Can u give the treatment for lichen planus pigmentation of the skin
Reading File
Finding Sources
Searching PubMed
"lichen planus pigmentosus" AND treatment
Searching the Web
lichen planus pigmentosus skin treatment 2024 2025
Finding Sources
Reading Article
PMID: 41642153
Reading Article
PMID: 37767951
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have comprehensive information to compile a detailed, well-structured answer. Here is the full response:
Lichen Planus Pigmentosus (LPP) - Treatment
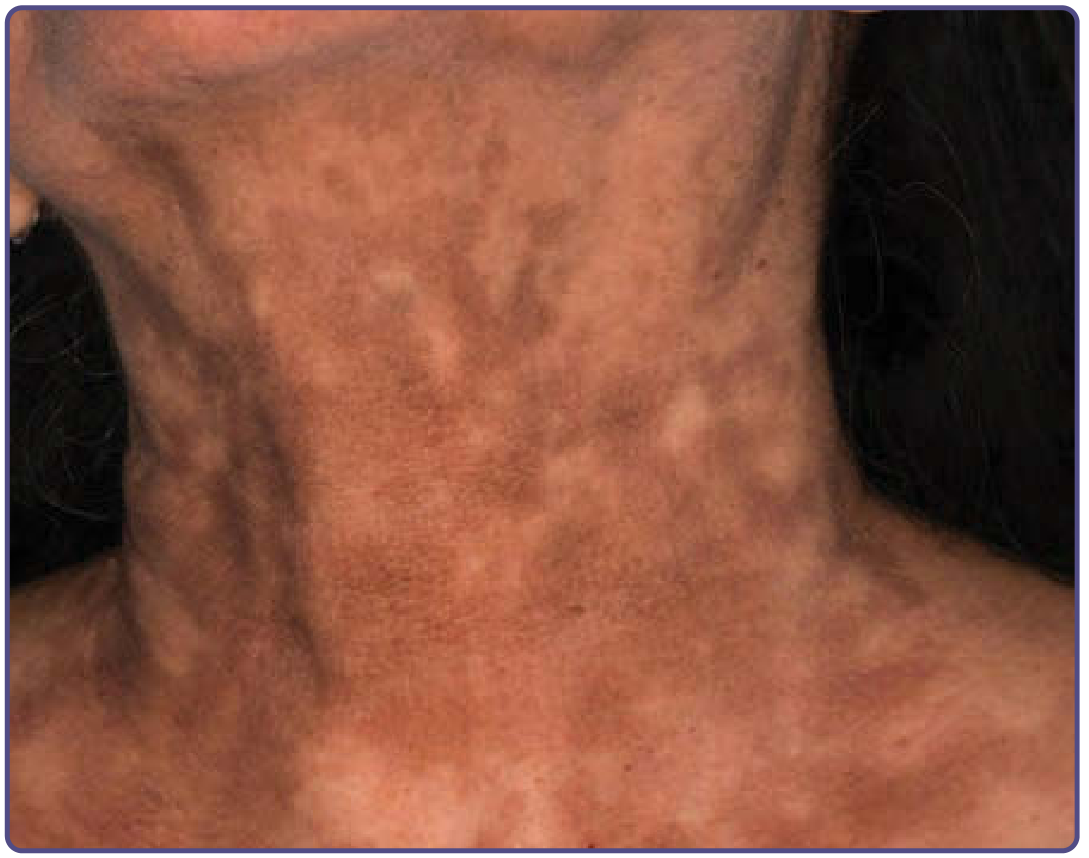
Lichen planus pigmentosus (LPP) is an acquired idiopathic dermal melanosis, considered a variant of lichen planus. It presents as symmetrical, poorly demarcated brown to gray-brown hyperpigmented macules mainly on photoexposed sites (forehead, temples, neck) and flexural folds. It predominantly affects darker-skinned individuals (South/Southeast Asians, Arabic populations). An important clinical reality: treatments provide only minimal improvement in pigmentation, and the condition is notoriously difficult to treat.
