A middle age gentlena woth cholestatic jaundice with normal mrcp with total and died t bilutubin ajove 20 mg/dl with probable malena was admitted and started on octreotide infusion high dose ppis the next day mornjn he debeloed svere epigadyric pwub and vomiting usg is normql what could be the differentials
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
octreotide infusion acute pancreatitis cholecystitis side effects jaundice
Finding Sources
Finding Sources
Finding Sources
Here is a structured clinical analysis of this case:
Clinical Summary (Reconstructed from Your Description)
Patient: Middle-aged man
Admission diagnosis: Cholestatic jaundice (Total bilirubin >20 mg/dL, Direct bilirubin elevated) with probable melena
MRCP: Normal
USG: Normal
Treatment started: Octreotide infusion + high-dose PPIs
New symptom next morning: Severe epigastric pain + vomiting, USG still normal
Differential Diagnoses for the New Epigastric Pain + Vomiting
1. ACUTE PANCREATITIS - Most Likely Drug-Induced
This is the top priority differential given the timeline.
- Octreotide is a known (though rare) cause of acute pancreatitis - it can occur within the first hours to days of starting an infusion. This is well-documented in product literature. The Canadian product monograph explicitly states: "Acute pancreatitis has been reported within the first hours or days of octreotide."
- The mechanism: octreotide causes biliary sludge, increases bile lithogenicity, and can trigger sphincter of Oddi dysfunction leading to pancreatic ductal hypertension.
- USG can be normal in early acute pancreatitis (sensitivity of USG is only ~60-70% in early disease). CT abdomen with contrast is the gold standard.
- Workup: Serum amylase + lipase (3x ULN = diagnostic), urgent CECT abdomen.
2. ACUTE ACALCULOUS CHOLECYSTITIS
- Octreotide markedly inhibits gallbladder contractility and reduces bile flow. This promotes gallbladder stasis and sludge formation - a well-established risk (27% gallstone rate, 24% sludge rate even on short-term use per drugs.com data).
- Acalculous cholecystitis can occur with bile stasis even without stones - and importantly, USG can be normal or near-normal early in acalculous disease.
- More common in critically ill, hospitalized patients.
- Workup: HIDA scan (most sensitive), repeat USG with wall thickness/Murphy's sign assessment, hepatobiliary CT.
3. ASCENDING CHOLANGITIS (Charcot's / Reynolds' Triad)
- The patient already has cholestatic jaundice with Tbili >20 and melena. Even though MRCP was normal initially, dynamic biliary obstruction (stone passing, stricture flare, biliary sludge post-octreotide) can cause ascending cholangitis.
- Octreotide itself has been associated with cholangitis in the literature.
- Epigastric/RUQ pain + jaundice already present + fever (if present) = Charcot's triad.
- Workup: Fever check, blood cultures, LFTs trend, WBC, repeat imaging, consider ERCP.
4. PPI-RELATED OR DRUG-INDUCED GASTROPARESIS / Severe Dysmotility
- High-dose IV PPIs can occasionally cause severe nausea/vomiting and epigastric discomfort.
- Less likely to cause "severe" pain but worth considering as a contributing factor.
- PPIs can mask a duodenal ulcer perforation by reducing acid - pain may be partially treated but obstruction or bleeding persists.
5. PERFORATED PEPTIC ULCER (Partial or Contained)
- The patient had melena, suggesting upper GI bleed - likely a pre-existing peptic ulcer.
- A contained microperforation or posterior perforation (pancreatic penetration) would cause severe epigastric pain but may have normal free gas on USG (especially posterior perforations).
- Normal USG does NOT rule out perforation - you need an erect CXR (free subdiaphragmatic air) or CT.
- Workup: Erect CXR, urgent CT abdomen with oral contrast.
6. SPHINCTER OF ODDI DYSFUNCTION (SOD) / FUNCTIONAL BILIARY PAIN
- Given normal MRCP, SOD is a reasonable underlying diagnosis. Octreotide can paradoxically worsen SOD by altering sphincter tone in some patients.
