How to identity pneumonia in chest X ray
Reading File
Finding Sources
Searching the Web
pneumonia chest X-ray radiographic findings identification signs
Finding Sources
Loading Image
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have extensive textbook content and several real radiograph images. Here is the comprehensive answer:
Identifying Pneumonia on Chest X-Ray
Chest radiography is the standard first imaging examination for suspected pneumonia. The American Thoracic Society / Infectious Diseases Society of America (IDSA) guidelines recommend radiographic confirmation before treatment, because clinical signs alone are insufficiently accurate. Here is a systematic approach.
1. Standard Views
Obtain posteroanterior (PA) and lateral views. The lateral view helps localize which lobe is involved (critical for middle lobe and lower lobe disease, which can be obscured by the heart or diaphragm on the frontal view).
2. Core Radiographic Signs
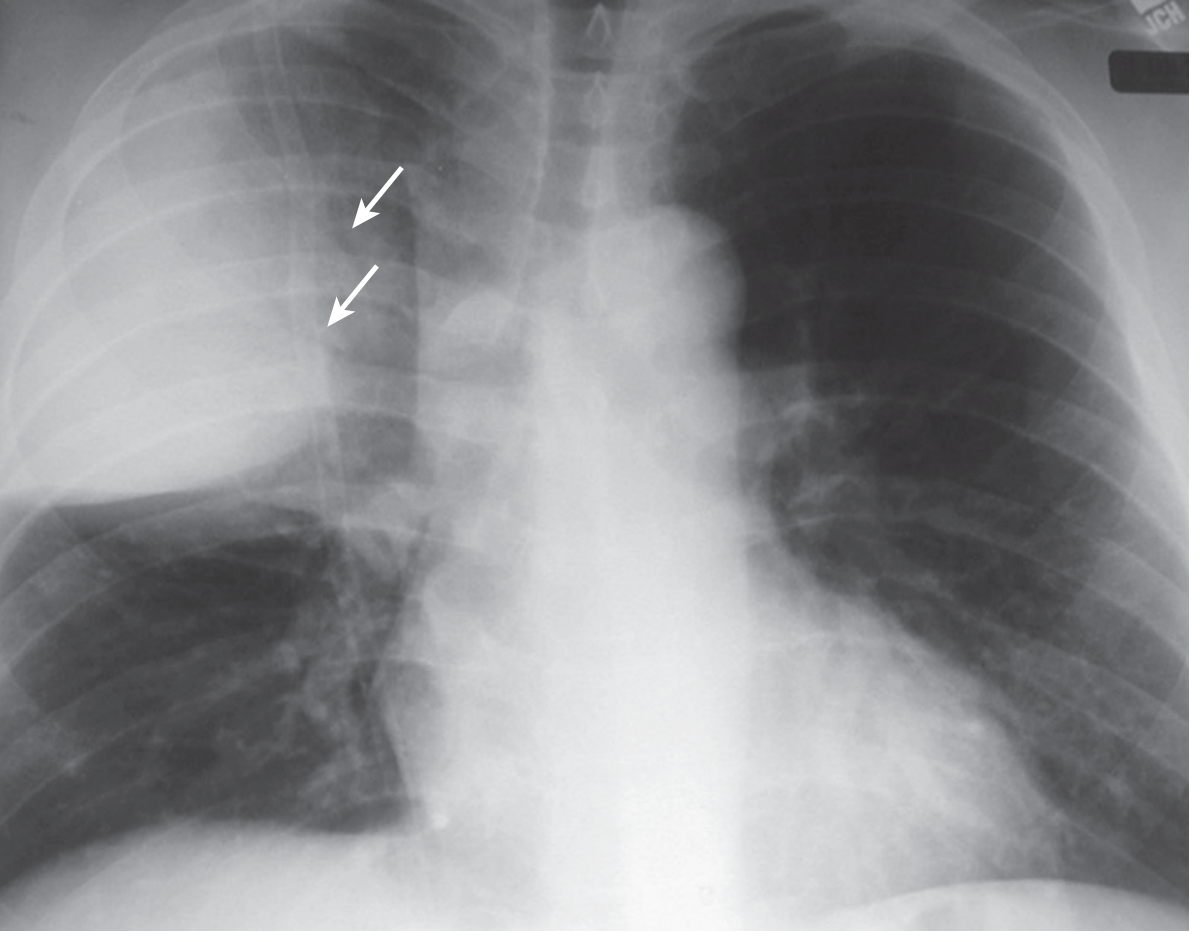
Consolidation / Opacity
The most important finding. When alveoli fill with inflammatory exudate, pus, or fluid, the normally dark (air-filled) lung becomes white/opaque.
