i want to learn ophthalmology from Kanski. how many days are required to finish and retain the information?
Kanski Clinical Ophthalmology 8th edition page count chapters overview
Kanski Clinical Ophthalmology 10th edition 2023 page count chapters table of contents
table of contents chapters page count
Kanski's Clinical Ophthalmology - How Long to Finish and Retain It
The Book at a Glance
| # | Chapter | Pages (approx.) |
|---|---|---|
| 1 | Examination Techniques | 36 |
| 2 | Eyelids | 60 |
| 3 | Lacrimal Drainage System | 16 |
| 4 | Orbit | 44 |
| 5 | Dry Eye | 12 |
| 6 | Conjunctiva | 36 |
| 7 | Cornea | 70 |
| 8 | Corneal and Refractive Surgery | 16 |
| 9 | Episclera and Sclera | 16 |
| 10 | Lens | 38 |
| 11 | Glaucoma | 84 |
| 12 | Uveitis | 76 |
| 13 | Retinal Vascular Disease | 60 |
| 14 | Acquired Macular Disorders | 62 |
| 15 | Inherited Retinal Degenerations | 38 |
| 16 | Retinal Detachment | 36 |
| 17 | Vitreous Opacities | 6 |
| 18 | Strabismus | 50 |
| 19 | Neuro-ophthalmology | 86 |
| 20 | Ocular Tumours | 54 |
| 21 | Ophthalmic Side Effects of Systemic Medication | 10 |
| 22 | Trauma | 26 |
| Total (text) | ~932 pages |
Time Estimates - By Study Goal
| Study Mode | Pages/Day | Days to Read | Retention Method | Total Days |
|---|---|---|---|---|
| Passive read-through | 40-50 pp | ~20 days | None structured | ~20 days |
| Active reading (notes + highlights) | 25-30 pp | ~35 days | Light review | ~40 days |
| Learn + retain (active recall, spaced repetition) | 15-20 pp | ~55 days | Anki/flashcards + weekly reviews | ~70-90 days |
| Exam-level mastery (ophthalmology boards/FRCS) | 10-15 pp | 70+ days | Multi-pass + MCQ practice | 3-6 months |
Realistic Schedule (3-Month Plan, Recommended)
- Weeks 1-2: Ch. 1-4 (Examination, Eyelids, Lacrimal, Orbit)
- Weeks 3-4: Ch. 5-10 (Dry Eye, Conjunctiva, Cornea, Lens)
- Weeks 1-2: Ch. 11-12 (Glaucoma, Uveitis - these are the two densest chapters)
- Weeks 3-4: Ch. 13-17 (Retinal vascular, Macula, Inherited, Detachment)
- Week 1-2: Ch. 18-22 (Strabismus, Neuro-ophthalmology, Tumours, Trauma)
- Weeks 3-4: Full revision pass, Anki deck review, MCQ practice
Key Tips for Retention
-
Study images first. Kanski is built around clinical photographs - before reading a section, look at all the images in it. Your brain encodes the pattern visually, then the text fills in the mechanism.
-
Prioritize the heavy chapters. Glaucoma (Ch. 11), Uveitis (Ch. 12), Neuro-ophthalmology (Ch. 19), and Retinal Vascular Disease (Ch. 13) together make up ~35% of the book. Budget extra time here.
-
Use spaced repetition. After finishing each chapter, create 20-30 Anki cards (key findings, eponyms, management stepladders). Review the deck daily for 10 minutes. This alone roughly doubles long-term retention compared to re-reading.
-
Don't re-read passively. After your first pass, testing yourself (covering text, recalling findings from images) is far more effective than reading again.
-
Pair with clinical exposure. Seeing real patients or case photos while reading the corresponding chapter locks in memory far faster than text alone.
Bottom Line
| Goal | Minimum Time |
|---|---|
| Read it cover to cover (casual) | 3-4 weeks |
| Understand and remember the main concepts | 8-10 weeks |
| Exam-ready retention (FRCS / fellowship level) | 3-5 months |
now i have my posting in cornea department, I want to start from cornea. help me study
Kanski Cornea Chapter - Complete Study Guide
Complete Topic Map (Chapter 7)
Section A - Foundations (Study First)
- Anatomy and Physiology - dimensions, 5-layer structure (epithelium, Bowman, stroma, Descemet, endothelium)
- Signs of Corneal Disease
- Superficial signs (epithelial staining patterns, filaments, pannus)
- Deep signs (KPs, stromal edema, neovascularization, scarring)
- Documentation (slit-lamp grading)
- Specular Microscopy - endothelial cell count, polymegethism, pleomorphism
- Corneal Topography - Placido disc, elevation maps
- Principles of Treatment - infection control, promoting epithelial healing
Section B - Infections (Core Clinical)
- Bacterial Keratitis - pathogens, risk factors, ulcer morphology, Gram stain, fortified antibiotics, treatment failure
- Fungal Keratitis - filamentous vs. Candida, feathery infiltrate, natamycin/voriconazole
- Herpes Simplex Keratitis (HSK) - primary vs. recurrent, 5 types:
- Epithelial (dendritic/geographic) - treat with antivirals
- Disciform keratitis - stromal immune reaction
- Necrotizing stromal keratitis
- Neurotrophic keratopathy
- Iridocyclitis; prophylaxis with long-term acyclovir
- Herpes Zoster Ophthalmicus - Hutchinson's sign, acute vs. chronic eye disease, post-herpetic neuralgia
- Interstitial Keratitis - syphilitic IK (salmon patch, ghost vessels), Cogan syndrome
- Protozoan Keratitis (Acanthamoeba) - contact lens risk, ring infiltrate, PHMB/polyhexamethylene biguanide
- Helminthic Keratitis - onchocerciasis (river blindness)
- Microsporidial Keratitis
Section C - Inflammatory & Immune
- Bacterial Hypersensitivity Keratitis
- Marginal keratitis - peripheral ulcer, clear zone from limbus
- Phlyctenulosis - nodular limbal/corneal lesion
- Rosacea Keratitis - inferior corneal vascularization, meibomian gland dysfunction link
- Peripheral Corneal Ulceration/Thinning
- Mooren ulcer - idiopathic, painful, central guttering
- Peripheral ulcerative keratitis (PUK) - associated with systemic vasculitis (RA, Wegener's)
Section D - Ectasias
- Keratoconus - scissors reflex, Munson sign, Fleischer ring, Vogt striae, Rizzuti sign; corneal cross-linking (CXL)
- Pellucid Marginal Degeneration
- Keratoglobus
- Post-LASIK ectasia
Section E - Dystrophies (genetically determined, bilateral, symmetric)
- Epithelial and Subepithelial:
- Meesmann dystrophy
- Epithelial basement membrane dystrophy (EBMD / map-dot-fingerprint)
- Reis-Bucklers dystrophy
- Stromal:
- Granular dystrophy (breadcrumb opacities, Masson trichrome stain)
- Lattice dystrophy (branching refractile lines, amyloid, Congo red)
- Macular dystrophy (diffuse clouding, alcian blue, keratan sulfate)
- Schnyder crystalline dystrophy
- Endothelial:
- Fuchs endothelial dystrophy (cornea guttata, Hassal-Henle bodies)
- Posterior polymorphous dystrophy (PPMD)
- Congenital hereditary endothelial dystrophy (CHED)
Section F - Degenerations
- Arcus senilis
- Pterygium - fibrovascular ingrowth, Stocker line
- Calcific band keratopathy
- Terrien marginal degeneration
- Recurrent corneal epithelial erosion
Section G - Metabolic & Miscellaneous
- Metabolic keratopathies - Wilson disease (Kayser-Fleischer ring), cystinosis, tyrosinemia
- Neurotrophic keratopathy - trigeminal nerve damage, Mackie staging
- Contact lens-related disease - GPC, CLPU, CLARE, pseudomonas risk
- Congenital anomalies - microcornea, megalocornea, Peters anomaly, sclerocornea
Study Schedule (2-Week Focused Posting Plan)
| Day | Topic | Clinical Correlation |
|---|---|---|
| Day 1 | Anatomy + Signs of corneal disease + Specular microscopy | Slit-lamp examination basics |
| Day 2 | Bacterial keratitis (full section) | Corneal scraping, culture, fortified drops |
| Day 3 | Fungal keratitis + Acanthamoeba | Identify feathery/ring infiltrate on slit-lamp |
| Day 4 | Herpes simplex keratitis (all subtypes) | Dendritic ulcer identification with fluorescein |
| Day 5 | Herpes zoster ophthalmicus | Hutchinson's sign, dermatome distribution |
| Day 6 | Interstitial keratitis + Marginal/Phlyctenular | Systemic workup (VDRL, FTA-ABS) |
| Day 7 | Rosacea + Peripheral ulceration + Mooren + PUK | Systemic vasculitis link, RA screen |
| Day 8 | Corneal ectasias (Keratoconus focus) | Topography maps, cross-linking patients |
| Day 9 | Epithelial + Stromal dystrophies | Recognize on slit-lamp (breadcrumb, lattice lines) |
| Day 10 | Endothelial dystrophies (Fuchs esp.) | Specular microscopy, DSAEK/DMEK planning |
| Day 11 | Degenerations (Pterygium, band keratopathy, EBMD) | Pre-op pterygium cases |
| Day 12 | Neurotrophic keratopathy + Contact lens disease | Corneal sensation testing, aesthesiometry |
| Day 13 | Metabolic keratopathies + Congenital anomalies | KF ring search in young patients |
| Day 14 | Full revision - self-test with slit-lamp images | Attend OPD, apply everything |
High-Yield Facts to Memorize First
- Dendritic ulcer = HSV epithelial keratitis. Terminal bulbs. Treat: acyclovir 3% ointment 5x/day. Never give steroids alone.
