Classification of the beta blockers
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Explain beta blockers according to 10 Mark
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from Lippincott's and Katzung's pharmacology textbooks. Here is a complete 10-mark answer on beta blockers:
Beta-Adrenergic Blockers (Beta Blockers)
1. Introduction
Beta blockers are drugs that competitively antagonize the effects of catecholamines (epinephrine, norepinephrine) at beta-adrenergic receptors. They were introduced by Sir James Black in the 1960s, and propranolol remains the prototype of this class. Most members end in "-olol" (except labetalol and carvedilol).
2. Classification
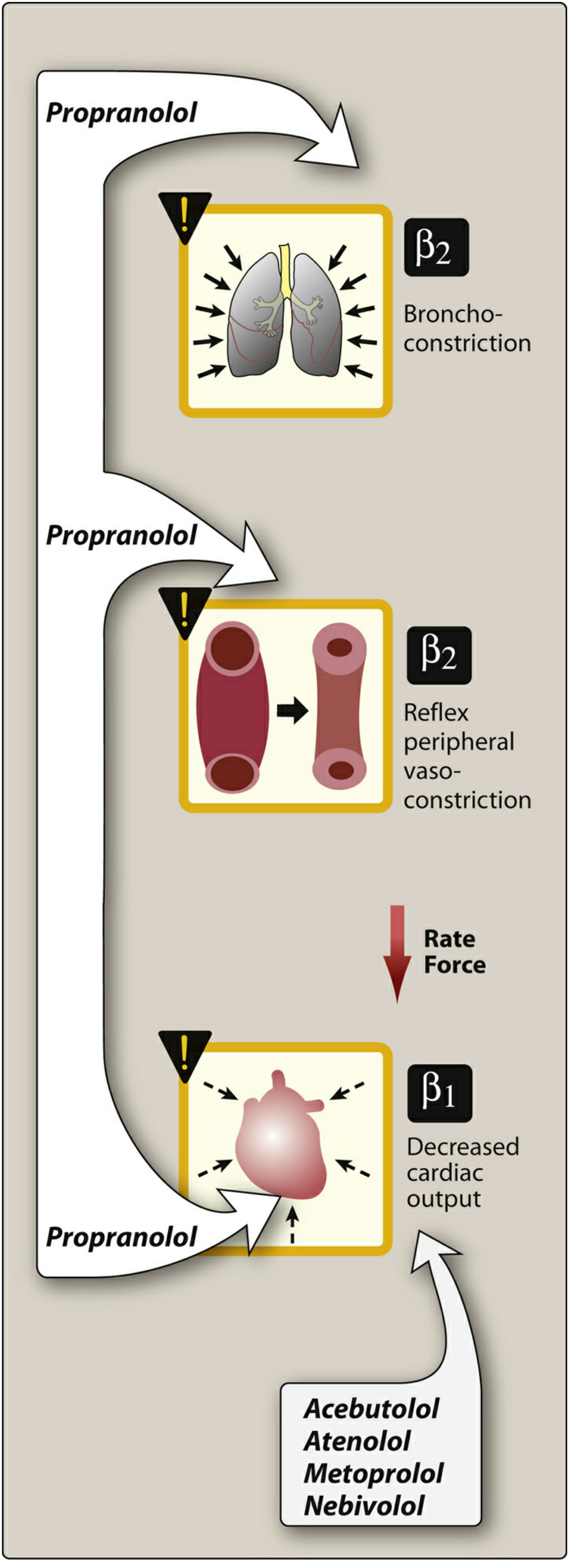
A. Based on Receptor Selectivity
| Generation | Type | Examples |
|---|---|---|
| 1st | Non-selective (β1 + β2 block) | Propranolol, Nadolol, Timolol, Sotalol |
| 2nd | Cardioselective (β1 only) | Metoprolol, Atenolol, Bisoprolol, Acebutolol, Esmolol |
| 3rd | Non-selective + α1 block (vasodilating) | Carvedilol, Labetalol |
| 3rd | β1-selective + vasodilating (via NO) | Nebivolol |
Note: Cardioselectivity is relative and is lost at higher doses - all beta blockers become non-selective at high doses.
