Sime way to understand MI in ecg
Reading File
Finding Sources
Searching Images
myocardial infarction ECG changes ST elevation STEMI leads
Finding Sources
Searching Images
ECG localization MI territory leads inferior lateral anterior posterior
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Now I have rich textbook content and real ECG images. Let me compile a comprehensive, easy-to-understand answer.
MI on ECG — A Simple, Systematic Guide
The Core Concept: What Happens in MI?
When a coronary artery is blocked, the affected heart muscle goes through three concentric zones:
- Ischemia (outer) → T-wave changes
- Injury (middle) → ST-segment changes
- Necrosis (inner) → Q-wave changes
Each has its own ECG signature, and they evolve over time.
Step 1 — The 3 Classic ECG Changes
| Finding | What it looks like | What it means | When it appears |
|---|---|---|---|
| Hyperacute T waves | Tall, peaked, broad T waves | Very early ischemia | Minutes |
| ST elevation | ST segment lifts above baseline (convex/tombstone shape) | Acute transmural injury | Minutes–hours |
| Pathologic Q waves | Wide (≥40 ms) and deep (≥25% of R) Q | Myocardial necrosis | 8–12 hours (sometimes <1 hr) |
| T-wave inversion | Narrow, symmetric, deep T inversion | Ischemia or post-injury evolution | Hours–days |
| ST depression | ST droops below baseline | Subendocardial ischemia / reciprocal change | Variable |
ST elevation morphology matters: STEMI shows flat/convex (tombstone) ST elevation. Benign causes (early repolarization, pericarditis) tend to have concave ("smiley face") ST elevation. — Rosen's Emergency Medicine
Step 2 — STEMI Diagnostic Criteria (Harrison's 22e)
New ST elevation at the J-point in ≥2 contiguous leads:
- All leads except V2–V3: ≥ 1 mm (0.1 mV)
- V2–V3 in men ≥40 y: ≥ 2 mm
- V2–V3 in men <40 y: ≥ 2.5 mm
- V2–V3 in women: ≥ 1.5 mm
(Source: Fourth Universal Definition of MI, 2018)
Step 3 — Localize the MI by Leads
This is the most practical skill. Think of the 12 leads as cameras pointing at different walls:
| Territory | Leads with ST Elevation | Reciprocal Depression | Artery |
|---|---|---|---|
| Anterior | V1–V4 | III, aVF | LAD |
| Anterolateral | V1–V6, I, aVL | III, aVF | LAD (proximal) |
| High lateral | I, aVL | III, aVF, V1 | LCx or 1st diagonal |
| Lateral | V5, V6, I, aVL | — | LCx |
| Inferior | II, III, aVF | I, aVL | RCA (90%) or LCx |
| Posterior | ST depression V1–V3 + tall R/T in V1 | — (it IS the reciprocal) | RCA or LCx |
| Right ventricular | V1 + right-sided leads (V3R, V4R) | — | Proximal RCA |
