Osteomyelitis
Reading File
Finding Sources
Searching PubMed
osteomyelitis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough response.
Osteomyelitis
Osteomyelitis is inflammation of bone and marrow, virtually always secondary to infection. It may complicate any systemic infection but frequently presents as a solitary primary focus. All organism types can cause it, but pyogenic bacteria and mycobacteria are the most common.
1. Routes of Infection
Three pathways allow organisms to reach bone:
- Hematogenous spread - the most common route in children; a bacteremia (even from minor mucosal injuries or skin infections) seeds the bone
- Contiguous spread - extension from adjacent soft tissue infection, cellulitis, or septic arthritis
- Direct implantation - penetrating trauma, open fractures, or orthopedic surgical procedures
- Robbins & Kumar Pathologic Basis of Disease; Bailey and Love's Short Practice of Surgery, p. 656
2. Pathogenesis & Anatomy
Why the metaphysis?
Infection starts in the metaphyses of long bones because of the slow flow through looped metaphyseal vessels, combined with microtrauma, which encourages bacterial seeding during bacteremia. In neonates, metaphyseal vessels penetrate the growth plate, so both the epiphysis and joint are frequently involved. In older children, the metaphysis is typical. After growth plate closure in adults, anastomoses between metaphyseal and epiphyseal vessels create routes for bacterial spread to subchondral regions.