- Presents with recurrent biliary-type epigastric pain, elevated enzymes, normal imaging.
7. ISCHEMIC HEPATITIS / HEPATIC INFARCTION
- In a jaundiced patient with possible GI bleeding, hemodynamic instability could reduce hepatic perfusion.
- Octreotide causes splanchnic vasoconstriction - rarely, this can compromise hepatic arterial flow.
- Consider if transaminases suddenly spike.
8. REACTIVATION / WORSENING OF UNDERLYING HEPATIC PATHOLOGY
- Bilirubin >20 with normal MRCP suggests intrahepatic cholestasis (drug-induced liver injury, viral hepatitis, autoimmune hepatitis, acute alcoholic hepatitis, etc.).
- The original cause may be worsening (e.g., hepatitis flare).
Key Workup to Order RIGHT NOW
| Investigation | Rationale |
|---|---|
| Serum lipase + amylase | Rule out acute pancreatitis (most urgent) |
| Erect CXR | Rule out free air (perforation) |
| CECT abdomen | Gold standard - pancreatitis, cholecystitis, perforation |
| CBC + CRP + Procalcitonin | Infection/cholangitis |
| LFTs + coagulation profile | Hepatic status |
| Blood cultures x2 | If fever - cholangitis/sepsis |
| Blood glucose | Octreotide-induced hypoglycemia/hyperglycemia |
Clinical Bottom Line
Stop or hold octreotide infusion while the workup is ongoing - it is the most likely iatrogenic trigger. The combination of:
- Drug-induced acute pancreatitis (octreotide, within 24 hrs)
- Drug-induced gallbladder stasis/acalculous cholecystitis (octreotide)
- Ascending cholangitis on background of cholestatic jaundice
...are the top three differentials. Normal USG does NOT exclude any of these in the first 24 hours. A CECT abdomen + serum lipase is the single most important next step.
Sources: Octreotide hepatobiliary adverse effects - LiverTox/NCBI | Octreotide pancreatitis product monograph | Yamada's Textbook of Gastroenterology, 7th ed. | Harrison's Principles of Internal Medicine, 22nd ed.
So mrcp is only for extraheoatic ciplestaisa
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Great question - this is a common misconception. Here is the precise answer:
What MRCP Actually Detects - and What It Misses
MRCP's Core Strength: Biliary Tree Anatomy
MRCP visualizes the entire biliary ductal system - intrahepatic bile ducts, common hepatic duct, common bile duct, cystic duct, pancreatic duct, and the ampulla. So it can detect:
- CBD stones (choledocholithiasis)
- Biliary strictures (benign or malignant)
- Bile duct dilatation
- Primary sclerosing cholangitis (PSC) - intrahepatic AND extrahepatic
- Choledochal cysts
- Pancreatic duct pathology
So MRCP does cover some intrahepatic biliary pathology - specifically the larger intrahepatic ducts.
What MRCP CANNOT See - and Why a Normal MRCP Does NOT Rule Out Cholestasis
| Cause of Cholestasis | Visible on MRCP? | Why |
|---|---|---|
| CBD stone / stricture | Yes | Ductal level pathology |
| PSC (larger ducts) | Yes (beading pattern) | Ductal level |
| Cholangiocarcinoma | Yes (stricture/mass) | Ductal level |
| Drug-induced cholestasis | No | Canalicular / hepatocyte level |
| Viral hepatitis | No | Hepatocellular level |
| Alcoholic hepatitis | No | Hepatocellular level |
| Primary biliary cholangitis (PBC) | No | Destroys small interlobular ducts - below MRCP resolution |
| Intrahepatic cholestasis of sepsis | No | Functional / canalicular |
| Autoimmune hepatitis | No | Hepatocellular |
| Infiltrative disease (lymphoma, sarcoid, amyloid) | No | Parenchymal |
| PSC early small duct disease | No | Small ducts below resolution |
The Core Principle
MRCP rules out LARGE DUCT obstruction (extrahepatic + large intrahepatic ducts). A normal MRCP means the bile ducts are NOT dilated or obstructed - it says NOTHING about hepatocyte function, canalicular transport, or small duct disease.