- Ring infiltrate = Acanthamoeba until proven otherwise. Contact lens + water exposure history.
- Feathery edges + satellite lesions = Fungal keratitis. Post-trauma with vegetable matter.
- Clear zone between ulcer and limbus = Marginal keratitis (staph hypersensitivity). Steroids + antibiotics.
- No clear zone + melting = Mooren or PUK - check ANA, ANCA, RF.
- Munson sign + scissors reflex = Keratoconus. Fleischer ring (iron) + Vogt striae.
- Cornea guttata + corneal edema = Fuchs dystrophy. Worse in morning.
- KF ring = Wilson disease (copper). Slit-lamp: golden-brown at Descemet periphery.
- Hutchinson's sign (tip of nose involved) = 76% risk of ocular involvement in HZO.
- Breadcrumbs = Granular (TGFBI, AD), branching lines = Lattice (amyloid), diffuse haze = Macular (AR, worst vision).
How to Use the Book in the Department
- Before OPD: Skim the images/figures of the day's topic - takes 10 min.
- After OPD: Read the full section for conditions you actually saw that day. Active recall is strongest right after seeing a patient.
- Evening: Make 5-10 Anki cards per session (signs, investigations, treatment steps).
- Weekend: Review the whole week's cards + re-read one section from scratch.
Generate an Anki-style flashcard deck for high-yield corneal findings
Kanski Cornea Flashcards
Presentation · PPTX
What's Inside (1.1 MB, 97 slides)
- Front (navy): category tag + question number + the question
- Back (dark blue): structured answer with a gold PEARL box at the bottom for mnemonics/clinical tips
14 Categories Covered
| Category | Cards |
|---|---|
| Anatomy | 3 |
| Signs | 6 |
| Bacterial Keratitis | 3 |
| Fungal Keratitis | 3 |
| HSV Keratitis | 4 |
| HZO | 3 |
| Acanthamoeba | 2 |
| Interstitial Keratitis | 2 |
| Hypersensitivity (Marginal/Phlyctenular) | 2 |
| Rosacea | 2 |
| Peripheral Ulceration (Mooren/PUK) | 2 |
| Keratoconus | 3 |
| Dystrophies (Granular/Lattice/Macular/Fuchs/EBMD/PPMD) | 4 |
| Degenerations, Metabolic, Neurotrophic, CL disease, Congenital, Keratoplasty, Treatment | 11 |
How to Use
- Open in PowerPoint and go through slide by slide (question → answer)
- Use Presenter View to show only the front card on screen and keep the answer hidden
- You can also print 4 slides/page (2 fronts + 2 backs) as paper flashcards
- Work through 10 cards/day in the morning before OPD - 5 days to complete the full deck
continue
Kanski Cornea - Session 1: Anatomy & Signs of Corneal Disease
PART 1: ANATOMY
The Cornea at a Glance
- Horizontal diameter: 12 mm, Vertical: 11.5 mm
- Central thickness: ~540 µm (range 490-590 µm)
- Peripheral thickness: ~700 µm
- Central corneal thickness (CCT) is a key determinant of IOP readings - thin cornea underestimates IOP on applanation tonometry
The 5 Layers - Deep Dive
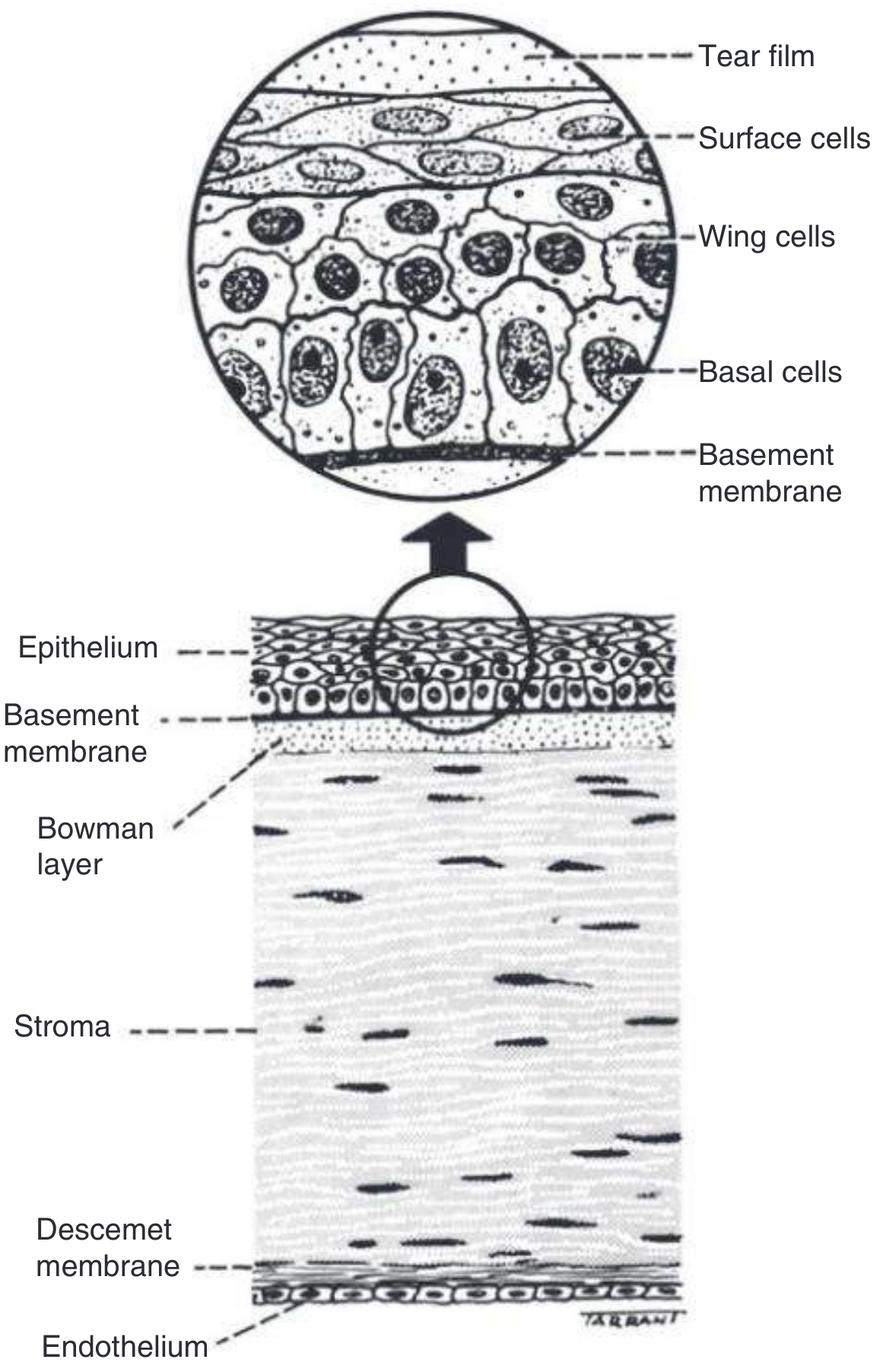
Layer 1: Epithelium
| Cell Type | Location | Function |
|---|---|---|
| Basal columnar cells | Single layer, deepest | Attached to basement membrane by hemidesmosomes - these fail in recurrent erosion syndrome |
| Wing cells | 2-3 layers above basal | Provide structural support |
| Squamous surface cells | Outermost 2 layers | Have microplicae + microvilli that anchor the tear film mucin layer |
- Limbal stem cell deficiency (LSCD) → "conjunctivalization" of the cornea: vascularization + goblet cells appear on corneal surface
- Causes of LSCD: chemical burns, Stevens-Johnson syndrome, aniridia, repeated surgeries
- Treatment: limbal stem cell transplantation (autograft or allograft)
Clinical tip: Superficial cells are shed every few days into the tear film. The entire epithelium turns over every 7-10 days. This is why superficial defects heal quickly but recurrent erosion is about a deeper problem - faulty hemidesmosome anchoring.