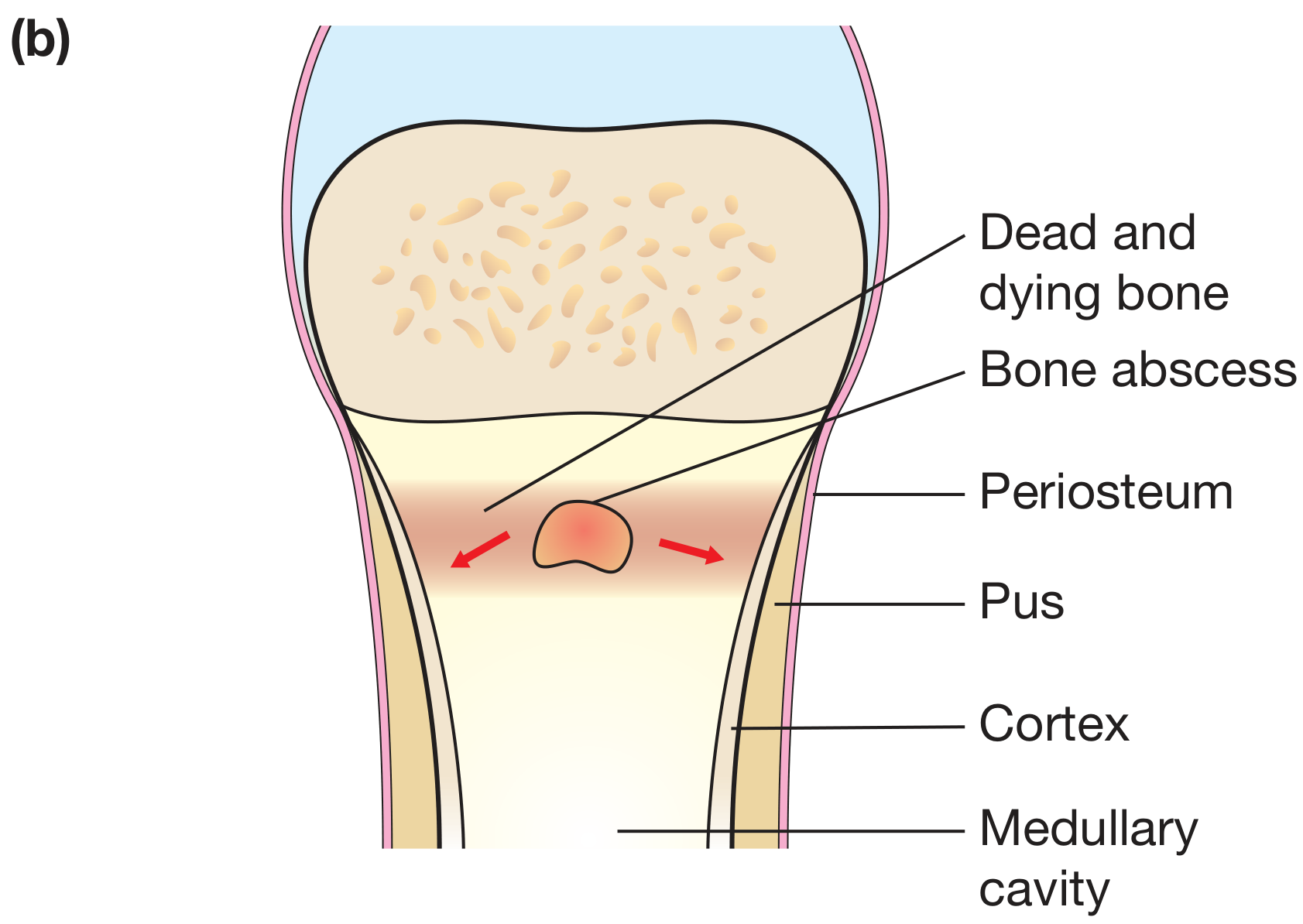
Figure: Bailey and Love's - Pathology of osteomyelitis: bone abscess, pus tracking through cortex, periosteal elevation
Sequence of events (acute phase):
- Bacteria proliferate → neutrophilic reaction
- Within 48 hours: necrosis of bone cells and marrow
- Bacteria spread through Haversian canals → reach periosteum
- In children, the loosely attached periosteum is elevated → subperiosteal abscess forms, dissecting along the bone surface
- Periosteal lifting further impairs blood supply → more necrosis
- Rupture of periosteum → soft tissue abscess → may track to skin as a draining sinus
- Epiphyseal spread → septic arthritis, articular cartilage destruction, permanent disability
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 779
3. Chronic Osteomyelitis - Key Structures
As infection evolves into the chronic phase, two characteristic structures form:
| Structure | What it is |
|---|---|
| Sequestrum | Dead, devitalized infected bone (avascular) |
| Involucrum | Shell of new reactive periosteal bone surrounding the sequestrum |
The "bone-within-a-bone" appearance on imaging results from the involucrum encasing the sequestrum. Pus tracks through gaps (cloacae) in the involucrum into soft tissues, eventually reaching the skin as sinus tracts.
Chronic infection shows: marrow fibrosis, sequestrum, and a chronic inflammatory infiltrate of lymphocytes and plasma cells on histology.