Always get right-sided leads (V3R, V4R) in inferior STEMI to rule out RV involvement — fluid management changes completely. — Rosen's Emergency Medicine
Step 4 — ECG Examples
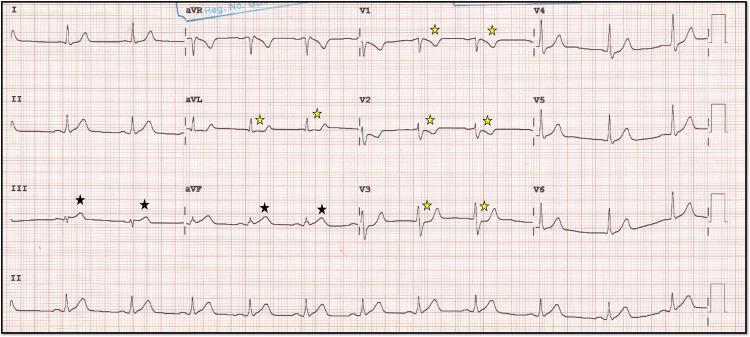
Inferior STEMI (RCA territory)
ST elevation in II, III, aVF (black ★) with reciprocal ST depression in aVL and V1–V3 (yellow ★):
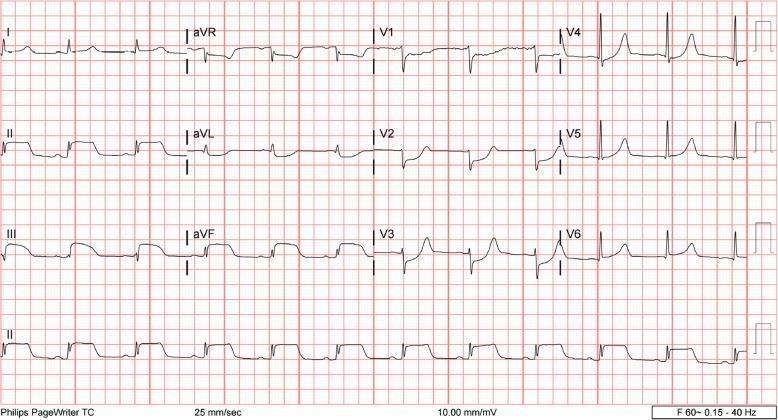
Inferior-Posterior STEMI
ST elevation II/III/aVF + ST depression V1–V4 (posterior involvement) + lateral V5–V6 changes:
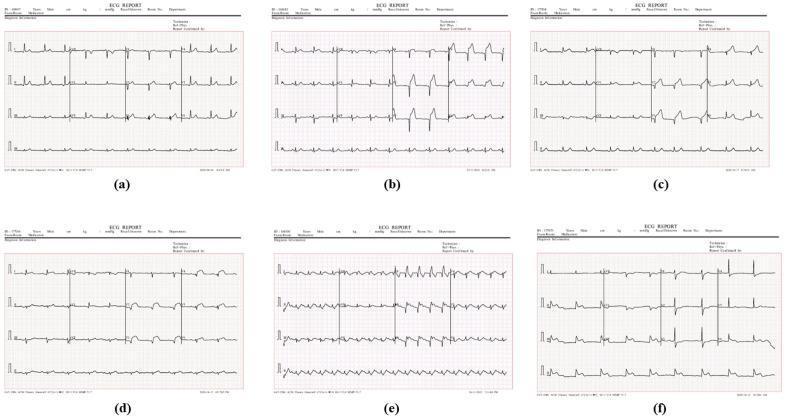
Multiple MI Territory Comparison
(a) Normal, (b) Anterior, (c) Anterolateral, (d) Anteroseptal, (e) Extensive anterior, (f) Inferior MI:
Step 5 — Special Patterns (Don't Miss These)
🔴 Left Main / Proximal LAD
- ST elevation in aVR (≥0.5 mV) — ~78% sensitive, 83% specific for left main disease
- If elevation greater in aVR than V1 → left main; greater in V1 → proximal LAD
🔴 de Winter Pattern (LAD equivalent)
- J-point depression + upsloping ST depression + tall T waves in V1–V6
- ST elevation in aVR
- Treat as STEMI equivalent
🔴 Wellens Syndrome (Critical LAD stenosis warning)
- Type A: Biphasic T waves V2–V3 (25% of cases)
- Type B: Deep symmetric T inversions V2–V3 (75% of cases)
- Seen when pain-free — heralds impending anterior STEMI if untreated
🔴 Posterior MI
- No direct posterior leads on standard ECG
- Clue: ST depression + tall R wave + upright T in V1–V3 (mirror image of posterior STEMI)
- Confirm with posterior leads (V7–V9) showing ST elevation
Step 6 — Differential for ST Elevation (Not All STE = STEMI)
| Condition | Distinguishing Feature |
|---|---|
| Acute pericarditis | Diffuse STE in almost all leads (except aVR), concave morphology, PR depression |
| Early repolarization | Concave STE, notching at J point, young healthy patient |
| LVH / LBBB | Discordant ST changes (opposite to QRS direction) |
| Takotsubo | Anterior STE, no culprit artery on angiogram, usually post-stress in older women |
| Hyperkalemia | Peaked T waves + wide QRS, no regional pattern |
| Brugada | V1–V2 STE with coved morphology |
Quick Memory Trick for Lead Territories
INFERIOR = II, III, aVF (think: F for Floor = bottom of heart)
ANTERIOR = V1–V4 (think: chest leads = front wall)
LATERAL = I, aVL, V5–V6 (think: Left side)
POSTERIOR = depression V1–V3 (reciprocal of the back wall)
Sources: Rosen's Emergency Medicine, 9e | Harrison's Principles of Internal Medicine, 22e (2025)
This is a shared conversation. Sign in to Orris to start your own chat.