) |
Note: FAP accounts for <1% of all CRC but is diagnosed in childhood (colonic polyps appearing in teenage years); prophylactic colectomy is the standard of care.
- Robbins & Kumar Basic Pathology; Harrison's Principles of Internal Medicine 22E
D. Colitis-Associated Neoplasia (IBD-associated dysplasia)
In both ulcerative colitis (UC) and Crohn's colitis, the risk of adenocarcinoma is elevated due to chronic mucosal inflammation driving a dysplasia-carcinoma sequence analogous to Barrett's esophagus.
Risk factors for dysplasia/cancer in IBD:
- Duration of disease: Risk begins to rise 8-10 years after diagnosis
- Extent of involvement: Pancolitis > left-sided or proctitis
- Severity and frequency of active inflammation (neutrophilic)
- Primary sclerosing cholangitis (PSC): Markedly greater risk; surveillance initiated at time of PSC diagnosis, not 8 years later
Surveillance:
- Colonoscopic surveillance recommended starting 8 years after IBD diagnosis
- Extensive mucosal biopsies required; dysplasia frequently occurs in flat mucosa that appears grossly normal
- Advanced endoscopic imaging (NBI, chromoendoscopy) helps target dysplastic areas
- Robbins & Kumar Basic Pathology, p. 766-777
4. HEREDITARY SYNDROMES - A FOCUSED SUMMARY
| Syndrome | Gene Mutation | Lesion Type | Malignancy Risk |
|---|---|---|---|
| FAP | APC | Thousands of colorectal adenomas | ~100% CRC without intervention |
| Lynch syndrome | MLH1, MSH2, MSH6, PMS2 | Fewer adenomas, but rapid progression | 40-80% lifetime CRC risk |
| Peutz-Jeghers | LKB1/STK11 | GI hamartomas | Colon, pancreas, breast, other |
| Juvenile polyposis | SMAD4, BMPR1A | Colorectal hamartomas | Colorectal carcinoma |
| MUTYH-associated polyposis | MUTYH (biallelic) | Multiple colorectal adenomas | CRC |
5. SUMMARY TABLE: PREMALIGNANT LESIONS BY GI SITE
| Location | Premalignant Lesion | Progression to |
|---|---|---|
| Esophagus | Barrett's esophagus (columnar metaplasia) | Adenocarcinoma |
| Esophagus | Squamous dysplasia | Squamous cell carcinoma |
| Stomach | Chronic atrophic gastritis | Gastric adenocarcinoma |
| Stomach | Intestinal metaplasia | Gastric adenocarcinoma |
| Stomach | Gastric dysplasia (LGD/HGD) | Gastric adenocarcinoma |
| Stomach | Gastric adenoma | Gastric adenocarcinoma |
| Colon/Rectum | Tubular/villous adenoma | Colorectal adenocarcinoma |
| Colon/Rectum | Sessile serrated adenoma | Colorectal adenocarcinoma |
| Colon/Rectum | IBD-associated dysplasia | Colorectal adenocarcinoma |
| Colon/Rectum | FAP polyps | Colorectal adenocarcinoma |
| Small intestine | Crohn's-associated dysplasia | Small intestinal adenocarcinoma |
| Small intestine | PJS hamartomas | Colorectal/other carcinomas |
Key Takeaways
- Dysplasia is the common histological endpoint of all GI premalignant lesions - it is the morphological manifestation of accumulated genetic/epigenetic mutations
- H. pylori drives the gastric premalignant cascade and eradication is mandatory in all patients with preneoplastic gastric lesions
- Polyp size and villous architecture are the two most important determinants of malignant risk in colorectal adenomas; lesions >4 cm harbor cancer in ~40% of cases
- Surveillance endoscopy with targeted biopsy is the cornerstone of management across all GI premalignant conditions
- Endoscopic eradication (RFA, EMR, ESD) has largely replaced surgery for esophageal dysplasia (Barrett's HGD) and is increasingly applied for gastric lesions
- Hereditary syndromes (FAP, Lynch, PJS) require genetic testing, family screening, and often prophylactic surgery
Sources: Robbins & Kumar Basic Pathology; Harrison's Principles of Internal Medicine 22E; Yamada's Textbook of Gastroenterology 7e; Goldman-Cecil Medicine; Sleisenger and Fordtran's GI and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.