B. Based on Intrinsic Sympathomimetic Activity (ISA)
- With ISA (partial agonists): Pindolol, Acebutolol, Penbutolol, Carteolol
- Without ISA: Propranolol, Metoprolol, Atenolol, Bisoprolol, Nadolol
C. Based on Lipid Solubility
- Lipophilic (cross BBB, hepatic metabolism, CNS effects): Propranolol, Metoprolol, Carvedilol
- Hydrophilic (renal excretion, fewer CNS effects): Atenolol, Nadolol
- Intermediate: Bisoprolol, Acebutolol
D. Based on Additional Actions
- Membrane stabilizing (local anesthetic) activity: Propranolol, Acebutolol
- Ultra-short acting (IV only): Esmolol (t½ = 9-10 min, metabolized by RBC esterases)
3. Mechanism of Action
Beta blockers competitively block beta-adrenoceptors:
- β1 blockade (cardiac): Decreased heart rate (negative chronotropy), decreased force of contraction (negative inotropy), decreased cardiac output, slowed AV conduction, reduced renin release from kidneys
- β2 blockade (extra-cardiac): Bronchoconstriction, peripheral vasoconstriction, inhibition of glycogenolysis, decreased lipolysis
4. Pharmacological Actions
| System | Effect |
|---|---|
| Heart | ↓ heart rate, ↓ contractility, ↓ cardiac output, ↓ automaticity, slows AV conduction |
| Blood Pressure | Lowers BP via ↓ CO + ↓ renin + long-term ↓ peripheral resistance |
| Bronchi | Bronchoconstriction (via β2 block - dangerous in asthma) |
| Peripheral vessels | Vasoconstriction (initial), ↓ blood flow to periphery |
| Metabolic | ↓ glycogenolysis, ↓ glucagon secretion, ↑ triglycerides, ↓ HDL |
| Eye | ↓ aqueous humor production → ↓ intraocular pressure |
| Renin | ↓ renin secretion from juxtaglomerular cells |
| CNS | ↓ sympathetic outflow (lipophilic agents: propranolol) |
5. Therapeutic Uses
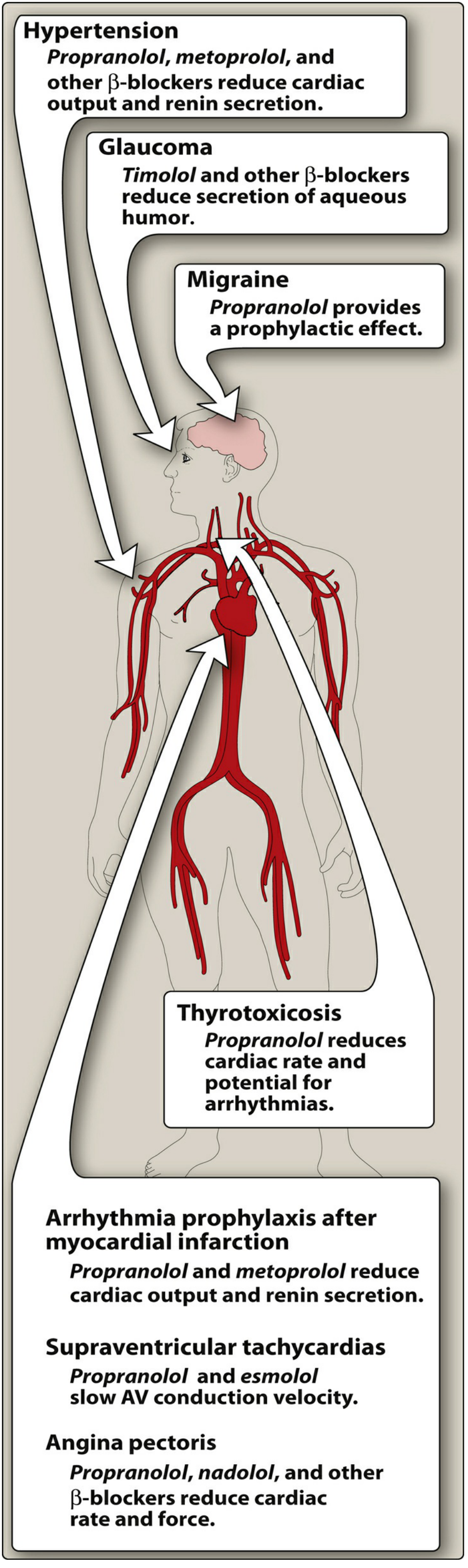
- Hypertension - First-line; metoprolol and atenolol most widely used
- Angina pectoris - Reduce myocardial O2 demand by lowering HR and contractility; first-line therapy for stable angina; avoid in vasospastic angina
- Myocardial infarction - Reduce infarct size, prevent reinfarction, reduce arrhythmic death (propranolol, metoprolol)
- Heart failure - Carvedilol, metoprolol (sustained-release), bisoprolol reduce mortality in HFrEF
- Arrhythmias - Supraventricular tachycardias (AF, flutter); esmolol for acute rate control
- Hypertensive emergencies - IV labetalol (combined α + β block); IV esmolol
- Migraine prophylaxis - Propranolol (lipophilic, penetrates CNS)
- Hyperthyroidism / Thyroid storm - Propranolol controls tachycardia and also inhibits peripheral T4→T3 conversion
- Glaucoma - Timolol, betaxolol (topical); reduce aqueous humor secretion
- Anxiety / Tremors - Propranolol reduces somatic symptoms (palpitations, tremor)
- Pheochromocytoma - Labetalol (always give alpha blocker first, then beta blocker)
- Portal hypertension - Propranolol reduces portal pressure
6. Pharmacokinetics - Key Differences
| Drug | Selectivity | Half-life | Route of Elimination | Special Feature |
