Teach osteoporosis pharmacology all from definition and classification to adr and uses and indications from the standard books like kdt and katzung
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Osteoporosis Pharmacology - Complete Guide
Sources: Katzung's Basic and Clinical Pharmacology, 16th Ed. | Lippincott Illustrated Reviews: Pharmacology
SECTION 1: DEFINITION
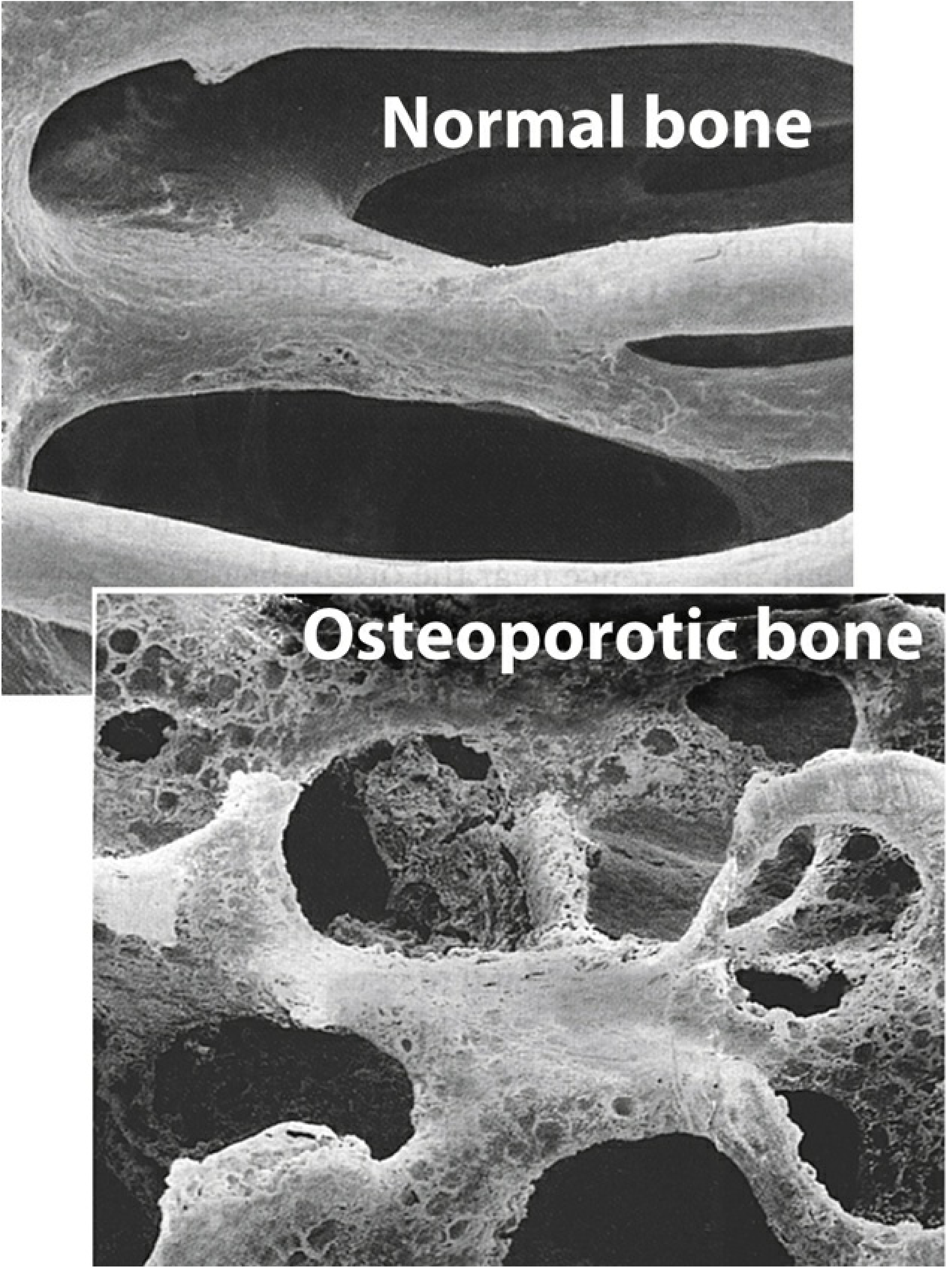
Osteoporosis is defined as abnormal loss of bone predisposing to fractures. It is characterized by progressive loss of bone mass and skeletal fragility, leading to increased fracture risk. It occurs most frequently in postmenopausal women but also affects older men.