Harrison's 22nd edition is explicit: "False-negative results occur in patients with partial obstruction of the common bile duct or in patients with cirrhosis or PSC, in which scarring prevents the intrahepatic ducts from dilating."
Practical Implication for Your Patient
This patient has:
- Tbili >20, cholestatic pattern
- Normal MRCP - means no large duct obstruction
- Therefore the cause is almost certainly intrahepatic cholestasis
The correct diagnostic pathway after a normal MRCP for cholestatic jaundice:
- AMA (Anti-mitochondrial antibody) - for Primary Biliary Cholangitis
- ANA, ASMA, IgG - for Autoimmune Hepatitis / AIH-PBC overlap
- Drug history - DILI is one of the most common causes
- LFT pattern - Hepatitic (high AST/ALT) vs pure cholestatic (high ALP/GGT)
- Liver biopsy - if no cause found (gold standard for intrahepatic cholestasis)
- pANCA, IgG4 - for PSC small duct disease, IgG4 cholangiopathy
- Viral serology - Hep A/B/C/E, EBV, CMV
In short: MRCP = biliary anatomy scan. It does not assess hepatocyte function or canalicular transport. A normal MRCP should redirect your workup toward intrahepatic causes, not reassure you that there is no serious pathology. - Yamada's Textbook of Gastroenterology, 7th ed. | Harrison's Principles of Internal Medicine, 22nd ed.
Anatony of bikiary tree
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a complete account of biliary tree anatomy from the surgical and gastroenterology textbooks:
Anatomy of the Biliary Tree
Overview Diagram
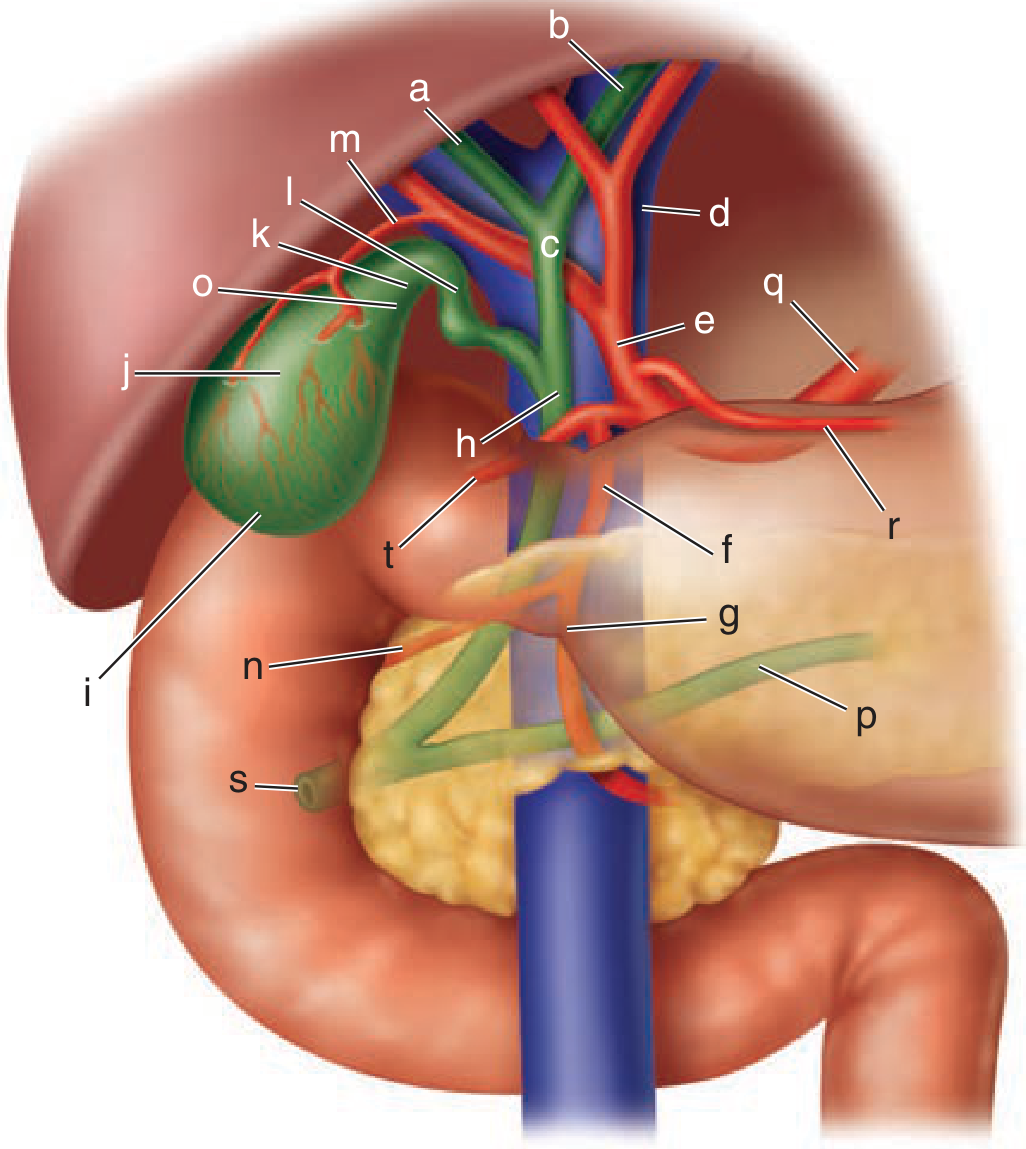
Key: a = right hepatic duct, b = left hepatic duct, c = common hepatic duct, d = portal vein, e = proper hepatic artery, f = gastroduodenal artery, h = common bile duct, i = fundus of gallbladder, j = body, k = infundibulum, l = cystic duct, m = cystic artery, s = ampulla of Vater, p = pancreatic duct
(Schwartz's Principles of Surgery, 11th ed.)
1. Intrahepatic Bile Ducts
