Angular deformity 15 marks structured answer for knruhs
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content. Let me compile a complete, exam-quality 15-mark structured answer for KNRUHS on Angular Deformity.
Angular Deformity - 15 Marks Structured Answer (KNRUHS)
Definition
Angular deformity is an abnormal deviation of a bone or limb from its normal alignment in the coronal, sagittal, or axial plane. In the lower limb, the normal mechanical axis (Mikulicz line) runs from the center of the femoral head through the intercondylar eminence of the tibial plateau to the center of the ankle mortise. Any deviation from this line constitutes an angular deformity.
- Normal femorotibial angle: The anatomic axes of femur and tibia form a laterally open angle of 174° at the knee (i.e., 6° of physiologic valgus).
Terminology / Types
| Term | Meaning | Location |
|---|---|---|
| Genu varum | Knee deviates medially; center of knee lateral to mechanical axis ("bow legs") | Knee - tibia/femur |
| Genu valgum | Knee deviates laterally; center of knee medial to mechanical axis ("knock knees") | Knee - tibia/femur |
| Cubitus varus | Carrying angle < normal ("gunstock deformity") | Elbow |
| Cubitus valgus | Carrying angle > normal (>15°) | Elbow |
| Coxa vara | Neck-shaft angle < 120° | Hip |
| Coxa valga | Neck-shaft angle > 140° | Hip |
| Hallux valgus | Lateral deviation of great toe | Foot |
| Varus | Apex of deformity points laterally; distal part angulates medially | |
| Valgus | Apex points medially; distal part angulates laterally |
Physiologic Angular Changes with Age (Normal Development)
Angular alignment changes normally in children - it is important to distinguish physiologic from pathologic:
| Age | Normal Alignment |
|---|---|
| Birth - 1 year | Up to 20° genu varum is normal |
| 18 months - 2 years | Varum transitions to valgum (by ~2.5 years) |
| 2 - 4 years | Up to 10° genu valgum is normal |
| 6-7 years | Adult alignment achieved (~6° valgus) |
An intercondylar distance >3 cm (in genu varum) or intermalleolar distance >5 cm (in genu valgum) is considered clinically abnormal.
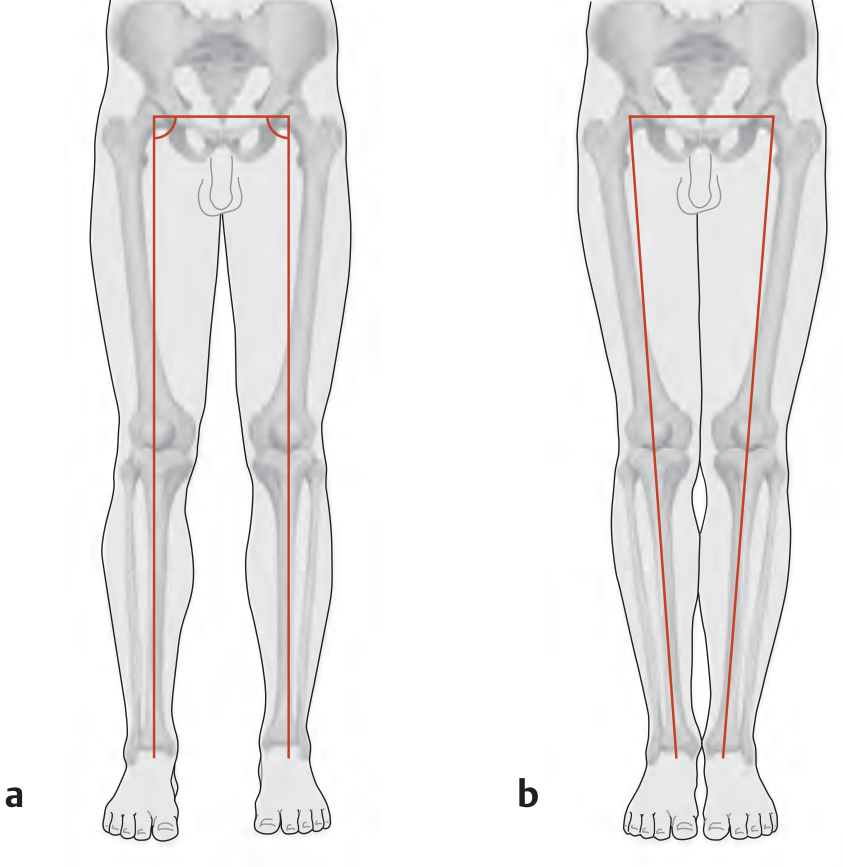
Mechanical axis (Mikulicz line): (a) normal rectangular alignment; (b) genu valgum - trapezoid shape - Campbell's Operative Orthopaedics / THIEME Atlas
Etiology / Causes
A. Congenital
- Congenital bowing of tibia (posteromedial / anterolateral)
- Coxa vara congenita
- Achondroplasia and skeletal dysplasias (disproportionately short extremities → genu varum; short trunk → genu valgum)
- Osteogenesis imperfecta
B. Developmental
- Physiologic - normal variant in children (see above)
- Blount's disease (tibia vara) - abnormal growth of posteromedial tibial physis
- Infantile (0-4 yrs): bilateral, obese early walkers; internal tibial torsion; Drennan's metaphyseal-diaphyseal angle > 16° is pathologic; Langenskiold classification (Stages I-VI)
- Adolescent (8-15 yrs): usually unilateral, obesity-related
C. Traumatic
- Malunion after fractures (commonest cause in adults)
- Physeal arrest after growth plate injury (Salter-Harris fractures, especially distal femur - high rate of angular deformity)