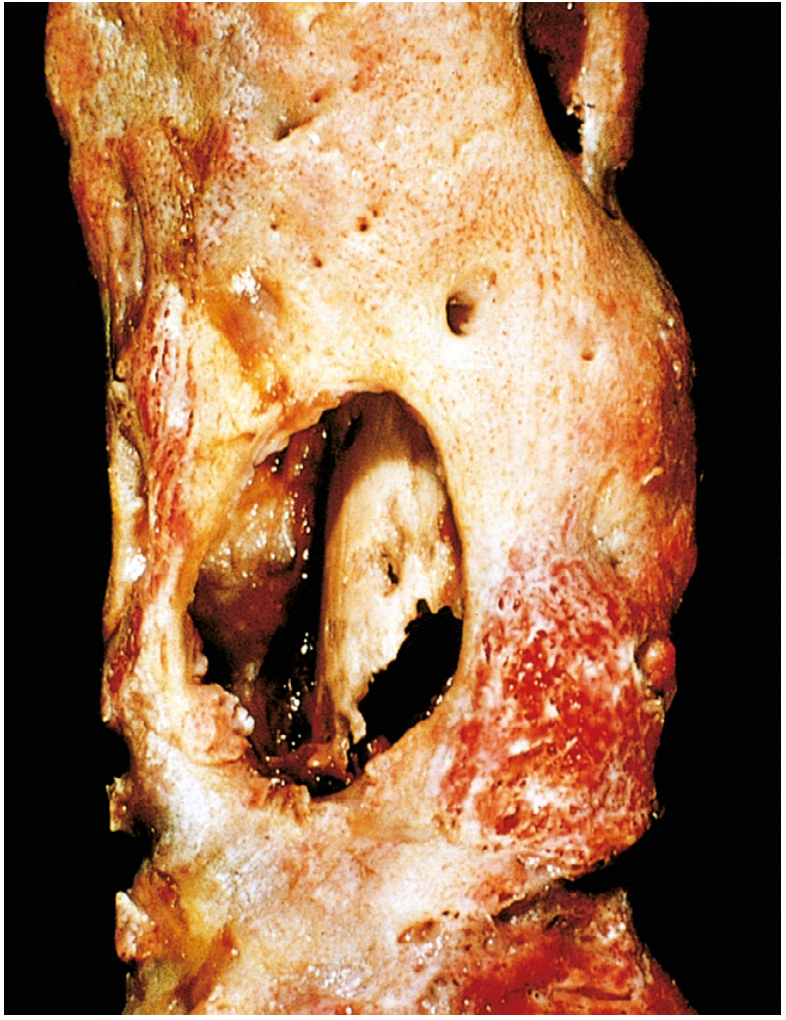
Fig. 26.16 - Robbins & Kumar: Resected femur with draining osteomyelitis. The drainage tract in the subperiosteal shell of viable new bone (involucrum) reveals the inner native necrotic cortex (sequestrum).
4. Microbiology
| Clinical Setting | Likely Organism(s) |
|---|---|
| Most common overall | Staphylococcus aureus (80-90% of culture-positive cases) |
| Neonates | Group B Streptococci, E. coli |
| Older children | S. aureus, Streptococcus pyogenes, H. influenzae |
| Sickle cell disease | Salmonella spp. (+ other gram-negatives) |
| Open fractures / surgery | Mixed bacterial infections |
| Diabetic foot | Polymicrobial |
| Post-penetrating injury | Pseudomonas aeruginosa (e.g., nail through shoe) |
| IV drug users | S. aureus, gram-negatives, Pseudomonas |
| Vertebral osteomyelitis | S. aureus (most common), gram-negatives |
| Immunocompromised | Mycobacteria, fungi (Candida, Aspergillus, Coccidioides, Blastomyces) |
S. aureus adheres to bone matrix collagen via cell wall proteins - a key virulence mechanism. No specific organism is identified in approximately 50% of patients even with cultures; PCR assays are improving this.
- Robbins & Kumar Pathologic Basis of Disease; Grainger & Allison's Diagnostic Radiology
5. Special Forms
Brodie Abscess
A subacute/chronic form - appears as a well-defined lytic lesion with a sclerotic rim, typically in the metaphysis of long bones. Represents a localized intraosseous abscess.