Bile is formed at the level of the hepatocyte canaliculi - the smallest channels between hepatocytes. These drain into:
- Bile canaliculi (between hepatocytes)
- Canals of Hering (transition zone, connects canaliculi to bile ductules)
- Bile ductules / cholangioles (periportal)
- Interlobular bile ducts (run with portal triads)
- Segmental intrahepatic ducts - drain Couinaud segments I-VIII
- Right anterior sectoral duct (segments V, VIII) + Right posterior sectoral duct (segments VI, VII) → unite to form the Right hepatic duct
- Left hepatic duct (segments II, III, IV + caudate/segment I usually drains here)
The intrahepatic ductal confluence branching pattern:
- True bifurcation (right + left meet): ~60%
- Trifurcation (right anterior, right posterior, left all meet): ~12%
- Right sectoral duct crossing to join left hepatic duct: ~28%
2. Hepatic Ducts (at the Hilum)
Right hepatic duct:
- Shorter than the left (0.5-2.5 cm)
- Formed just below the porta hepatis (95% of cases)
- In 5%, the ducts join within liver substance
Left hepatic duct:
- Longer and more superficial than the right
- Greater propensity for dilatation in distal obstruction
Common hepatic duct (CHD):
- Formed by union of right + left hepatic ducts - usually ~1 cm below porta hepatis
- Length: 2-6.5 cm
- Diameter: ~4 mm
- Position: anterior to portal vein, to the right of the hepatic artery
- Lies in the hepatoduodenal ligament (free edge of lesser omentum)
- The confluence lies anterior to the right branch of the portal vein
3. Triangle of Calot (Hepatocystic Triangle)
A critical surgical landmark:
- Superior border: hilum of the liver
- Right border: cystic duct
- Left border: common hepatic duct
Contents running through it:
- Right hepatic artery
- Cystic artery
- 90% of accessory hepatic ducts
- 95% of aberrant right hepatic arteries
This is why careful dissection is essential during cholecystectomy.