- Traction pin through proximal tibial physis → genu recurvatum
- Supracondylar fracture of humerus → cubitus varus (gunstock deformity) - most common angular deformity of elbow in children
D. Metabolic / Nutritional
- Rickets (nutritional, renal osteodystrophy, vitamin D-resistant) → genu varum/valgum
- Paget's disease → bowing of long bones
E. Infective
- Osteomyelitis/septic arthritis damaging growth plates → limb length discrepancy and angular deformity
F. Neoplastic
- Osteochondromas tethering growth → angular deformity (e.g., multiple hereditary exostoses)
- Fibrous dysplasia → "shepherd's crook" deformity of proximal femur
G. Neuromuscular
- Cerebral palsy, poliomyelitis → muscle imbalance → angular deformity
Clinical Assessment
History
- Age of onset, progression, family history, trauma, nutritional status
- Symptoms: pain, cosmetic concern, gait abnormality
Clinical Examination
Measurement of deformity:
- Genu varum: Measure intercondylar distance (knees together, feet together; >3 cm = abnormal)
- Genu valgum: Measure intermalleolar distance (knees together; >5 cm = abnormal)
- Cubitus varus/valgus: Measure carrying angle (normal 5-15° valgus in adults)
Assess:
- Site, direction, degree of angulation
- Rotational deformity (often coexists)
- Leg length discrepancy
- Joint stability (ligamentous laxity vs. bony deformity)
- Neurovascular status
Radiological Assessment
- Full-length standing AP radiograph of lower limbs (scanogram) - from femoral head to ankle
- Measure:
- Mechanical axis deviation (MAD): Distance of mechanical axis from center of tibial plateau (normal = 0-10 mm medial)
- Mechanical lateral distal femoral angle (mLDFA): Normal = 88° ± 3°
- Medial proximal tibial angle (MPTA): Normal = 87° ± 3°
- CORA (Center of Rotation of Angulation): Point where bisectors of proximal and distal bone segments intersect - the apex of the deformity; guides the level of corrective osteotomy
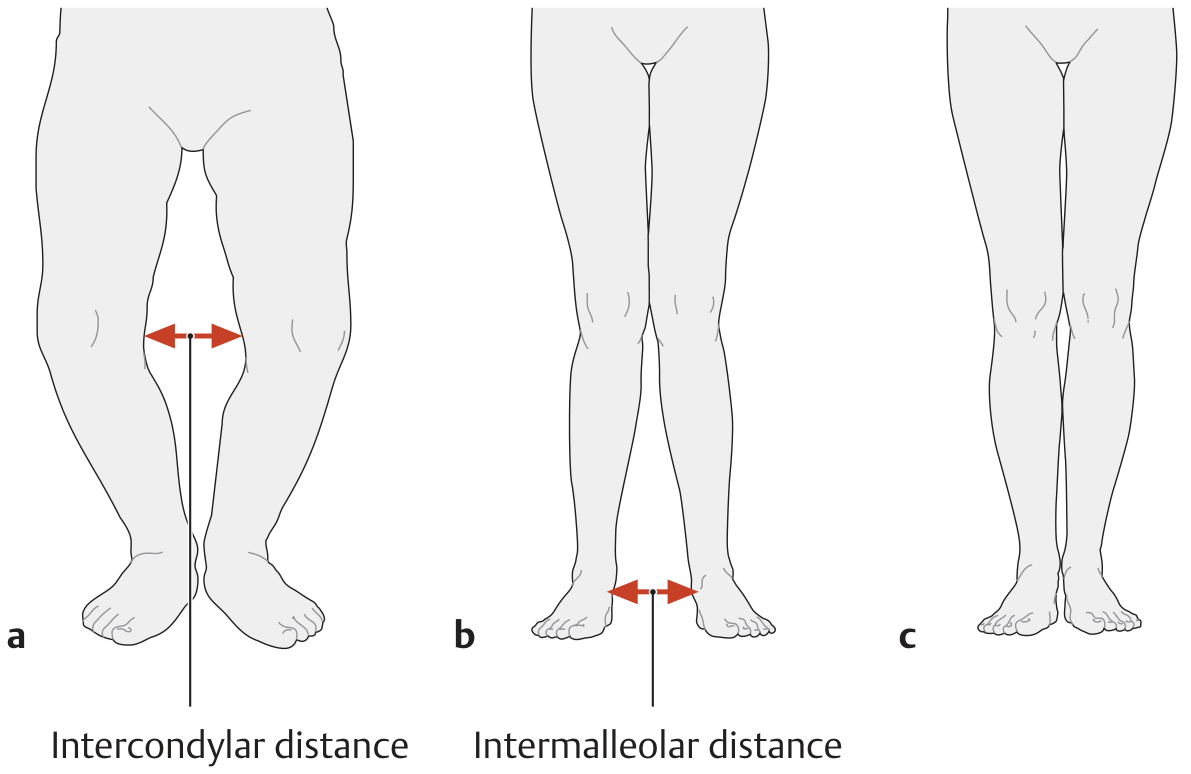
Clinical measurement: (a) intercondylar distance for genu varum; (b) intermalleolar distance for genu valgum - THIEME Atlas of Anatomy
Pathological Consequences of Untreated Angular Deformity
- Genu varum: Increased medial compartment loading → medial joint OA; lateral collateral ligament and iliotibial band tension; stress on lateral foot border
- Genu valgum: Increased lateral compartment loading → lateral joint OA; medial ligament stretching; patellofemoral maltracking
- Abnormal joint loading leads to premature osteoarthritis
- Limb length inequality if asymmetric
- Compensatory deformities in adjacent joints
Treatment
Conservative (Non-operative)
- Observation: Physiologic deformities in children self-correct with growth; reassure parents
- Bracing / Orthoses:
- Infantile Blount disease (Langenskiold Stage I-II, age < 3 years): knee-ankle-foot orthosis (KAFO) used until age 3, then consider surgery if no improvement
- Rickets: treat underlying metabolic cause; deformity may correct with medical management
Operative Treatment - Indications
- Deformity not correcting with growth/conservative measures