Layer 2: Bowman Layer
- Acellular, formed from randomly arranged collagen fibres (unlike the regular lamellae of the stroma)
- 8-12 µm thick
- Does NOT regenerate - any significant injury to Bowman leaves a permanent scar
- This is clinically relevant: PTK (phototherapeutic keratectomy) ablates Bowman deliberately in band keratopathy/EBMD, but the resulting surface heals over with epithelium, not new Bowman
Layer 3: Stroma
- Makes up 90% of corneal thickness (~480 µm)
- Composed of ~200 regular, parallel lamellar sheets of collagen fibrils
- The spacing between fibrils is maintained by proteoglycan ground substance (primarily keratan sulphate and chondroitin sulphate)
- Scattered keratocytes (modified fibroblasts) maintain the extracellular matrix
- The regularity of collagen spacing = optical clarity. Any swelling, scar, or infiltrate disrupts this arrangement
Mechanism of corneal oedema: When stroma swells, the collagen fibril spacing increases beyond the critical ~60 nm needed for destructive interference of scattered light → you see clouding.
Layer 4: Descemet Membrane
- Anterior banded zone - laid down in utero, 3 µm thick
- Posterior non-banded zone - laid down throughout life by the endothelium, thickens with age (reaches ~10 µm in adults)
- Horizontal/oblique = congenital glaucoma (buphthalmos)
- Vertical = birth forceps trauma
Layer 5: Endothelium
| Parameter | Value |
|---|---|
| Young adult density | ~3000 cells/mm² |
| Normal decline | ~0.6% per year |
| Density at which oedema develops | <500 cells/mm² |
A note on Dua's Layer: A 6th layer between the posterior stroma and Descemet has been proposed (15 µm thick, acellular). Its clinical relevance is in DMEK surgery and big-bubble DALK technique. Kanski acknowledges it but notes some authorities consider it posterior stroma.
Innervation - Why Corneal Pain is So Severe
- Subepithelial plexus - just below epithelium, dense
- Deeper stromal plexus
PART 2: SIGNS OF CORNEAL DISEASE
SUPERFICIAL SIGNS
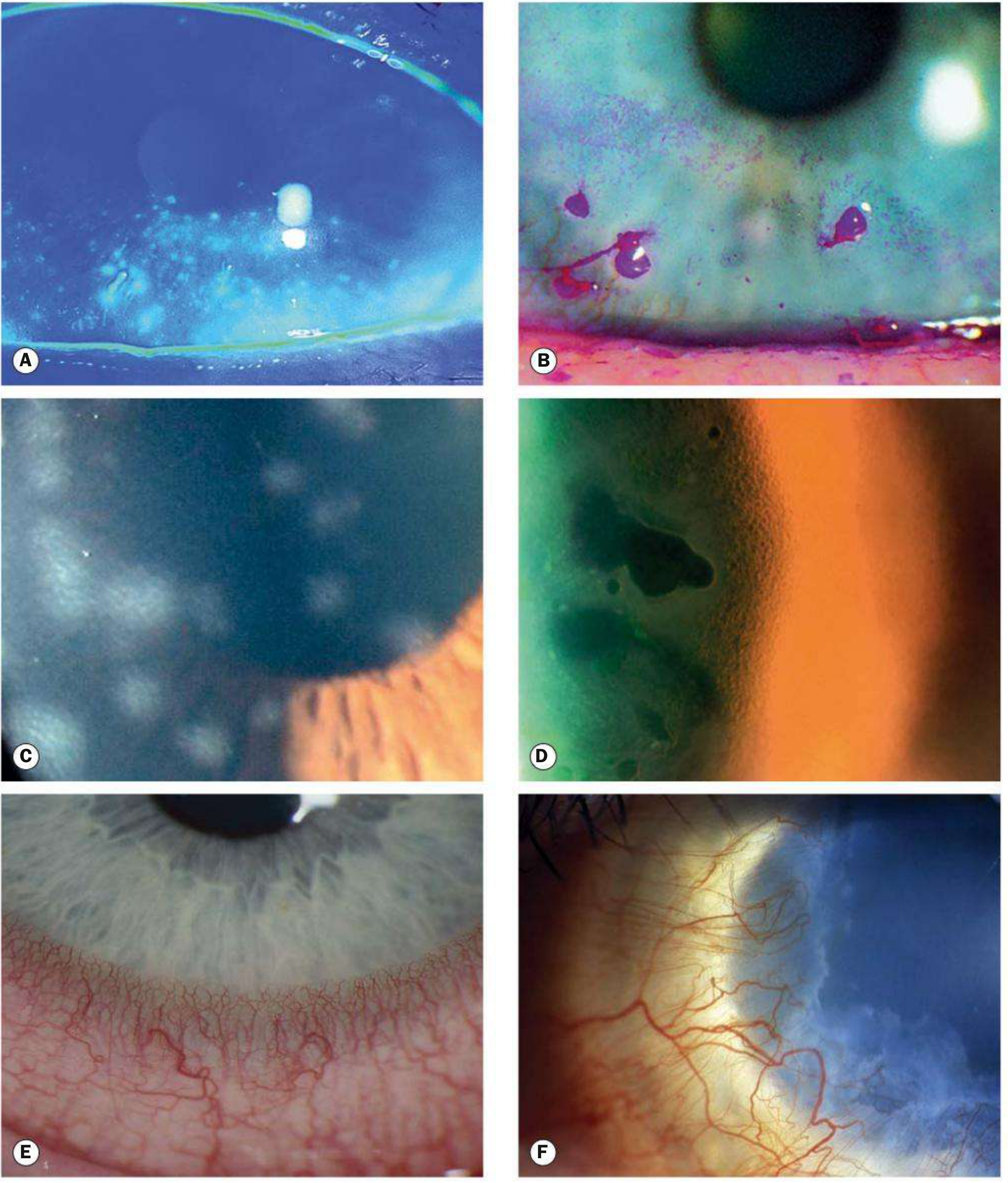
1. Punctate Epithelial Erosions (PEE) - Panel A
| Location | Think of... |
|---|---|
| Superior | Vernal disease, chlamydial conjunctivitis, SLK (superior limbic keratoconjunctivitis), floppy eyelid syndrome |
| Interpalpebral (central band) | Dry eye, UV keratopathy (snow blindness, welding arc), reduced corneal sensation |
| Inferior | Blepharitis, lagophthalmos, toxic drops, trichiasis/entropion |
| Diffuse | Viral conjunctivitis, drop toxicity (especially BAK preservative) |
| Central | Prolonged contact lens wear |
PEE vs PEK: PEE = epithelial defects (stain with fluorescein). PEK (punctate epithelial keratitis) = swollen/opalescent cells (stain better with rose bengal, variably with fluorescein).