Vertebral Osteomyelitis (Spondylodiscitis)
- More common in adults; lumbar and cervical vertebrae most frequently affected
- Often accompanied by paravertebral or epidural abscess
- Back pain + neurological signs (radicular pain, sensory loss, weakness, urinary retention, bowel/bladder incontinence) = emergency
Tuberculous Osteomyelitis (Pott's Disease)
- More destructive and resistant to control than pyogenic osteomyelitis
- Affects ~1-3% of individuals with pulmonary/extrapulmonary TB
- Classic sites: spine (Pott's disease), and weight-bearing joints
- Tuberculous dactylitis (spina ventosa): cyst-like cavities with diaphyseal expansion, more common in hand bones
- Presents with localized pain, low-grade fever, chills, weight loss
- Robbins & Kumar; Grainger & Allison's Diagnostic Radiology
6. Clinical Features
Acute hematogenous osteomyelitis:
- Systemic illness: malaise, fever, chills, leukocytosis
- Intense throbbing pain over the affected bone, point tenderness
- Only ~60% are febrile at initial evaluation
- Raised inflammatory markers (ESR, CRP, WBC)
- In infants: unexplained fever may be the only sign
Chronic osteomyelitis:
- Punctuated by spontaneous flares after years of dormancy
- Draining sinus tracts
- May be relatively indolent
- Robbins & Kumar; Rheumatology (2-Volume Set)
7. Investigations
| Investigation | Role |
|---|---|
| Plain radiograph | Changes lag 2 weeks behind onset; shows soft tissue swelling, cortical irregularity, periosteal reaction, lytic destruction |
| MRI | Gold standard - hypointense on T1, increased signal on T2; identifies marrow edema, soft tissue extension, epidural/paravertebral abscess; penumbra sign in subacute infection |
| Ultrasound | Useful in children; detects subperiosteal fluid, guides aspiration |
| CT | Defines cortical destruction, identifies sequestra |
| Bone scintigraphy | Whole-body scan useful for multifocal disease (especially in neonates) |
| Blood cultures | Positive in ~50% of hematogenous cases |
| Bone biopsy + culture | Required for definitive pathogen identification |
| ESR, CRP, WBC | Elevated; used to monitor treatment response |
- Grainger & Allison's Diagnostic Radiology; Rheumatology (2-Volume Set)
8. Management
Medical
- Antibiotics are the cornerstone
- Empiric coverage should target S. aureus; adjust based on culture results
- MRSA common in some areas; Panton-Valentine leukocidin (PVL)-positive strains increase morbidity
- Duration is debated; generally 4-6 weeks minimum for hematogenous osteomyelitis
- Oral vs IV route: Recent evidence (2025 meta-analysis, PMID: 40280255) supports oral antibiotics being non-inferior to IV for bone and joint infections in selected patients who are clinically improving
Surgical
- Drainage of pus when present (subperiosteal or intraosseous abscess)
- Debridement - removal of all nonviable/necrotic tissue
- Sequestrectomy - removal of sequestrum in chronic cases
- Rest/splintage of the affected limb
- Analgesia
Surgical indications:
- Failure to respond to antibiotics within 24-48 hours
- Presence of abscess (subperiosteal or soft tissue)
- Concurrent septic arthritis
- Chronic osteomyelitis with sequestrum
- Bailey and Love's Short Practice of Surgery, p. 657; Rheumatology (2-Volume Set)
9. Complications
| Complication | Notes |
|---|---|
| Chronic osteomyelitis | 5-25% of acute cases; delayed diagnosis, inadequate treatment |
| Septic arthritis | Via direct spread; cartilage destruction, permanent disability |
| Growth disturbance | Physeal damage in children; growth arrest, angular deformity |
| Pathologic fracture | Weakening of bone by infection/necrosis |
| Secondary (reactive) amyloidosis | With long-standing chronic infection |
| Draining sinus tracts | May develop squamous cell carcinoma (Marjolin's ulcer) |
| Sarcoma | Rare; in chronically infected bone |
| Sepsis / bacteremia | With hematogenous seeding |
| Endocarditis | Via bacteremia |
- Robbins & Kumar Pathologic Basis of Disease, p. 1093
10. Recent Evidence Update
A 2025 systematic review and meta-analysis (PMID: 40280255) confirmed that oral antibiotics are non-inferior to IV antibiotics for bone and joint infections in patients who are clinically and haematologically improving - supporting early switch from parenteral to oral therapy.
A 2025 systematic review (PMID: 40607967) identified major risk factors: diabetes mellitus, immunosuppression, peripheral vascular disease, open fractures, orthopedic hardware, and prior osteomyelitis.
Sources: Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease; Bailey and Love's Short Practice of Surgery 28e; Grainger & Allison's Diagnostic Radiology; Goldman-Cecil Medicine; Rheumatology 2-Volume Set; Campbell's Operative Orthopaedics 15e (2026)
This is a shared conversation. Sign in to Orris to start your own chat.