Cld
Chronic liver disease
Chronic Liver Disease (CLD) - Comprehensive Review
1. DEFINITION & OVERVIEW
2. ETIOLOGY (Causes)
| Category | Examples |
|---|---|
| Viral | Hepatitis B (HBV), Hepatitis C (HCV) |
| Alcohol | Alcoholic liver disease / Laennec's cirrhosis (10-20% of chronic alcoholics) |
| Metabolic | NAFLD/NASH (increasingly common), Wilson's disease, Hemochromatosis |
| Autoimmune | Autoimmune hepatitis, Primary biliary cholangitis (PBC), Primary sclerosing cholangitis (PSC) |
| Biliary | Chronic biliary obstruction, biliary cirrhosis |
| Drugs/Toxins | Methotrexate, amiodarone, isoniazid |
| Cryptogenic | Unknown etiology (~10-15%) |
| Vascular | Budd-Chiari syndrome, cardiac cirrhosis |
Key exam point: NASH has become the leading cause of cryptogenic cirrhosis; the process typically spans >20 years.
- Rosen's Emergency Medicine, p. 1247
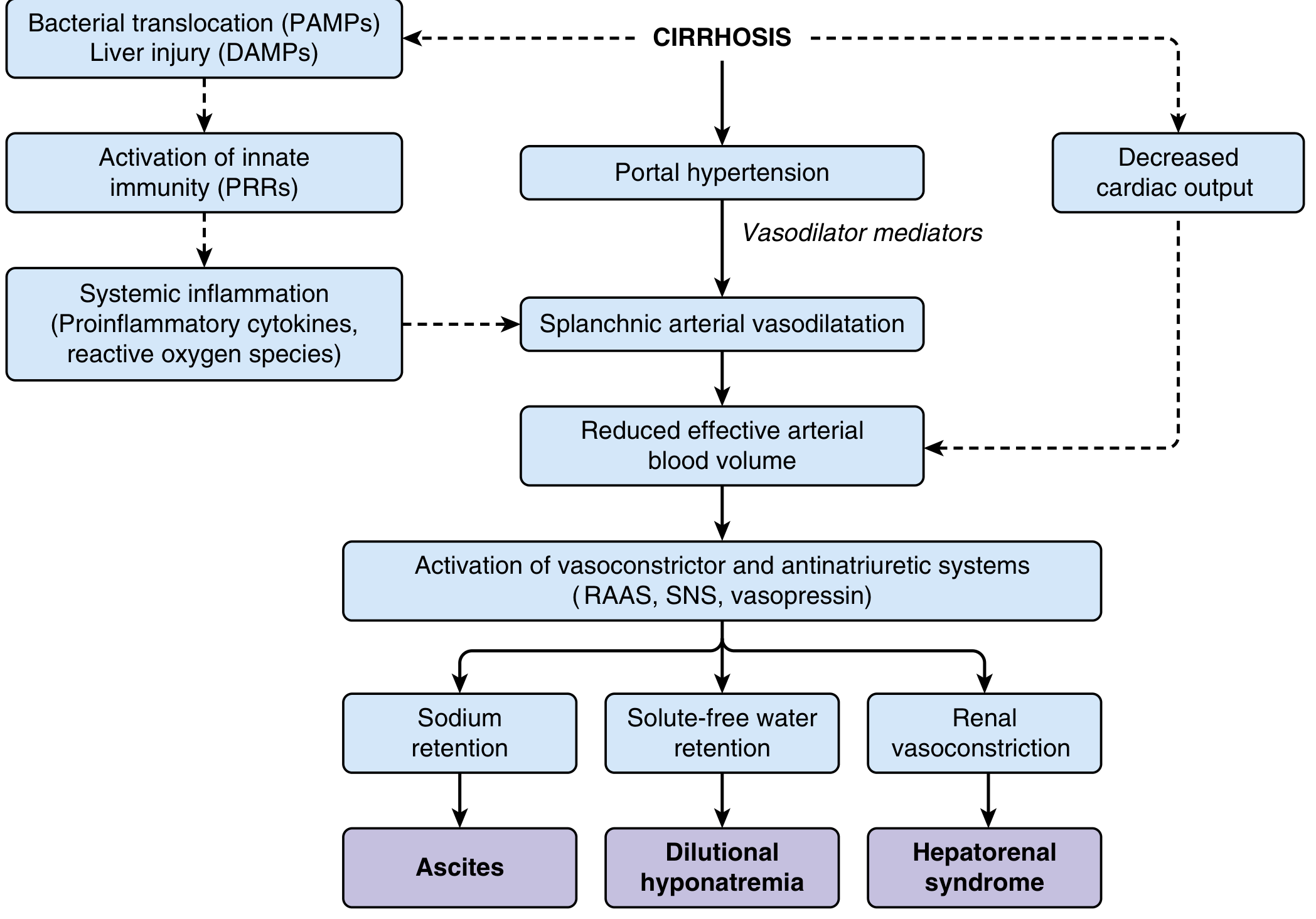
3. PATHOPHYSIOLOGY
- Loss of hepatocytes → impaired synthetic function (coagulopathy, hypoalbuminemia, jaundice)
- Fibrosis + nodules → distorted architecture → increased intrahepatic resistance → portal hypertension
- Portal hypertension → splanchnic vasodilation (mediated by nitric oxide and vasodilator substances)
- Splanchnic vasodilation → reduced effective arterial blood volume
- Compensatory activation of RAAS + SNS + vasopressin
- Consequences: Na retention → Ascites; Water retention → Dilutional hyponatremia; Renal vasoconstriction → HRS
4. CLINICAL FEATURES
Compensated vs. Decompensated
| Feature | Compensated | Decompensated |
|---|---|---|
| Symptoms | Often asymptomatic; fatigue, anorexia | Jaundice, ascites, encephalopathy, bleeding |
| 5-yr survival | ~80% | ~30% |
| Child-Pugh | Class A (5-6) | Class B/C (≥7) |
Physical Examination Signs