- Katzung, p. 1226 | Lippincott Pharmacology, p. 887
Normal bone vs osteoporotic bone - comparison of trabecular architecture:
SECTION 2: CLASSIFICATION / CAUSES
| Type | Cause |
|---|---|
| Postmenopausal (Type I) | Loss of estrogen leads to increased osteoclast activity |
| Senile / Age-related (Type II) | Occurs in both sexes with aging |
| Secondary Osteoporosis | Due to drugs or diseases |
Causes of secondary osteoporosis include:
- Long-term glucocorticoids (most common drug cause)
- Antiandrogen therapy (e.g., prostate cancer treatment)
- Thyrotoxicosis, hyperparathyroidism
- Malabsorption syndromes
- Alcohol abuse and cigarette smoking
- Idiopathic
Drugs that increase bone loss / fracture risk (Lippincott Fig. 27.3):
| Drug | Drug |
|---|---|
| Glucocorticoids | Aluminum antacids |
| Aromatase inhibitors | Anticonvulsants (phenytoin) |
| Furosemide | Heparin |
| Proton pump inhibitors | SSRIs |
| Medroxyprogesterone acetate | Thiazolidinediones |
| Thyroid hormone (excessive) |
SECTION 3: BONE REMODELING (Pathophysiology)
Throughout life, ~10% of the skeleton is replaced each year. The cycle involves:
- Osteoclasts - break down bone (resorption)
- Osteoblasts - synthesize new bone (formation)
- Hydroxyapatite crystals (calcium phosphate) are deposited during mineralization
In osteoporosis: bone resorption exceeds bone formation. Estrogen normally suppresses osteoclast proliferation; its loss at menopause triggers rapid bone loss.