2. Filaments - Panel B
- Dry eye (by far the most common)
- Superior limbic keratoconjunctivitis (SLK)
- Neurotrophic keratopathy
- Long-term ocular patching
3. Subepithelial Infiltrates - Panel C
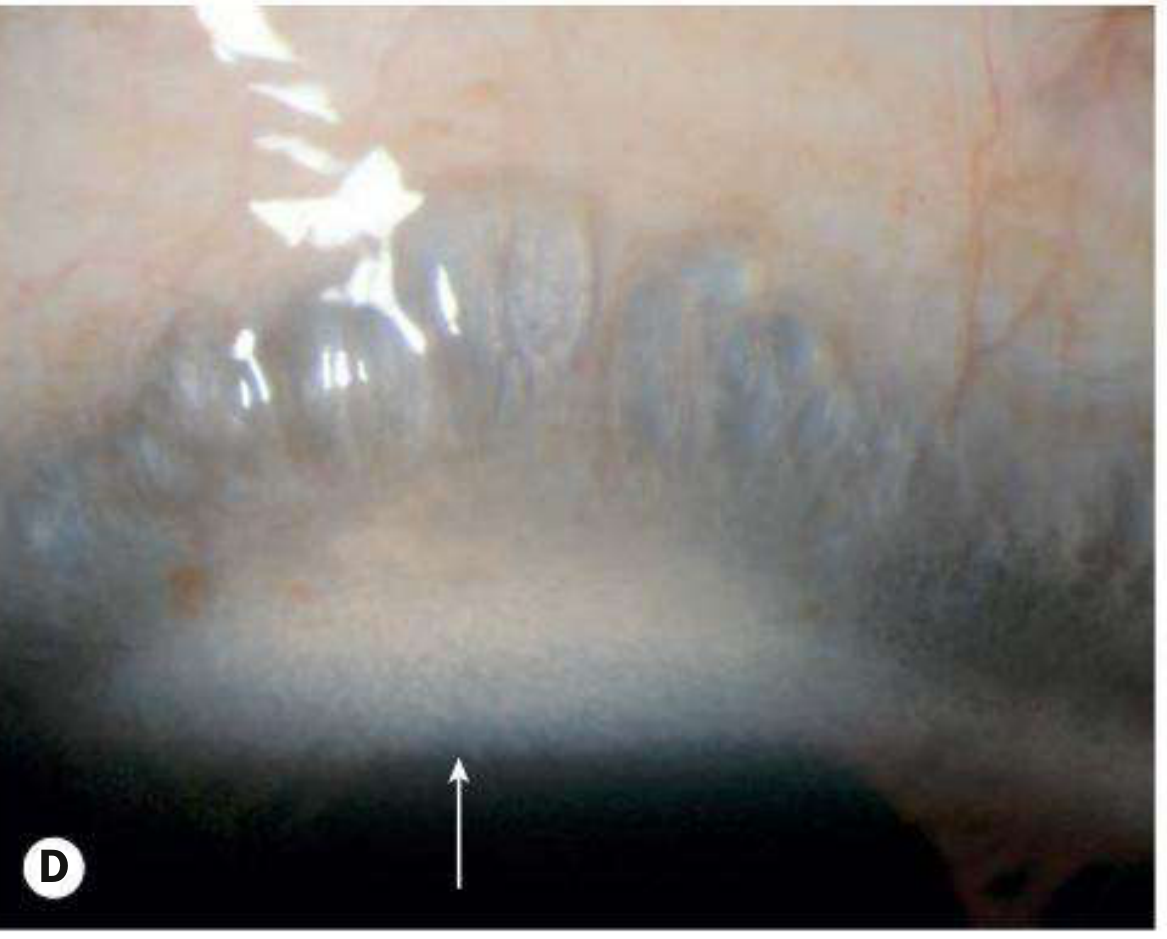
4. Epithelial Oedema + Bullae - Panel D
5. Superficial Neovascularization - Panel E
6. Pannus - Panel F
DEEP SIGNS
The PEDAL Mnemonic - Infective vs. Sterile Infiltrate
| Feature | Infective | Sterile |
|---|---|---|
| Pain | Moderate-severe | Mild |
| Epithelial defect | Very common, large | Less common, small |
| Discharge | Purulent | Mucopurulent |
| AC reaction | Severe | Mild |
| Location | Often central | Typically peripheral |
| Size | Larger | Smaller |
| Number | Usually single | Often multiple |
| Laterality | Unilateral | Often bilateral |
| Progression | Rapid | Slow |
PEDAL = Pain, Epithelial defect, Discharge, Anterior chamber reaction, Location. Use this at every corneal infiltrate you see in OPD.
Other Deep Signs
| Sign | Description | Causes |
|---|---|---|
| Ulceration | Tissue excavation + epithelial defect | Infective keratitis, autoimmune, neurotrophic |
| "Melting" | Tissue disintegration from enzymatic (MMP) activity, minimal infiltrate | PUK, Mooren ulcer - MMPs from activated neutrophils |
| Deep vascularization | Straight vessels entering stroma from limbus | Interstitial keratitis, herpes, chronic disease |
| Ghost vessels | Non-perfused empty vessels visible on retroillumination | Healed interstitial keratitis (syphilis), resolved HZO |
| Lipid deposition | Yellow-white crystalline deposits following new vessel leakage | Post-inflammatory neovascularization |
| Descemet folds (striate keratopathy) | Parallel wrinkled lines on Descemet | Corneal oedema, post-operative, trauma, ocular hypotony |
| Descemetocele | Bubble-like herniation of Descemet into a stromal defect | End-stage corneal thinning (perforating ulcer imminent) |
| Haab striae | Paired curved breaks in Descemet | Congenital glaucoma (horizontal), birth trauma (vertical) |
HOW TO DOCUMENT CORNEAL LESIONS
| Colour | What it represents |
|---|---|
| Black | Opacities (scars, degenerations) |
| Blue circles (fine) | Epithelial oedema |
| Blue shading | Stromal oedema |
| Wavy blue lines | Descemet folds |
| Yellow | Hypopyon |
| Red wavy lines from outside limbus | Superficial vessels |
| Red straight lines from limbus | Deep stromal vessels |
| Brown | Pigmented lesions (iron lines, KF ring, Krukenberg spindle) |
THE SEIDEL TEST
- Apply 1-2% fluorescein to the eye
- Use cobalt blue filter on slit-lamp
- Positive: colour changes from dark orange → bright yellow-green at one spot
- Means: aqueous is leaking through a wound or perforation at that site (diluting the concentrated dye)
Summary - What You Now Know
CORNEA = Protection + Optics
5 Layers: Epithelium > Bowman > Stroma > Descemet > Endothelium
Key facts: Bowman & stroma cannot regenerate. Descemet & epithelium can.
Endothelium: pump cells, cannot regenerate, <500/mm² → oedema.
Stem cells: limbus. Lose them → conjunctivalization.