- Looks like a white or grey patch against the dark lung
- Can be homogeneous (fills a whole lobe) or patchy
- Borders: sharp where bounded by a fissure, blurred where it abuts other aerated lung
Air Bronchogram
- Bronchi become visible as dark branching tubes within the white opacity because the surrounding alveoli are consolidated but the airways remain air-filled
- Highly specific for airspace (alveolar) consolidation
- Classic in lobar bacterial pneumonia (e.g., pneumococcal)
Silhouette Sign
When a consolidation is adjacent to the heart border or diaphragm, it erases ("silhouettes") that border. For example:
- Right middle lobe pneumonia obliterates the right heart border
- Right lower lobe pneumonia obliterates the right hemidiaphragm
- Lingular (left lower lobe equivalent) pneumonia obliterates the left heart border

3. Radiographic Patterns and Their Significance
Based on Fishman's Pulmonary Diseases and Disorders and Grainger & Allison's Diagnostic Radiology, there are five main patterns:
Pattern 1: Lobar Consolidation
- Dense, homogeneous opacification conforming to a lobe (bounded by fissures)
- Air bronchograms typically present
- Minimal volume loss
- Typical organisms: Streptococcus pneumoniae (most common), Klebsiella pneumoniae
- Klebsiella classically causes right upper lobe disease with bulging of the fissure (expansile consolidation) due to its mucoid nature
Pattern 2: Bronchopneumonia
- Patchy, multifocal, segmental areas of consolidation - not confined to a single lobe
- Follows bronchi and bronchioles
- May be bilateral or unilateral
- Confluent patches can look like lobar consolidation
- Typical organisms: Staphylococcus aureus, Haemophilus influenzae, gram-negative bacilli, Mycoplasma, Chlamydophila, viral infections
Pattern 3: Interstitial Pneumonia
- Reticular or reticulonodular pattern - a fine mesh-like or lace-like thickening
- Peribronchial thickening and perihilar predominance
- No frank consolidation (or consolidation develops later)
- Typical organisms: Viruses (influenza, RSV, adenovirus), Mycoplasma pneumoniae, Chlamydia
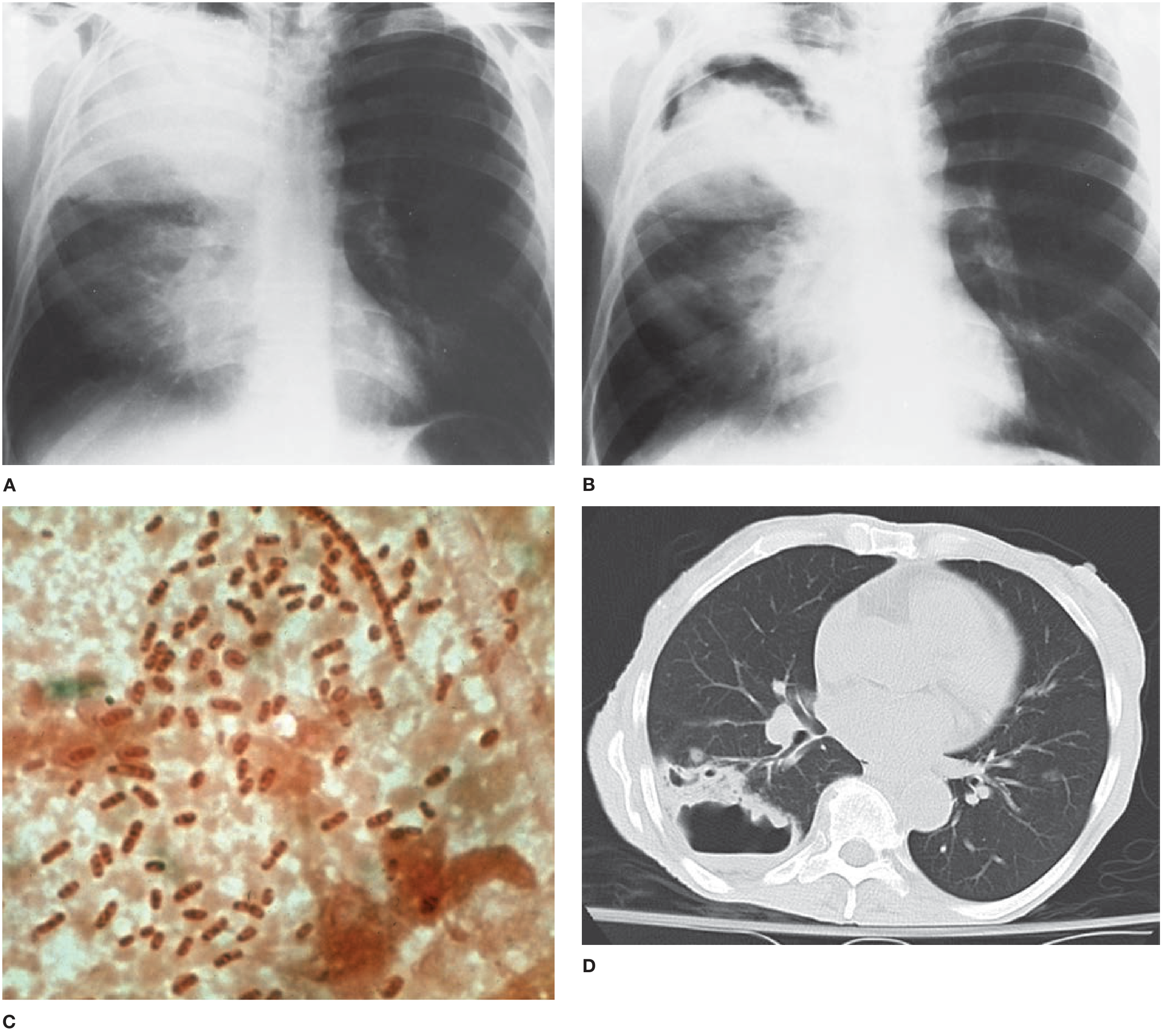
Pattern 4: Cavitation / Nodular Lesions
- Cavity = opacity with a lucent (dark) center, often with an air-fluid level
- Implies necrotic/destructive infection
- Typical organisms: Staphylococcus aureus (also forms pneumatoceles - thin-walled cysts), Klebsiella, anaerobes, gram-negative bacilli, Mycobacterium tuberculosis, endemic fungi
Pattern 5: Miliary / Micronodular
- Diffuse tiny nodules (1-3 mm) spread throughout both lungs, like millet seeds
- Typical organisms: Mycobacterium tuberculosis, endemic fungi, some viruses
| Radiographic Finding | Most Likely Organisms |
|---|---|
| Lobar consolidation | S. pneumoniae, K. pneumoniae |