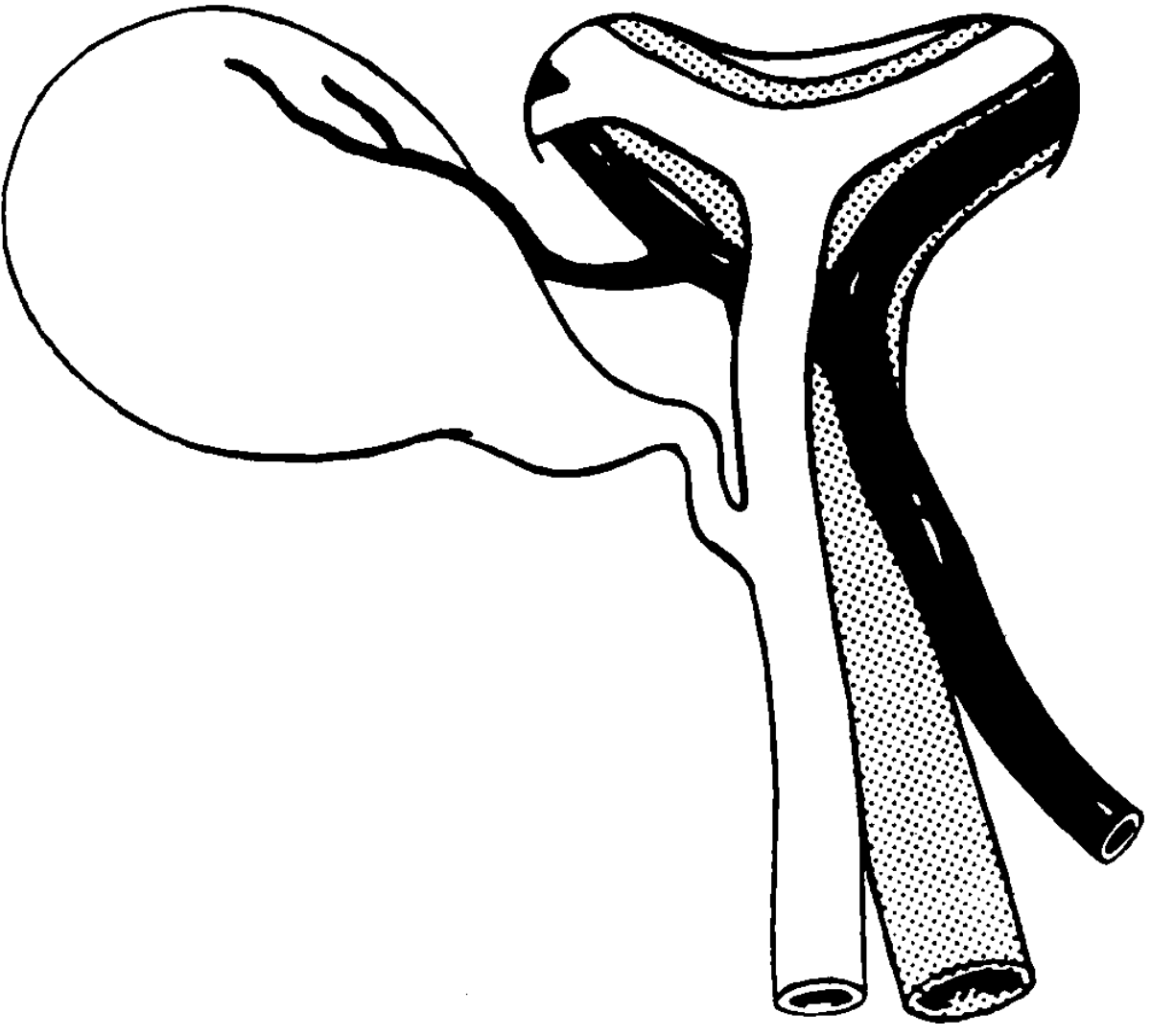
4. Cystic Duct
- Arises from the neck of the gallbladder
- Length: 0.5-8 cm (highly variable)
- Lumen: 1-3 mm (occasionally up to 10 mm - allows stones to pass into CBD)
- Contains spiral valves of Heister (mucosal folds - no true valvular function but make cannulation difficult)
- Most commonly (70%) joins CHD directly on the right side
Cystic duct variations (surgically important):
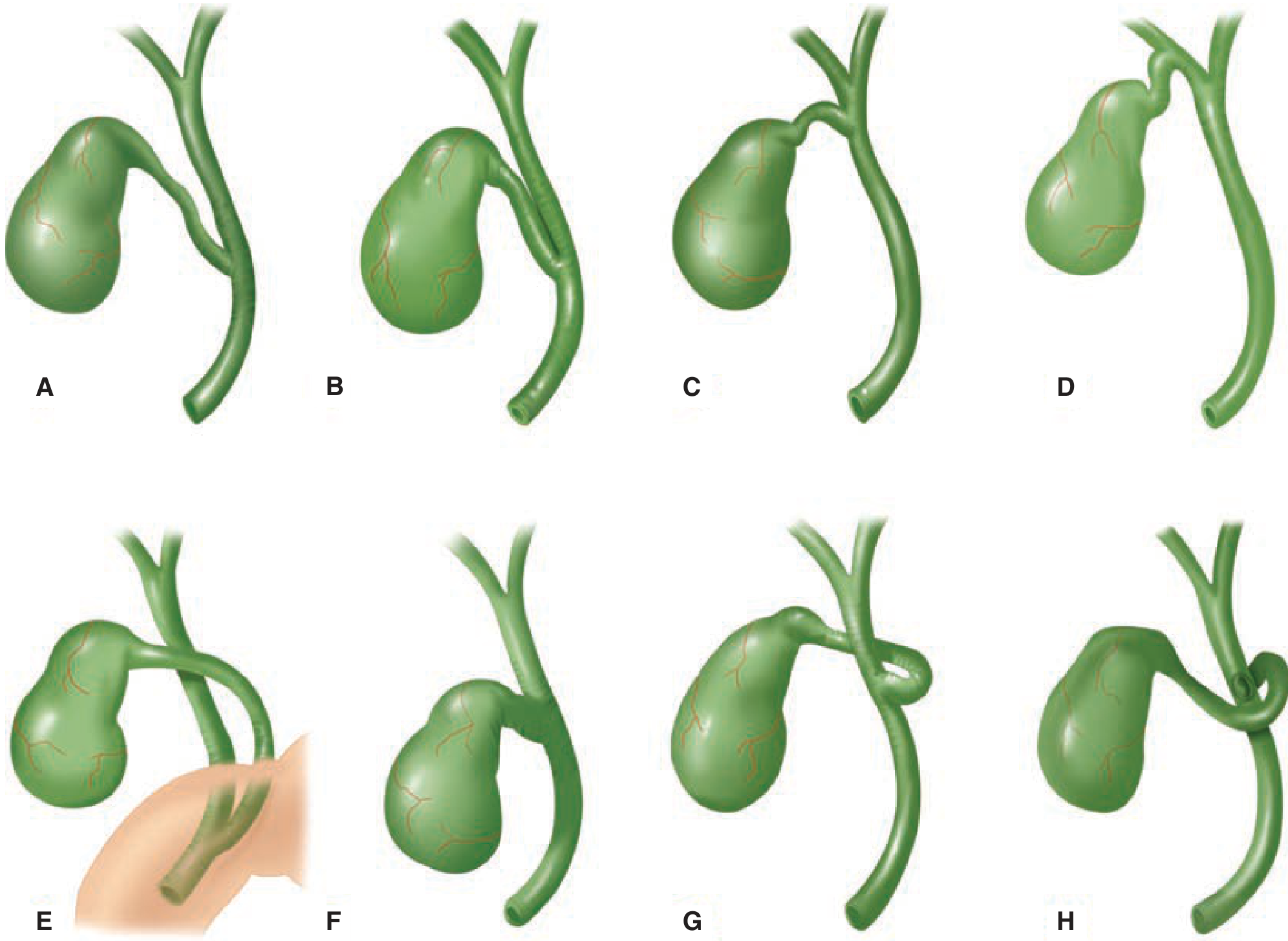
- A: Normal low junction with CHD
- B: Cystic duct adherent to CHD (parallel course)
- C: High junction
- D: Drains into right hepatic duct
- E: Long cystic duct joining behind the duodenum
- F: Absent cystic duct
- G: Crosses posterior to CHD, joins anteriorly
- H: Courses anterior to CHD, joins posteriorly
5. Common Bile Duct (CBD)
Begins where the cystic duct meets the CHD. Total length: 7-11 cm, diameter: 5-10 mm (up to 8 mm is normal; may enlarge slightly with age and after cholecystectomy).
The CBD has three anatomical segments:
| Segment | Location | Relationships |
|---|---|---|
| Supraduodenal (upper third) | Free edge of hepatoduodenal ligament | Right of hepatic artery, anterior to portal vein |