Signs by location:
Superior PEE → vernal/SLK/chlamydia
Inferior PEE → blepharitis/lagophthalmos/toxic drops
Interpalpebral → dry eye
Central → contact lenses
PEDAL = how to tell infective from sterile infiltrate
Seidel test = aqueous leak detection
Document all lesions with size + colour-coded diagram
no. i didn't understand after anatomy
Signs of Corneal Disease - Taught Simply
SUPERFICIAL SIGNS (Epithelium layer)
Panel A - Punctate Epithelial Erosions (PEE)
- Dots at the top (superior) → something is rubbing the upper cornea → vernal disease (giant papillae under upper lid), trachoma, SLK
- Dots in the middle exposed zone (interpalpebral) → the exposed surface is drying out → dry eye, UV damage (welding, snow)
- Dots at the bottom (inferior) → lower lid problem → blepharitis, inward-turning eyelashes (trichiasis), toxic eye drops (BAK preservative)
- Dots scattered everywhere (diffuse) → viral conjunctivitis or toxic drops affecting the whole surface
- Dots only in the centre → contact lens sitting on the cornea centre too long → contact lens wear
Panel B - Filaments
Panel C - Subepithelial Infiltrates
Panel D - Epithelial Oedema and Bullae
Panel E - Superficial Neovascularisation
Panel F - Pannus
DEEP SIGNS (Stroma, Descemet, Endothelium)
Infiltrate (Deep)
- Infective → needs aggressive antibiotics/antivirals immediately
- Sterile → needs steroids (giving antibiotics alone won't help; giving steroids on an infection will make it catastrophically worse)
| Letter | Feature | Infective | Sterile |
|---|---|---|---|
| P | Pain | Severe | Mild |
| E | Epithelial defect | Large, present | Small or absent |
| D | Discharge | Purulent (pus) | Mucopurulent |
| A | Anterior chamber reaction | Severe (hypopyon common) | Mild |
| L | Location | Central | Peripheral |
- Infective = usually one lesion, one eye
- Sterile = often multiple lesions, sometimes both eyes
Ulcer
Melting
Deep Vascularisation
Descemet Folds (Striate Keratopathy)
Descemetocele
Haab Striae
- Horizontal striae → the eyeball was enlarged (buphthalmos from congenital glaucoma) → Descemet was stretched sideways → horizontal breaks
- Vertical striae → forceps pressed on the eye during birth → vertical breaks
THE SEIDEL TEST - a must-know practical skill
- Put a drop of 2% fluorescein on the eye
- Put cobalt blue light on the slit-lamp
- The dye on the surface looks dark orange
- If aqueous is leaking: the leak dilutes the concentrated dye → you see a bright yellow-green stream coming from one spot
QUICK SUMMARY - Signs and Their Meaning
| Sign | Location | What it tells you |
|---|---|---|
| PEE (dots with fluorescein) | Epithelium | Surface is unhappy; location tells you why |
| Filaments (threads) | Epithelium | Dry eye |
| Subepithelial infiltrates (grey clouds, no staining) | Under epithelium | Immune reaction (adenovirus) |
| Bullae (blisters) | Epithelium | Endothelium is failing |
| Superficial vessels (wavy) | Epithelium | Hypoxia / chronic irritation |
| Pannus (vessels + scar) | Epithelium + stroma | Trachoma, contact lens, rosacea |
| Infiltrate (white opacity) | Stroma | Infection or sterile immune reaction - use PEDAL |
| Ulcer (crater + staining) | Stroma | Active tissue loss - treat urgently |
| Melting (rapid thinning, no pus) | Stroma | MMPs - autoimmune or neurotrophic |
| Ghost vessels | Deep stroma | Old healed interstitial keratitis |
| Descemet folds | Descemet | Corneal oedema |
| Descemetocele | Descemet bulging | Near-perforation - emergency |
| Haab striae | Descemet breaks | Congenital glaucoma (horiz.) / birth trauma (vert.) |
| Positive Seidel | Any layer | Eye is perforated - emergency |
ask question
punctate epithelial erosion: chronic blepharitis, lagophthalmos, eye drop toxicity, self induced, ulcerative keratopathy
- Correct name: Punctate Epithelial Erosions (PEE)
- Correct causes: chronic blepharitis, lagophthalmos, eye drop toxicity, self-induced ✓
- "Ulcerative keratopathy" is not in the inferior PEE list - you may be mixing it with something else. The ones you missed are aberrant eyelashes (trichiasis/distichiasis) and entropion (inward-turning lid). Both physically rub the inferior cornea.
- (a) What is this sign called?
- (b) What layer is failing to cause this?
- (c) What is the most likely diagnosis?
bullae, endothelium, Fuchs endothelial dystrophy
superficial punctate keratitis, epithelium, punctate epithelial keratitis, yes, exposure of corneal nerve endings leading to pain and photophobia
- Cycloplegic (cyclopentolate) - to relax ciliary spasm and relieve pain
- Lubricants / preservative-free drops
- Bandage contact lens - reduces pain from blinking over exposed nerve endings
- Oral analgesics - the pain can be severe
- It heals on its own within 24-48 hours because the epithelium regenerates quickly
No infiltrate + no discharge + no AC reaction = sterile = no antibiotics
- Single white-grey opacity, 3×3 mm, central cornea
- Large epithelial defect overlying it
- Thick purulent discharge
- Hypopyon 1.5 mm
- Patient reports severe pain
- One eye only
pain: severe, epithelial defect: large, discharge: thick purulent, anterior chamber reaction: hypopyon, location: centre suggestive of infective, requires antibiotic coverage
| Letter | Your finding | Points to... |
|---|---|---|
| P - Pain | Severe | Infective ✓ |
| E - Epithelial defect | Large | Infective ✓ |
| D - Discharge | Thick purulent | Infective ✓ |
| A - AC reaction | Hypopyon | Infective ✓ |
| L - Location | Central | Infective ✓ |
size of the defect?
Corneal scraping for microbiological investigations - send for Gram stain and culture.
Scrape first, treat second - always, for any significant corneal ulcer.
- Central ulcer >2 mm
- No prior antibiotic use
- Atypical appearance
- Treatment failure after 48-72 hours
- Immunocompromised patient
question
subepithelial infiltrate, they are the WBC that have been collected in the anterior stroma in response to an Antigen. usually doesn't require, lubricating eye drops required but if symptomatic ointment acyclovir is given
- Antibiotics - No ✅ you got this right
- Acyclovir - ❌ Wrong drug. Acyclovir works against Herpes simplex / Herpes zoster. Adenovirus is a completely different virus - acyclovir has no effect on adenovirus. Do not give it here.
- Lubricants ✅ correct for mild symptoms
- Correct treatment for symptomatic subepithelial infiltrates: Topical steroids (e.g. prednisolone 0.5% or fluorometholone) - they suppress the immune reaction and clear the infiltrates. BUT they recur when you taper the steroid, so you have to wean very slowly.
Subepithelial infiltrates after adenovirus = topical steroids, not antivirals, not antibiotics. Acyclovir = HSV/HZV only.
how do we know it is adenoviral conjunctivitis or herpes simplex keratitis if the patient present late? 6. shiedls test, flow of aqueous occurs where green colour mixes with yellow, primary repair
Your question: Adenovirus vs HSV when patient presents late?