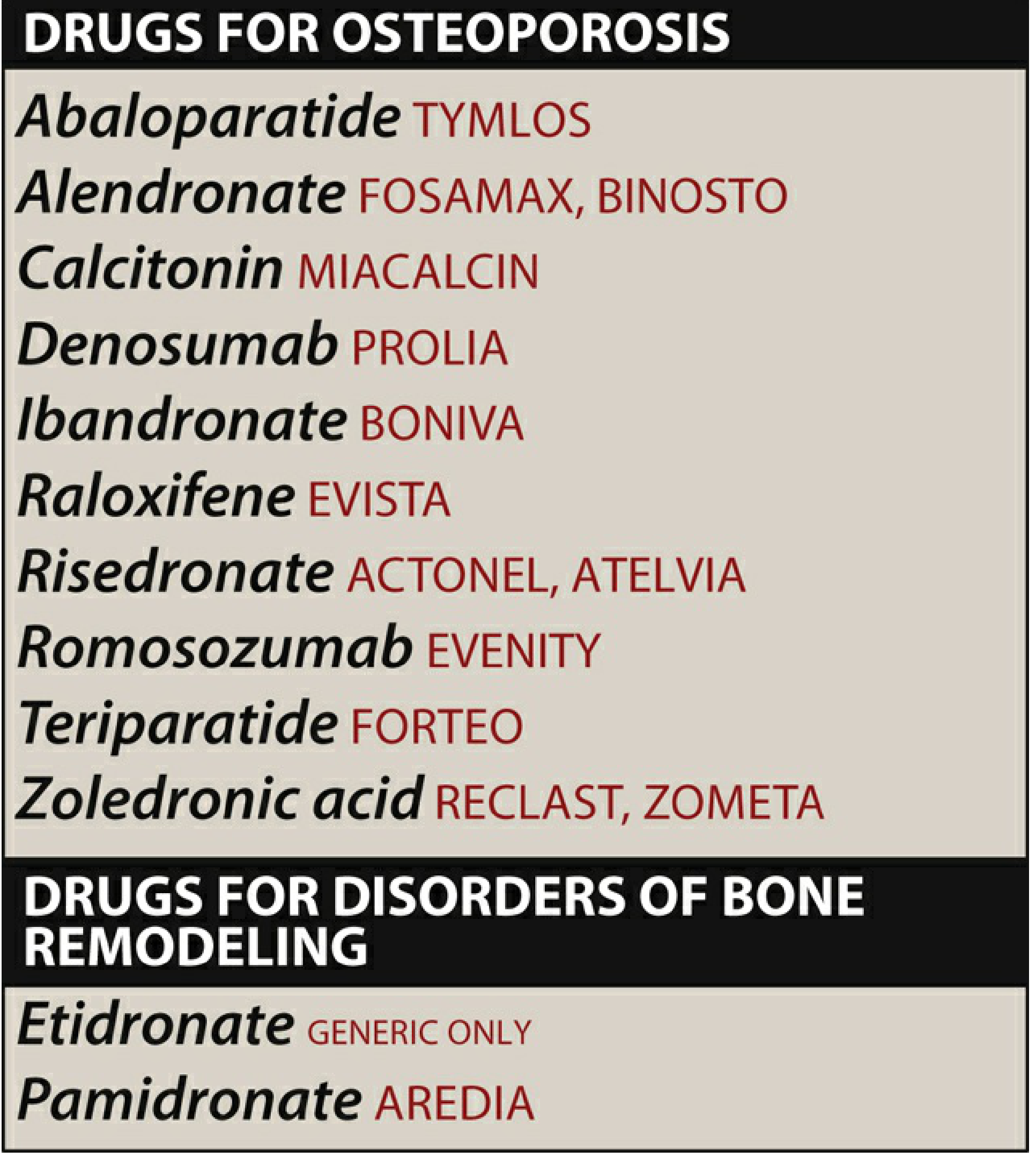
SECTION 4: DRUGS USED IN OSTEOPOROSIS
Classification of Anti-Osteoporosis Drugs
A. ANTIRESORPTIVE AGENTS (inhibit bone resorption)
1. Bisphosphonates
2. Denosumab (RANKL inhibitor)
3. SERMs (Raloxifene)
4. Estrogen / HRT
5. Calcitonin
B. ANABOLIC AGENTS (stimulate bone formation)
1. Teriparatide (PTH 1-34)
2. Abaloparatide (PTHrP analog)
3. Romosozumab (sclerostin inhibitor - dual action)
C. NON-PHARMACOLOGIC
Calcium + Vitamin D supplementation
SECTION 5: BISPHOSPHONATES
Drugs in Class
Alendronate, Risedronate, Ibandronate, Zoledronic acid, Etidronate, Pamidronate
Antiresorptive Potency (Relative)
| Drug | Relative Potency |
|---|---|
| Etidronate | 1 |
| Tiludronate | 10 |
| Pamidronate | 100 |
| Alendronate | 1,000 |
| Risedronate | 5,000 |
| Ibandronate | 10,000 |
| Zoledronic acid | 10,000 |
Lippincott Pharmacology, p. 893
Mechanism of Action
Bisphosphonates bind to hydroxyapatite crystals in bone and decrease osteoclastic bone resorption, resulting in a small increase in bone mass and decreased fracture risk. They are structural analogs of pyrophosphate - nitrogen-containing bisphosphonates (alendronate, risedronate, zoledronate) inhibit farnesyl pyrophosphate synthase, disrupting osteoclast cytoskeletal function and triggering apoptosis.