|---|---|---|---|---|
| Propranolol | Non-selective | 4-6 h | Hepatic (CYP1A2/2D6) | High first-pass, lipophilic, prototype |
| Metoprolol | β1-selective | 4-6 h | Hepatic (CYP2D6) | SR form for HF |
| Atenolol | β1-selective | 6 h | Renal | Hydrophilic, fewer CNS effects |
| Bisoprolol | β1-selective | 10-12 h | Hepatic + renal | Once daily |
| Esmolol | β1-selective | 9-10 min | RBC esterases | IV only, ultra-short acting |
| Nadolol | Non-selective | Long (14-24 h) | Renal | Not metabolized |
| Carvedilol | Non-selective + α1 | 7-10 h | Hepatic | Also blocks α1, antioxidant |
| Nebivolol | β1-selective | 10-12 h | Hepatic | Vasodilates via NO release |
| Labetalol | Non-selective + α1 | ~6 h | Hepatic | β:α ratio = 3:1 oral, 7:1 IV |
7. Adverse Effects
- Bronchoconstriction - β2 blockade; contraindicated in asthma (non-selective > selective)
- Bradycardia and heart block - Excessive β1 blockade
- Cold extremities - Peripheral vasoconstriction (β2 blockade)
- Metabolic effects - Masking of hypoglycemia symptoms (dangerous in diabetics on insulin), ↑ triglycerides, ↓ HDL
- CNS effects (lipophilic agents) - Depression, nightmares, fatigue, hallucinations, vivid dreams
- Rebound phenomenon - Abrupt withdrawal causes rebound angina, hypertension, MI; must taper over 2-3 weeks (due to β-receptor upregulation)
- Sexual dysfunction - Impotence
- Worsening heart failure - With acute decompensation (but used cautiously in stable HFrEF)
8. Contraindications
| Absolute | Relative |
|---|---|
| Bronchial asthma (non-selective) | COPD |
| Severe bradycardia / heart block | Diabetes mellitus |
| Cardiogenic shock | Peripheral vascular disease |
| Acute decompensated heart failure | Depression |
| Pheochromocytoma (without prior α blockade) | Pregnancy (non-selective → neonatal hypoglycemia, bradycardia) |
9. ISA (Intrinsic Sympathomimetic Activity) - Special Note
Drugs like pindolol, acebutolol, and penbutolol are partial agonists. They partially stimulate the beta receptor while blocking stronger endogenous catecholamines. Key points:
- Cause less bradycardia at rest - useful in patients with moderate bradycardia
- Minimize metabolic disturbances (do not lower HDL)
- Should NOT be used in post-MI patients or angina (partial agonism is harmful)
- Rarely used in clinical practice today
10. Drug Interactions
- Verapamil / Diltiazem + beta blockers = severe bradycardia and heart block
- CYP1A2/2D6 inhibitors (fluoxetine, paroxetine, bupropion, ritonavir) = elevated propranolol levels
- Tobacco smoking (CYP inducer) = reduced propranolol effect
- NSAIDs = reduce antihypertensive effect
- Insulin/Oral hypoglycemics = hypoglycemia unawareness (masking of tachycardia)
- Clonidine withdrawal + beta blockers = severe rebound hypertension
Sources: Lippincott Illustrated Reviews: Pharmacology, 7th Ed. | Katzung's Basic and Clinical Pharmacology, 16th Ed. | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.