| Feature | Adenoviral SEI | HSV stromal keratitis |
|---|---|---|
| History | Acute red eye 2-3 weeks ago, often epidemic (family/colleagues also affected), follicular conjunctivitis | Recurrent episodes, cold sore history, unilateral always |
| Appearance of infiltrates | Multiple, bilateral, scattered, no staining, no vascularisation | Disc-shaped central oedema (disciform), KPs underneath, mild AC reaction |
| Corneal sensation | Normal | Reduced - this is the key test |
| Dendrite history | Never | May have had dendritic ulcer in the past |
| Vascularisation | Absent | May be present in stromal disease |
| Staining | No staining | May have faint staining in active epithelial disease |
- Normal sensation → adenovirus
- Reduced sensation → HSV has damaged the trigeminal nerve endings
Q6 - Seidel Test
- Risk of infection entering the eye → endophthalmitis
- Risk of iris/vitreous prolapse
- Do NOT patch tightly, do NOT put any drops with preservatives
- Apply a rigid shield (not a pad) to protect the eye
- Refer urgently to theatre for primary surgical repair
- Give IV antibiotics prophylactically
desmatocele; DM, can perforate anytime; avoid sternous activity, sneezing
- Admit the patient - do not send home
- Stop all preserved drops immediately (toxic to the already-fragile surface)
- Bandage contact lens or cyanoacrylate glue (tissue adhesive) as a temporising measure
- Urgent penetrating keratoplasty or tectonic graft to restore structural integrity
- Treat the underlying cause (infection, autoimmune)
Final Session Score
| Q | Topic | Score |
|---|---|---|
| 1 | PEE - inferior location | 4.5/5 |
| 2 | Bullae + Fuchs | 3/3 |
| 3 | UV keratopathy + antibiotics | 1.5/3 |
| 4 | PEDAL | 5/5 |
| 4b | Scraping before antibiotics | 0/1 |
| 5 | Subepithelial infiltrates | 2/3 |
| 6 | Seidel test | 1.5/3 |
| 7 | Descemetocele | 3/3 |
| Total | 20.5/26 = 79% |
more
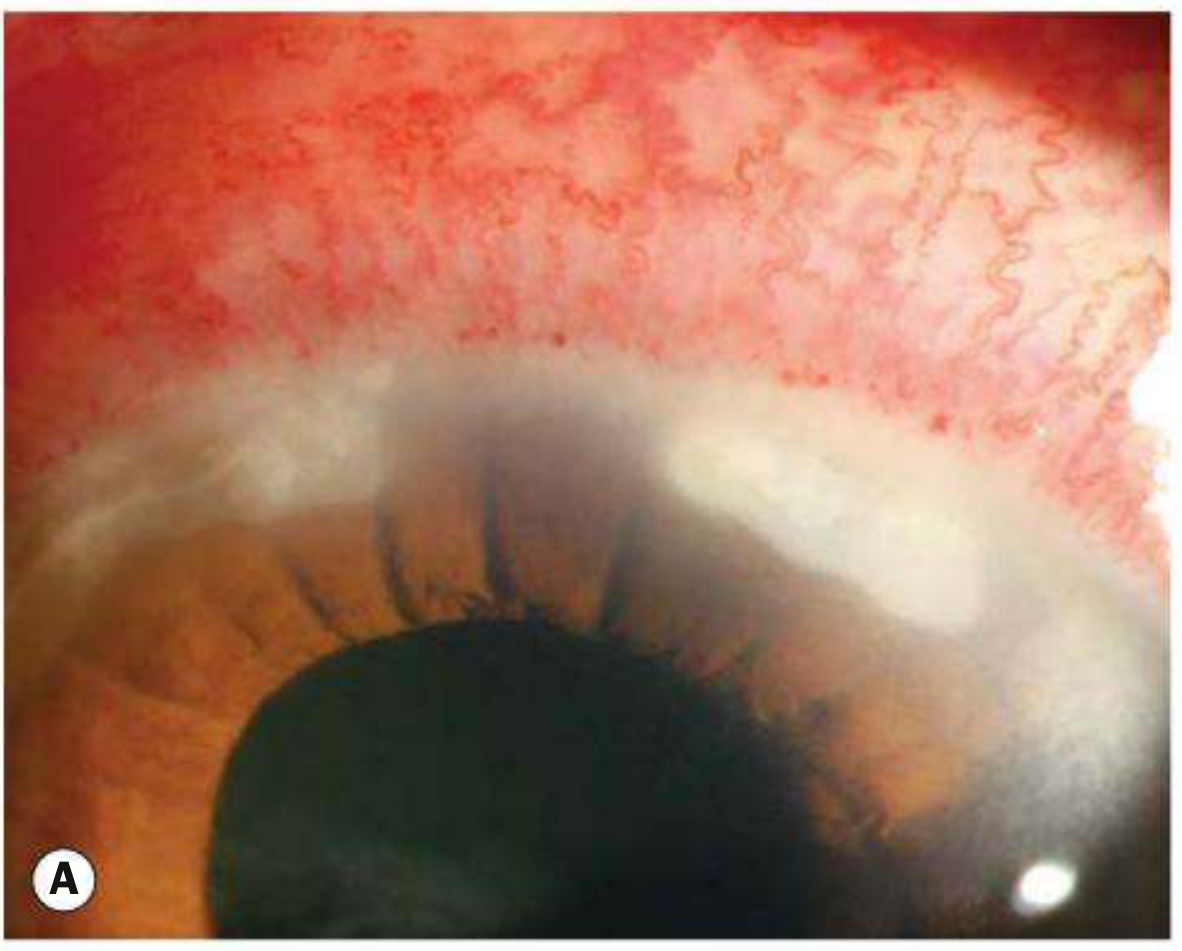
- Small white opacity at the 3 o'clock position, peripheral cornea
- A clear gap of about 1-2 mm between the opacity and the limbus
- Mild redness
- Minimal pain
- Both eyes affected
- Has crusty eyelids in the morning
- Crescent-shaped ulcer at the peripheral cornea
- NO clear gap - the ulcer runs right up to the limbus
- Severe pain
- Progressive - getting worse each day
- Slit-lamp shows the cornea is thinning and "melting"
- Bloods show positive RF and anti-CCP
a: arcus senilis with acute purulent conjunctivitis. b. Peripheral ulcerative keratitis. c. systemic disease has not been mentioned but usually occurs in autiimmune condition. d.lucid interval
- Marginal keratitis = clear zone present between ulcer and limbus
- PUK / Mooren = no clear zone - ulcer reaches right to the limbus
Clear zone = Marginal keratitis (sterile, treat with steroid + treat blepharitis) No clear zone + melting = PUK (autoimmune, screen for RA/vasculitis, needs systemic immunosuppression)
- Patient X: You suspect dry eye with filaments
- Patient Y: You suspect a corneal abrasion (epithelial defect)
- Patient Z: You suspect a herpetic dendrite - you want to see the devitalized cells at the edges clearly
x: rose bengal, ED: fluorescein, herpetic: both rose bengal for bulb
- Fluorescein → stains the ulcer base (the actual defect) green
- Rose bengal → stains the terminal bulbs and devitalized cells at the edges pink - this is what makes the dendrite look like a classic branching pattern with bulbs at the tips
| Dye | Under cobalt blue light | What it stains |
|---|---|---|
| Fluorescein | Bright yellow-green | Epithelial defects (breaks in tight junctions) |
| Rose bengal | Red/pink (no blue light needed - seen in white light) | Devitalized cells, mucus, filaments |
| Lissamine green | Green (white light) | Same as rose bengal but less irritating to patient |
- Blurry vision
- The cornea looks hazy and slightly cloudy
- On slit-lamp you see fine parallel wavy lines running across the deep cornea
- No epithelial defect, no infiltrate, no discharge
DM folds, DM, endothelium damage during surgery, no
- Topical steroids (prednisolone 1%) - reduce post-operative inflammation
- Hypertonic saline drops (5% NaCl) - draws water out of the oedematous cornea osmotically
- Monitor - mild post-op DM folds often resolve within days as the endothelium recovers
- If not improving → check specular microscopy → consider DMEK if endothelial count critically low
Session 2 Complete - Final Tally
| Q | Topic | Score |
|---|---|---|
| 8 | Marginal keratitis vs PUK | 2/4 |
| 9 | Fluorescein vs Rose bengal | 2.5/3 |
| 10 | DM folds post cataract surgery | 4/4 |
| Session 2 subtotal | 8.5/11 |
Overall Score (Both Sessions)
| Session | Score |
|---|---|
| Session 1 (Q1-7) | 20.5/26 |
| Session 2 (Q8-10) | 8.5/11 |
| Grand Total | 29/37 = 78% |
- Strong: sign identification, emergency recognition, clinical reasoning
- Needs work: specific drug names, eponyms/test names, clear zone terminology
how does the stain work? what are the principles of staining? why do specific type of stain is used in specific disease?
The Core Principle
A healthy cell with an intact membrane does NOT let dye in. A dead, dying, or membrane-damaged cell DOES.
Fluorescein - "The Defect Detector"
- Epithelial defects (abrasions, ulcers)
- PEE (tiny inter-cell gaps)
- The base of a dendritic ulcer
- Aqueous leaks (Seidel test - fluorescein is diluted by aqueous → colour shift)
- Dead cells with intact membranes
- Mucus
- Devitalized but still-attached cells
Rose Bengal - "The Dead Cell Detector"
Healthy cells are protected from rose bengal staining by the tear film mucin layer coating their surface. When cells are devitalized, they lose this mucin protection → rose bengal penetrates and stains them red.