| Bronchopneumonia (patchy) | S. aureus, gram-negative bacilli, anaerobes |
| Interstitial infiltrates | Viruses, M. pneumoniae |
| Cavity formation | TB, S. aureus, gram-negative bacilli |
| Miliary nodules | TB, endemic fungi |
| Round pneumonia | S. pneumoniae (especially children) |
(Grainger & Allison's Diagnostic Radiology, Box 5.1; Fishman's Pulmonary Diseases, Table 122-7)
4. Associated Findings to Look For
| Finding | Significance |
|---|---|
| Pleural effusion | Parapneumonic effusion; large effusion suggests bacterial cause; empyema if loculated |
| Volume loss / atelectasis | Mucus plugging of bronchi; look for shift of fissures |
| Hilar lymphadenopathy | TB, viral infections, endemic fungi |
| Pneumothorax | Rare complication, especially with S. aureus |
| Bilateral/diffuse opacity | Viral pneumonitis, Pneumocystis jirovecii (PJP), severe sepsis |
5. Where to Look (Anatomy Tips)
- Lower lobes are most commonly affected (gravity-dependent)
- Right middle lobe: best seen on lateral view; obliterates right heart border on PA
- Upper lobes: consider TB (especially apical/posterior segments), or Klebsiella in alcoholics
- Dependent segments (posterior upper lobes, superior lower lobes): suspect aspiration pneumonia
6. Important Limitations
- False negatives can occur in: early infection, neutropenia, severe dehydration, Pneumocystis pneumonia
- Chest radiograph can appear normal in 5-10% of proven pneumonias (early disease)
- Radiographic patterns overlap - you cannot reliably identify the causative organism from the X-ray pattern alone
- HRCT is more sensitive (can detect pneumonia up to 5 days earlier than plain film) and is indicated when clinical suspicion is high but X-ray is negative or non-specific
7. Differential Diagnosis (Things That Mimic Pneumonia)
- Pulmonary edema (bilateral perihilar "bat-wing" opacity)
- Pulmonary infarct (Hampton's hump - pleural-based wedge opacity)
- Lung cancer with post-obstructive collapse
- Organizing pneumonia / cryptogenic organizing pneumonia (COP)
- Aspiration of foreign material
- Hemorrhage or contusion
Key takeaway: Look for a new opacity (white area) in the lungs - it may be lobar, patchy, or interstitial. Air bronchograms within it strongly suggest airspace consolidation. Check borders for the silhouette sign. Then integrate with clinical context (fever, cough, productive sputum) for the diagnosis. No single radiographic pattern is pathognomonic for a specific organism.
Sources: Fishman's Pulmonary Diseases and Disorders (2-Volume Set), Chapter 122; Murray & Nadel's Textbook of Respiratory Medicine; Grainger & Allison's Diagnostic Radiology, Chapter 5
This is a shared conversation. Sign in to Orris to start your own chat.