Dosing Schedule
| Drug | Route | Frequency |
|---|---|---|
| Alendronate | Oral tablet | Daily (10 mg) or Weekly (70 mg) |
| Risedronate | Oral tablet | Daily (5 mg), Weekly (35 mg), or Monthly |
| Ibandronate | Oral / IV | Monthly (150 mg oral) / Every 3 months (3 mg IV) |
| Zoledronic acid | IV only | Once yearly (5 mg) |
Administration Rules for Oral Bisphosphonates
- Take with 6-8 oz plain water ONLY
- Take at least 30 minutes (60 min for ibandronate) BEFORE any food, drink, or medications
- Remain upright (do not lie down) for at least 30 minutes after
- (Exception: risedronate delayed-release - taken AFTER breakfast)
Pharmacokinetics
- Oral bioavailability: <1% - poorly absorbed
- Food and other drugs significantly interfere with absorption
- Rapidly cleared from plasma by avid binding to hydroxyapatite in bone
- Once bound to bone, cleared over hours to years (long half-life in bone)
- Eliminated mainly via kidneys - avoid in severe renal impairment
Indications
- Postmenopausal osteoporosis (first-line)
- Osteoporosis in men
- Glucocorticoid-induced osteoporosis
- Paget disease of bone (higher doses)
- Hypercalcemia of malignancy
- Bone metastases (pamidronate, zoledronate)
Adverse Drug Reactions (ADRs)
- GI upset - nausea, esophageal irritation, dyspepsia (especially alendronate - must stay upright after dosing)
- Osteonecrosis of the Jaw (ONJ) - especially with IV bisphosphonates at high doses
- Atypical femoral fractures - stress fractures of the subtrochanteric femur with long-term use (>5 years)
- Flu-like symptoms - acute phase reaction with IV zoledronate (fever, myalgias, arthralgias)
- Hypocalcemia - particularly with IV forms
- Esophagitis / esophageal ulcers - if patient does not remain upright
Notes (Katzung)
- Side-by-side trials showed alendronate > calcitonin in efficacy
- Bisphosphonates protect against both hip and spine fractures
- BMD benefits plateau after a few years (unlike denosumab)
- A drug holiday is often recommended after 3-5 years in low-risk patients
SECTION 6: DENOSUMAB (RANKL INHIBITOR)
Drug
Denosumab (Prolia - for osteoporosis; Xgeva - for malignancy-related bone disease)
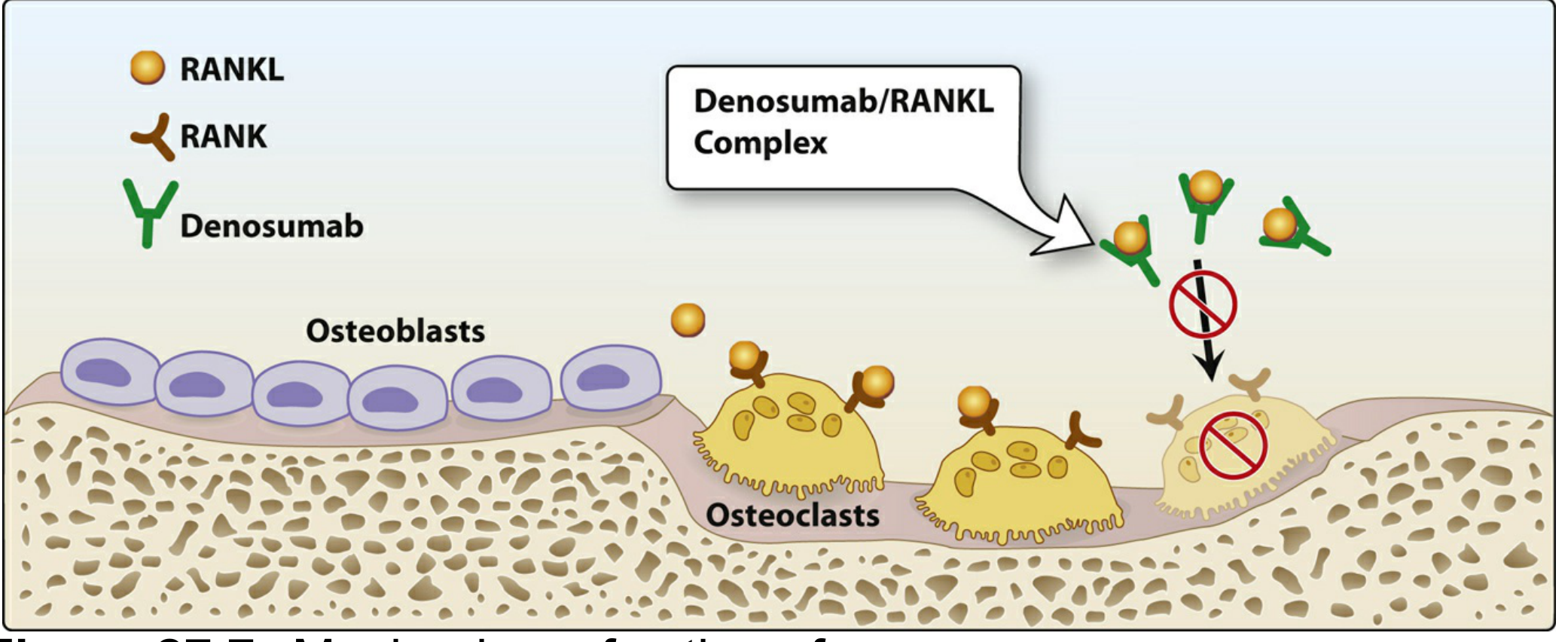
Mechanism of Action
Denosumab is a human monoclonal antibody directed against RANKL (Receptor Activator of Nuclear Factor kappa-B Ligand). By binding to RANKL, it prevents activation of RANK receptors on osteoclasts, thereby inhibiting osteoclast formation, function, and survival - reducing bone resorption.