- Devitalized epithelial cells (dry eye, exposure, toxicity)
- Mucus filaments (dry eye filaments)
- Terminal bulbs of HSV dendrite (the bulb cells are devitalized virus-infected cells)
- Edges of a dendritic ulcer (surrounding devitalized cells)
Lissamine Green - "The Gentle Rose Bengal"
Side by Side Comparison
| Feature | Fluorescein | Rose Bengal | Lissamine Green |
|---|---|---|---|
| What it stains | Gaps between cells (defects) | Dead/devitalized cells + mucus | Dead/devitalized cells + mucus |
| Mechanism | Pools in epithelial gaps | Penetrates cells without mucin protection | Same as rose bengal |
| Colour | Yellow-green | Red/pink | Green |
| Light needed | Cobalt blue (fluorescence) | White light | White light |
| Pain on instillation | None | Significant stinging | Minimal |
| Best for | Abrasions, ulcers, Seidel test, PEE | Filaments, dry eye severity, HSV dendrite edges | Dry eye, filaments (better tolerated) |
Why Specific Stains for Specific Diseases
- The floor of the ulcer = epithelial defect = Fluorescein stains it green
- The terminal bulbs and edges = devitalized virus-infected cells still sitting there = Rose bengal stains them red
- Using both together gives you the full picture of the dendrite - floor + outline
One Sentence Summary for Each
- Fluorescein = shows you where cells are missing (gaps, defects, leaks)
- Rose bengal = shows you where cells are dead but still present
- Lissamine green = same as rose bengal, better tolerated
what are the different stains used in ophthalmology
GROUP 1: CLINICAL STAINS (Used on the Patient)
1. Fluorescein
- Corneal abrasions, ulcers
- PEE in dry eye
- Dendrite floor in HSV
- Seidel test (aqueous leak)
- Applanation tonometry (mixed with anaesthetic in Minims)
- Contact lens fitting (fluorescein pattern)
- Fundus fluorescein angiography (IV form - different use)
2. Rose Bengal
- Dry eye severity (van Bijsterveld score)
- Filaments
- HSV dendrite edges + terminal bulbs
- Sicca syndrome assessment (Sjogren's) Problem: Stings significantly on instillation
3. Lissamine Green
4. Indocyanine Green (ICG)
- ICG angiography - for choroidal neovascularisation (polypoidal choroidal vasculopathy, occult CNV)
- Where fluorescein angiography is inadequate (blocked by haemorrhage, RPE) Note: Can cause anaphylaxis in iodine-allergic patients
5. Trypan Blue
- Cataract surgery - stains the anterior lens capsule to make it visible during capsulorhexis (especially useful in mature/white cataracts where the red reflex is absent)
- DMEK/DSAEK surgery - stains the donor graft to help orientation
- Vitreoretinal surgery - stains epiretinal membranes
6. Brilliant Blue G
- Vitreoretinal surgery - ILM peeling for macular hole, epiretinal membrane
- Visualizes the thin transparent ILM that is otherwise invisible
7. Triamcinolone Acetonide (off-label stain)
- Vitreoretinal surgery - stains vitreous white, making it visible during vitrectomy
- Helps ensure complete vitreous removal
GROUP 2: LABORATORY STAINS (Corneal Scraping / Histology)
For Microbiology (Corneal Scraping)
| Stain | What it shows | Used for |
|---|---|---|
| Gram stain | Gram +ve (purple) / Gram -ve (pink) bacteria | Bacterial keratitis - identifies organism type immediately |
| Giemsa stain | Cell morphology, bacteria, fungi, protozoa | Bacterial, fungal, Acanthamoeba (cysts + trophozoites) |
| KOH (potassium hydroxide) | Dissolves human cells, leaves fungal hyphae visible | Fungal keratitis - rapid bedside test |
| Calcofluor white | Fluoresces fungal cell walls + Acanthamoeba cysts | Fungal and Acanthamoeba - very sensitive |
| Ziehl-Neelsen (ZN) | Acid-fast organisms (red) | Mycobacterial keratitis (non-tuberculous mycobacteria after LASIK) |
For Histopathology (Tissue / Biopsy)
| Stain | What it shows | Ophthalmic use |
|---|---|---|
| H&E (Haematoxylin & Eosin) | General tissue architecture | Baseline for all biopsies |
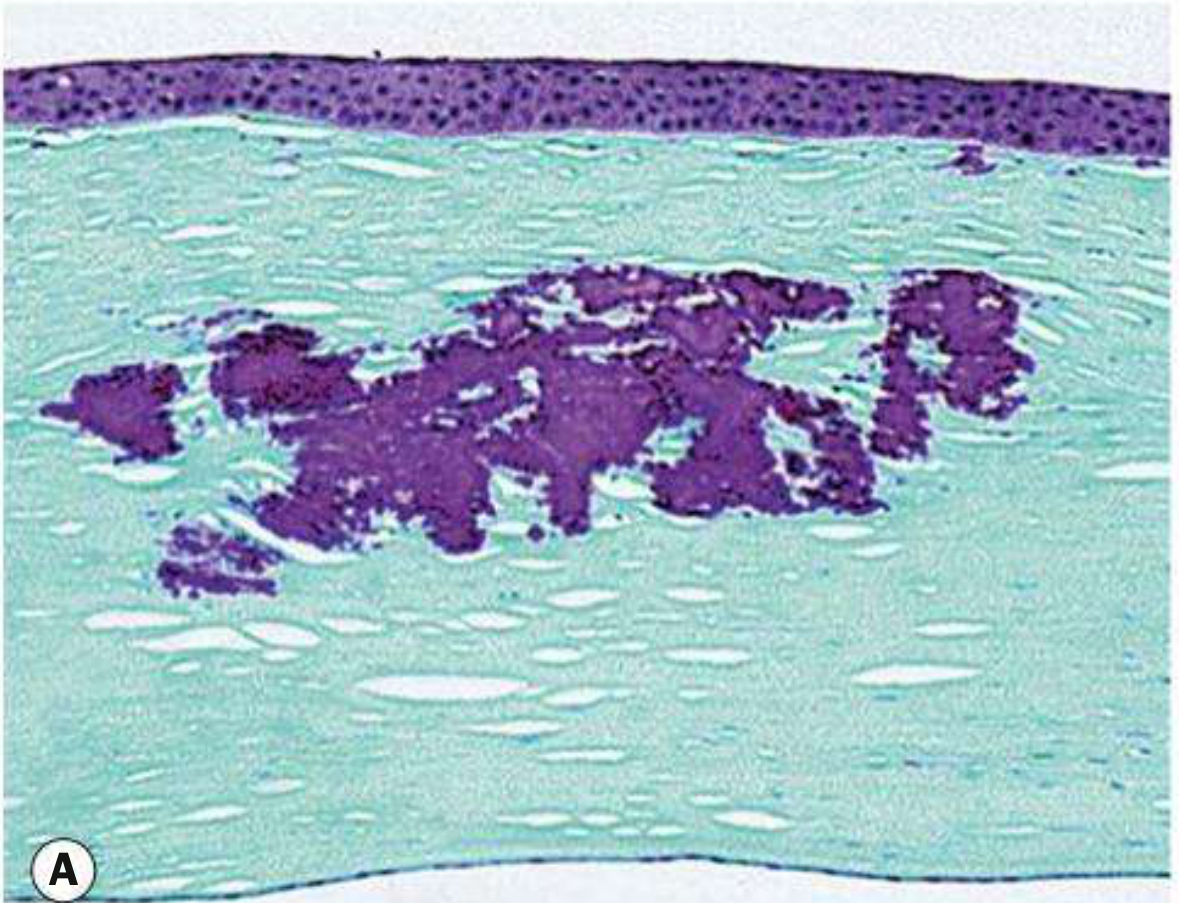
| Masson Trichrome | Hyaline (red) | Granular corneal dystrophy - deposits stain red |
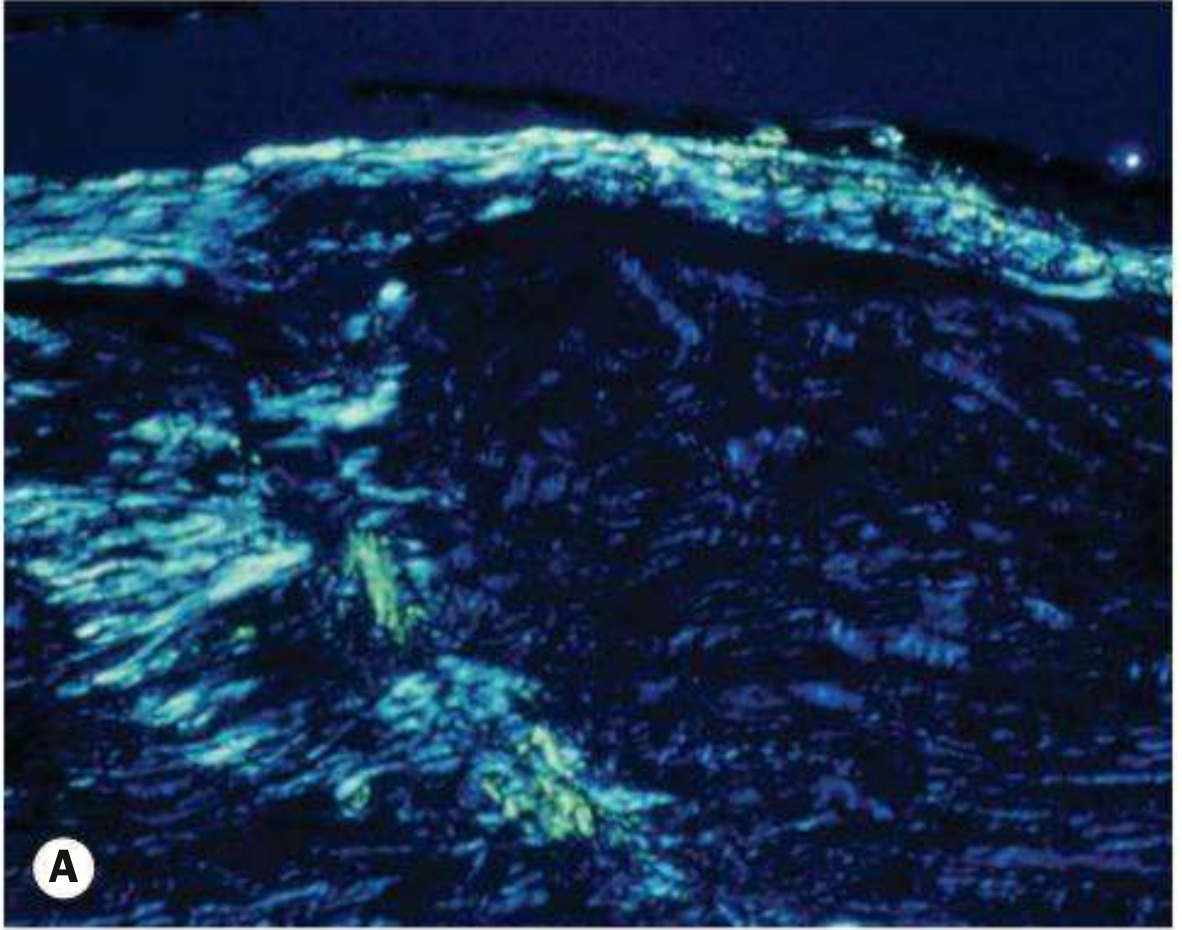
| Congo Red | Amyloid (salmon pink) - green birefringence under polarised light | Lattice corneal dystrophy - amyloid deposits |