- Progressive deformity
- Symptomatic (pain, gait disturbance, limb length discrepancy)
- Angular deformity causing significant joint stress or secondary OA
- In post-fracture malunion: corrective osteotomy delayed at least 1 year unless function impaired
Osteotomy - Principles
The osteotomy should ideally be performed at the CORA (apex of deformity) to avoid translation:
- Opening wedge osteotomy: Bone defect filled with graft; opens on concave side; fixation with plate
- Closing wedge osteotomy: Bone removed on convex side; shortens limb slightly but more stable healing
- Dome (barrel vault) osteotomy: Used near physis; no limb length change
- Acute vs. gradual correction: Acute correction (osteotomy + plate/nail) vs. gradual (external fixator, Ilizarov, Taylor Spatial Frame)
Specific Procedures by Location
| Deformity | Procedure |
|---|---|
| Genu varum (medial OA) | High tibial osteotomy (HTO) - opening/closing wedge; supracondylar femoral osteotomy |
| Genu valgum | Distal femoral osteotomy (varus-producing); supramalleolar osteotomy if deformity at ankle |
| Cubitus varus (post-supracondylar #) | Lateral closing wedge supracondylar osteotomy of humerus |
| Blount's disease | Tibia vara correction (proximal tibial + fibular osteotomy); epiphyseal stapling (hemiepiphysiodesis) for younger children |
| Rickets bowing | Correct metabolic disease first; osteotomy if residual deformity |
| Osteogenesis imperfecta | Sofield-Millar procedure (fragmentation and realignment with intramedullary rod e.g., Fassier-Duval telescopic rod) for genu varum/valgum |
Epiphysiodesis / Guided Growth
- In skeletally immature patients with sufficient growth remaining
- Hemiepiphysiodesis: Temporary tethering of the growth plate on the convex side using staples or tension band plate (8-plate) to gradually correct the deformity
- Advantages: minimally invasive, gradual, reversible
- Used for Blount disease, rickets, idiopathic valgus/varus in children
Complications of Corrective Osteotomy
- Neurovascular injury (especially anterior tibial artery at HTO - compression with valgus correction, stretching with varus correction)
- Anterior compartment syndrome (post HTO)
- Peroneal nerve palsy
- Over/under-correction
- Delayed union / non-union
- Infection
- Late angular deformity recurrence (up to 46% in some series; revision rates 19-40%)
Summary Table
| Parameter | Genu Varum | Genu Valgum |
|---|---|---|
| Clinical test | Intercondylar gap >3 cm | Intermalleolar gap >5 cm |
| Mechanical axis | Knee lateral to axis | Knee medial to axis |
| Joint at risk | Medial OA | Lateral OA / patellofemoral |
| Common cause in children | Blount's, rickets | Rickets, idiopathic |
| Common cause in adults | Post-traumatic malunion, OA | Post-traumatic, OA |
| Primary operative procedure | High tibial osteotomy | Distal femoral osteotomy |
Sources: Campbell's Operative Orthopaedics 15th Ed 2026 | Miller's Review of Orthopaedics 9th Ed | THIEME Atlas of General Anatomy and Musculoskeletal System | Rockwood & Green's Fractures in Adults 10th Ed 2025
What examiner expects
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.