Dosing
- 60 mg subcutaneous injection every 6 months
Indications
- Postmenopausal osteoporosis in women at high fracture risk
- Osteoporosis in men
- Glucocorticoid-induced osteoporosis
- Hypercalcemia of malignancy (Xgeva formulation)
- Prevention of skeletal-related events in multiple myeloma / bone metastases
Advantages Over Bisphosphonates
- No renal dose adjustment needed
- BMD continues to increase up to 10 years (unlike bisphosphonates which plateau after a couple of years)
- Alternative first-line agent, particularly at higher fracture risk
ADRs
- GI upset, bone pain
- Increased risk of infections (cellulitis, serious infections) - RANKL is also expressed on immune cells
- Dermatologic reactions (eczema, rash)
- Hypocalcemia
- Rarely: ONJ, atypical fractures (like bisphosphonates)
Critical Warning (Katzung)
When denosumab is discontinued, there is often a surge of bone resorption (rebound) that is only partially prevented with antiresorptive agents like zoledronate. Therefore, transitioning to a bisphosphonate on discontinuation is mandatory.
SECTION 7: TERIPARATIDE AND ABALOPARATIDE (ANABOLIC AGENTS)
Drugs
- Teriparatide (Forteo) - recombinant human PTH 1-34
- Abaloparatide (Tymlos) - analog of parathyroid hormone-related peptide (PTHrP)
Mechanism of Action
- Act as agonists at the parathyroid hormone receptor (PTH1R)
- Once-daily subcutaneous administration results in stimulation of osteoblastic activity and increased bone formation and bone strength
- When given intermittently (pulse dosing), the anabolic effect predominates over resorptive effect
- Note: PTH also activates bone resorption, but the net effect is anabolic with this dosing regimen
Dosing
| Drug | Dose | Route | Duration |
|---|---|---|---|
| Teriparatide | 20 mcg daily | SC injection | Max 2 years |
| Abaloparatide | 80 mcg daily | SC injection | Max 2 years |
Indications
- High fracture risk patients
- Patients who have failed or cannot tolerate other therapies
- Severe postmenopausal osteoporosis
Efficacy
- At least as great as bisphosphonates in preventing fractures
- Produces structurally normal new bone (unlike fluoride which produces abnormal bone)
- Effective for both vertebral and nonvertebral fractures
ADRs
- Injection site reactions
- Hypercalcemia (transient)
- Orthostatic hypotension
- Hyperuricemia (abaloparatide)
- Osteosarcoma risk - increased in rats at high doses; contraindicated in patients at risk (Paget disease, prior radiation therapy to bone, unexplained elevations of alkaline phosphatase)
Contraindications
- History of Paget disease
- Prior skeletal radiation
- Unexplained elevated alkaline phosphatase
- Pre-existing hypercalcemia
- Pediatric patients (open epiphyses)
Important (Katzung + Lippincott)
- After completing 2-year course, an antiresorptive agent must be started to maintain BMD gained
- Cumulative lifetime use >2 years is NOT recommended
SECTION 8: ROMOSOZUMAB (SCLEROSTIN INHIBITOR)
Drug
Romosozumab (Evenity)
Mechanism of Action (DUAL - unique)
- Monoclonal antibody against sclerostin
- Sclerostin (produced by osteocytes) is an inhibitor of bone formation via the Wnt signaling pathway
- Romosozumab binds sclerostin → promotes osteoblast activity (anabolic) + decreases bone resorption (antiresorptive)
- The only agent with both effects simultaneously (Katzung Fig. 42-5 shows the highest BMD increase)
Dosing
- 210 mg SC injection monthly (2 injections of 105 mg to give full dose)