| Alcian Blue / PAS | Mucopolysaccharides / GAGs (blue) | Macular corneal dystrophy - keratan sulfate deposits |
| PAS (Periodic Acid Schiff) | Fungal cell walls, basement membranes, mucins | Fungal infections, basement membrane pathology |
| Alcian Blue | Acid mucopolysaccharides | Macular dystrophy, mucin |
| Perl's Prussian Blue | Iron (blue) | Siderosis bulbi, iron foreign body |
| Oil Red O | Lipids | Lipid keratopathy, Schnyder crystalline dystrophy |
| Von Kossa | Calcium (black) | Band keratopathy |
The Three Corneal Dystrophies - Stain Summary (High Yield)
| Dystrophy | Deposit | Stain | Colour |
|---|---|---|---|
| Granular | Hyaline protein | Masson Trichrome | Red |
| Lattice | Amyloid | Congo Red | Green birefringence under polarised light |
| Macular | Keratan sulphate (GAG) | Alcian Blue / PAS | Blue |
Quick Summary Table
| Category | Stain | Key Use |
|---|---|---|
| Clinical - defects | Fluorescein | Abrasions, ulcers, Seidel |
| Clinical - dead cells | Rose bengal / Lissamine green | Dry eye, HSV bulbs |
| Clinical - surgical | Trypan blue | Capsulorhexis in white cataract |
| Clinical - ILM | Brilliant blue G | Macular hole surgery |
| Lab - bacteria | Gram, Giemsa | Corneal scraping |
| Lab - fungi | KOH, Calcofluor, PAS | Fungal keratitis |
| Lab - Acanthamoeba | Giemsa, Calcofluor | Ring infiltrate, CL wearer |
| Lab - dystrophies | Masson/Congo/Alcian | Granular/Lattice/Macular |
| Lab - calcium | Von Kossa | Band keratopathy |
| Lab - iron | Perl's Prussian Blue | Siderosis |
| Lab - amyloid | Congo Red | Lattice dystrophy, AL amyloid |
give the clinical images to each
Stains in Ophthalmology - With Clinical Images
CLINICAL STAINS (Used on the Patient)
1. Fluorescein - "Shows gaps/defects"
- Panel A = Fluorescein showing PEE (dry eye) - tiny green dots on cobalt blue background
- Panel D = Fluorescein showing bullous keratopathy - the large green pool is where a bulla has ruptured, leaving an epithelial defect
2. Rose Bengal - "Shows dead cells + mucus"
LABORATORY / HISTOLOGY STAINS
3. Masson Trichrome - "Granular dystrophy"

4. Congo Red - "Lattice dystrophy (Amyloid)"
"Histology showing green birefringence of amyloid when viewed through polarised light"
5. Alcian Blue / PAS - "Macular dystrophy (Keratan sulphate/GAG)"
THE 3 DYSTROPHY STAINS SIDE BY SIDE
| Dystrophy | Deposit | Stain | Colour | Vision |
|---|---|---|---|---|
| Granular | Hyaline | Masson Trichrome | Red | Relatively preserved |
| Lattice | Amyloid | Congo Red | Apple-green (polarised) | Moderate loss |
| Macular | Keratan sulphate (GAG) | Alcian Blue | Blue | Worst - earliest loss |
SURGICAL STAINS
6. Trypan Blue - "Cataract surgery / DMEK"
QUICK VISUAL SUMMARY
| Stain | Colour seen | Where used | What it finds |
|---|---|---|---|
| Fluorescein (cobalt blue light) | Yellow-green glow | Slit-lamp | Epithelial gaps, defects, leaks |
| Rose Bengal (white light) | Red/pink | Slit-lamp | Dead cells, mucus, dendrite edges |
| Lissamine Green (white light) | Green | Slit-lamp | Same as rose bengal, less stinging |
| Masson Trichrome (histology) | Red deposits on green background | Lab | Granular dystrophy (hyaline) |
| Congo Red polarised (histology) | Apple-green birefringence | Lab | Lattice dystrophy (amyloid) |
| Alcian Blue (histology) | Blue | Lab | Macular dystrophy (GAG/keratan sulphate) |
| Gram (lab) | Purple/pink | Lab | Bacteria type (bacterial keratitis) |
| KOH (lab) | Unstained hyphae visible | Lab | Fungal keratitis |
| Trypan Blue (surgical) | Blue | OT | Capsule staining (white cataract), DMEK graft |
Test me on clinical stains with case scenarios
fluorescein
- Fluorescein - shows the epithelial defects (PEE)
- Rose bengal / Lissamine green - shows the devitalized cells AND the mucus filaments
- Fluorescein → tiny bright yellow-green dots (PEE) scattered across the exposed cornea under cobalt blue light
- Rose bengal / Lissamine green → pink/red staining of devitalized cells on cornea AND conjunctiva; if filaments are present, they stain brightly as red thread-like strands
filaments, rose bengal. stains the devitalized tissue
- See the full extent of the ulcer floor
- See the terminal bulbs and devitalized edges clearly