| Retroduodenal (middle third) | Behind 1st part of duodenum | Diverges from portal vein and hepatic arteries |
| Pancreatic (lower third) | Behind/through head of pancreas | Groove or tunnel in pancreatic head → enters 2nd part of duodenum |
The CBD runs obliquely 1-2 cm within the wall of the duodenum before opening at the ampulla of Vater (papilla of Vater), approximately 10 cm distal to the pylorus.
6. Junction with Pancreatic Duct - Ampulla of Vater
The CBD and main pancreatic duct (of Wirsung) unite in one of three ways:
| Pattern | Frequency |
|---|---|
| Unite outside duodenal wall → single common channel through wall | ~70% |
| Join within duodenal wall → short or no common channel, but single opening | ~20% |
| Separate openings into duodenum | ~10% |
The sphincter of Oddi surrounds the ampulla and controls bile and pancreatic juice flow. It has three components: sphincter choledochus, sphincter pancreaticus, and sphincter ampullae.
7. Gallbladder
- Pear-shaped reservoir, 7-10 cm long, capacity ~50 mL
- Parts: Fundus → Body → Infundibulum (Hartmann's pouch) → Neck → Cystic duct
- Lies in the gallbladder fossa on the inferior surface of the liver (segments IV/V)
- Hartmann's pouch is the dependent part of the infundibulum - where stones commonly lodge
- Blood supply: Cystic artery (usually from right hepatic artery, within Calot's triangle)
- The ducts of Luschka (subvesical ducts) run adjacent to the gallbladder fossa and can be injured during cholecystectomy, causing bile leaks
Clinical Correlations
| Structure | Clinical Relevance |
|---|---|
| CBD normal diameter | <6 mm on USG; up to 8-10 mm post-cholecystectomy or with age |
| Retroduodenal CBD | Posterior duodenal ulcer can erode into it causing hemobilia |
| Pancreatic segment | Pancreatic head cancer / chronic pancreatitis compresses CBD here |
| Low cystic duct insertion | Risk of misidentification as CBD during laparoscopic cholecystectomy |
| Triangle of Calot | Most common site of bile duct injury during cholecystectomy |
| Ampulla of Vater | Gallstone impaction → obstructive jaundice + acute pancreatitis |
Sources: Yamada's Textbook of Gastroenterology, 7th ed. | Schwartz's Principles of Surgery, 11th ed. | Grainger & Allison's Diagnostic Radiology | Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.