- Approved for 12 months only
Indications
- Postmenopausal osteoporosis at high fracture risk
ADRs
- Arthralgias, headache
- Injection site reactions
- Cardiovascular risk - small but significant increase in MI and stroke in clinical trials
Contraindications
- History of MI or stroke (black box warning)
- No renal dose adjustment required
After Therapy
- Must transition to an antiresorptive agent to maintain bone gained
SECTION 9: SELECTIVE ESTROGEN RECEPTOR MODULATORS (SERMs)
Drugs
- Raloxifene (Evista) - available; first SERM approved for osteoporosis
- Bazedoxifene - used in Europe
- Tamoxifen - has bone effects but not approved for osteoporosis
Mechanism of Action
- SERMs are estrogen receptor modulators that act as estrogen agonists on bone (and lipid metabolism) but as estrogen antagonists on breast and endometrial tissue
- Raloxifene prevents the estrogen-deficiency-driven proliferation and activation of osteoclasts
Indications
- Prevention and treatment of postmenopausal osteoporosis (alternative agent)
- Reduces risk of invasive breast cancer (important added benefit)
Limitations vs Bisphosphonates
- Protects against vertebral fractures only - NOT hip or nonvertebral fractures
- Bisphosphonates, denosumab, and teriparatide all protect against both
ADRs
- Hot flashes (leg cramps)
- Venous thromboembolism (VTE) - same risk as estrogen; contraindicated if history of DVT/PE
- Does NOT prevent hot flushes (may worsen them)
- Does NOT increase risk of endometrial or breast cancer
SECTION 10: ESTROGEN / HRT
Mechanism
Estrogen normally suppresses osteoclast proliferation and activation. Its deficiency at menopause leads to accelerated bone loss.
Status
Estrogen replacement was formerly standard of care but enthusiasm has waned because:
- Increases risk of breast cancer with continued use
- Increased risk of endometrial cancer (prevented if combined with progestin in women with uterus)
- Does NOT protect against heart disease and may increase risk
- Combined E+P increases risk of stroke and VTE
Current Role
- No longer routinely recommended as first-line for osteoporosis
- May be considered for women with severe menopausal symptoms who have contraindications or intolerance to first-line agents
SECTION 11: CALCITONIN
Drug
Salmon calcitonin (Miacalcin) - greater potency and longer duration than human calcitonin
Mechanism
- Peptide hormone secreted by thyroid parafollicular cells
- Binds directly to osteoclasts and inhibits their resorptive activity
Formulations
- Intranasal spray (most common for osteoporosis) - rhinitis is main ADR
- Subcutaneous / Intramuscular injection - injection site reactions
Indications
- Treatment of osteoporosis in women at least 5 years postmenopausal (when other agents not tolerated)
- Unique indication: relief of pain from osteoporotic vertebral fracture (analgesic property)
- Paget disease
- Hypercalcemia (acute)
ADRs
- Nasal: rhinitis, epistaxis
- Injectable: nausea, flushing, injection site reactions
- Increased risk of new malignancy with long-term use (limits use)
Limitations (Katzung + Lippincott)
- Less effective than bisphosphonates, denosumab, or teriparatide
- Reduces fractures only in the spine (not hip)
- Should only be used if other agents are inappropriate or not tolerated
SECTION 12: CALCIUM AND VITAMIN D
Role
Foundational supplementation - used adjunctively with all pharmacologic agents.