Here is a clinical image of LPP on the neck:
1. First - Identify and Remove Triggers
Before starting treatment, identify and eliminate potential causes:
- Mustard oil and amla (Indian gooseberry) oil (used in hair/cooking) are implicated triggers - these should be stopped
- Exclude drug-induced pigmentation (NSAIDs, antimalarials, psychotropics)
- Patch testing to exclude contact sensitization
2. Photoprotection (Mandatory in All Cases)
Photoprotection is critical and the single most important baseline measure. Broad-spectrum sunscreen (SPF 30 or higher) should be used daily, along with protective clothing, as UV exposure worsens pigmentation.
3. Topical Therapies
| Agent | Details |
|---|---|
| Tacrolimus 0.03% (calcineurin inhibitor) | Twice daily application; has shown improvement in LPP - one clinicopathological study by Al-Mutairi & El-Khalawany specifically assessed its response in LPP |
| Topical corticosteroids | Mild-to-moderate potency; can reduce inflammation but limited effect on established pigmentation |
| Topical vitamin A (retinoids) | May help; accelerates epidermal turnover and promotes pigment clearance |
| Topical depigmenting agents | Hydroquinone (2-4%), azelaic acid, kojic acid, niacinamide - used as adjuncts but limited evidence specific to LPP |
4. Systemic Therapies
| Agent | Details |
|---|---|
| Low-dose oral isotretinoin | 20 mg daily for 6 months with sunscreen; a prospective pilot study (Mathu SK et al., Int J Dermatol 2016) showed stabilization and decrease in pigmentation, especially when used early in the disease course |
| Oral corticosteroids | Short courses may suppress active inflammation; less useful for established pigmentation |
| Mycophenolate mofetil | Used for acquired dermal macular hyperpigmentation spectrum (which includes LPP); limited evidence, reserved for recalcitrant cases |
| Dapsone 100 mg/day | 8-12 week course; evidence from overlapping EDP/LPP spectrum |
5. Procedural / Cosmetic Interventions
A 2026 review in the Journal of Drugs in Dermatology (Ezekwe et al., PMID 41642153) - the most recent comprehensive review through December 2024 - assessed 16 studies on procedural options:
Chemical Peels:
- Glycolic acid peels (20-70%)
- Salicylic acid peels
- Phenol peels
- Jessner's solution / VI peel
- TCA (trichloroacetic acid) peels
- Often used in combination with topical retinoids; repeated sessions required; risk of post-inflammatory hyperpigmentation (PIH) in dark skin - use with caution
Laser Therapies:
- Q-switched Nd:YAG laser - most commonly studied; targets dermal melanin
- Fractional CO2 laser - promotes epidermal remodeling
- Picosecond Nd:YAG laser - newer modality with promising results
- 1550-nm erbium-doped fractional laser - used in combination with topical tacrolimus
Platelet-Rich Plasma (PRP): Emerging option; limited data but some reported improvement
Important caveat: All procedural evidence is based on small case series (most under 20 patients), no RCTs exist, and there is a real risk of PIH in darker skin types. These should be reserved for refractory cases.
6. Combination Approaches
Combination therapy tends to give better results than monotherapy:
- Topical tacrolimus + sunscreen
- Low-dose isotretinoin + sunscreen
- Chemical peel + topical retinoid
- Laser + topical tacrolimus (1550-nm erbium laser + tacrolimus ointment)
Prognosis
Some cases gradually resolve over many months, but this is the exception. Most cases are chronic. Treatment is aimed at stabilizing progression and achieving partial lightening rather than complete clearance.
Key takeaway: There is no single highly effective treatment for LPP. Management is stepwise: eliminate triggers → strict photoprotection → topical tacrolimus or retinoids → systemic isotretinoin if needed → procedural options for refractory cases. All therapies provide only partial improvement, and realistic patient counseling is important.
Sources: Fitzpatrick's Dermatology, 9th ed., Chapter 77 (Pigmentary Disorders); Chapter 32 (Lichen Planus and Lichenoid Dermatoses); Ezekwe et al. J Drugs Dermatol 2026 PMID 41642153; Shah et al. Int J Dermatol 2023 PMID 37767951
This is a shared conversation. Sign in to Orris to start your own chat.