Calcium
| Form | Elemental Ca% | Notes |
|---|---|---|
| Calcium carbonate | 40% | Inexpensive; take WITH meals; poorly absorbed with PPIs/H2 blockers |
| Calcium citrate | 21% | Better tolerated; can be taken WITH or WITHOUT food; preferred with acid reducers |
ADRs: gas, bloating, constipation
Drug interactions: separates absorption of iron, thyroid hormone, fluoroquinolones, tetracyclines (separate by several hours)
Vitamin D
- Essential for intestinal calcium absorption and bone mineralization
- Vitamin D2 (ergocalciferol) or Vitamin D3 (cholecalciferol) used for supplementation
- 800 IU/day shown to improve bone density, reduce falls, and prevent fractures
- Calcitriol (1,25-(OH)₂D) and 1α(OH)D₃ analogs also used (not FDA-approved for osteoporosis in US)
SECTION 13: INDICATIONS SUMMARY
| Indication | First-Line | Alternatives |
|---|---|---|
| Postmenopausal osteoporosis | Bisphosphonates, Denosumab | Raloxifene, Teriparatide, Romosozumab |
| Osteoporosis in men | Bisphosphonates, Denosumab | Teriparatide |
| Glucocorticoid-induced osteoporosis | Bisphosphonates, Denosumab, Teriparatide | - |
| High fracture risk / failed therapy | Teriparatide, Abaloparatide, Romosozumab | - |
| Vertebral fracture pain | Calcitonin (short-term) | - |
| Paget disease | Bisphosphonates (higher doses) | Calcitonin |
| Hypercalcemia of malignancy | Denosumab, Bisphosphonates (IV), Calcitonin | - |
Threshold for Pharmacologic Treatment (Lippincott, p. 891)
Treatment warranted in postmenopausal women and men ≥50 years with:
- Previous osteoporotic fracture, OR
- BMD T-score ≤ -2.5 (osteoporosis), OR
- Low bone mass (osteopenia) with high probability of future fractures (using FRAX tool)
SECTION 14: BONE MINERAL DENSITY - TREATMENT EFFECTS
The following diagram from Katzung (Fig. 42-5) shows comparative effects on BMD:
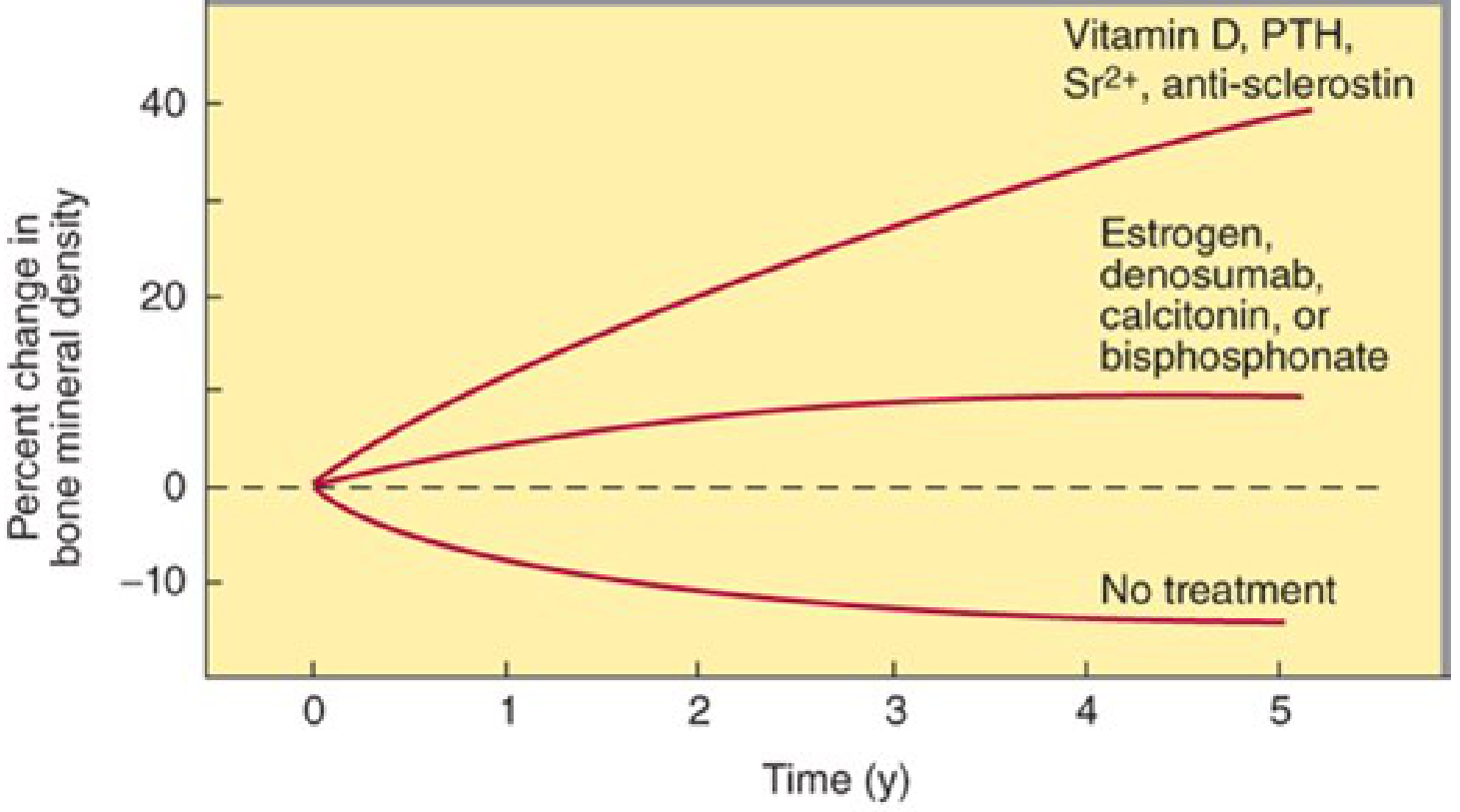
Key points from the graph:
- Antiresorptives (bisphosphonates, denosumab, calcitonin, estrogen) - produce a transient rise, then plateau as both formation and resorption equalize
- Anabolics / dual agents (Vitamin D, PTH/teriparatide, strontium, romosozumab/anti-sclerostin) - continue to increase BMD throughout the treatment period, achieving greater gains
- No treatment - continued bone loss over time
SECTION 15: SEQUENCE / COMBINATION THERAPY PRINCIPLES
From Katzung:
- Anabolic first, antiresorptive second - after teriparatide or abaloparatide, must follow with bisphosphonate/denosumab to preserve gains
- Romosozumab (1 year) → then antiresorptive agent
- Denosumab discontinuation → must switch to bisphosphonate (not just stop) to prevent rebound
- Bisphosphonate holiday - after 3-5 years, low-risk patients may pause; residual drug in bone provides continued effect
Quick ADR Summary Table
| Drug Class | Key ADRs |
|---|---|
| Bisphosphonates (oral) | Esophagitis, GI upset, atypical femoral fracture, ONJ |
| Bisphosphonates (IV) | Flu-like reaction, hypocalcemia, ONJ |
| Denosumab | Infections, hypocalcemia, rebound on withdrawal, ONJ, atypical fracture |
| Teriparatide/Abaloparatide | Hypercalcemia, orthostatic hypotension, osteosarcoma (rat data), injection site rxn |
| Romosozumab | MI/stroke risk (black box), arthralgias |
| Raloxifene | VTE, hot flashes, leg cramps |
| Estrogen | Breast cancer, endometrial cancer, VTE, stroke |
| Calcitonin | Rhinitis (nasal), nausea, flushing, malignancy risk (long-term) |
| Calcium supplements | Constipation, gas, bloating, drug interactions |
This teaching note draws directly from Katzung's Basic and Clinical Pharmacology, 16th Ed. (Chapter 42) and Lippincott Illustrated Reviews: Pharmacology (Chapter 27 - Drugs for Osteoporosis and Bone Remodeling Disorders). KDT (Kasaung-Dipiro-Talbert style classification) principles are reflected in the mechanism-based grouping used throughout.
This is a shared conversation. Sign in to Orris to start your own chat.