- Skin: Spider angiomata, palmar erythema, jaundice, ecchymosis, Dupuytren contracture
- Abdomen: Hepatomegaly or shrunken liver, splenomegaly, ascites, caput medusae (dilated abdominal veins)
- Endocrine/Metabolic: Gynecomastia, testicular atrophy, loss of body hair (in men)
- General: Muscle wasting, peripheral edema, leukonychia (white nails), clubbing
Biliary cirrhosis is distinctive: patients present with pruritus and jaundice before end-stage disease.
- Rosen's Emergency Medicine, p. 1247
5. INVESTIGATIONS
Blood Tests
| Test | Finding in CLD |
|---|---|
| AST/ALT | Mildly elevated (rarely >5x in cirrhosis) |
| Bilirubin | Elevated (late finding) |
| Albumin | Low (impaired synthesis) |
| PT/INR | Prolonged (coagulopathy) |
| Platelets | Low (hypersplenism) |
| BUN/Creatinine | Elevated (dehydration or HRS) |
| Alkaline phosphatase | Disproportionately elevated in biliary disease |
Imaging
- Ultrasound: Nodular liver surface, splenomegaly, ascites - first-line
- Transient elastography (FibroScan): Non-invasive staging of fibrosis; also predicts varices and liver-related death
- CT/MRI: Better characterization, HCC surveillance
Liver Biopsy
- Gold standard for confirming cirrhosis and grading fibrosis
- Limitations: sampling error, interobserver variability, procedure risk
- Increasingly replaced by non-invasive markers
6. SEVERITY SCORING SYSTEMS (HIGH-YIELD EXAM TOPIC)
Child-Pugh Score (5 parameters)
| Parameter | 1 point | 2 points | 3 points |
|---|---|---|---|
| Bilirubin (mg/dL) | <2 | 2-3 | >3 |
| Albumin (g/dL) | >3.5 | 2.8-3.5 | <2.8 |
| PT prolongation (sec) / INR | <4 / <1.7 | 4-6 / 1.7-2.3 | >6 / >2.3 |
| Ascites | None | Mild | Moderate-severe |
| Encephalopathy | None | Grade 1-2 | Grade 3-4 |
- Class A (5-6): Compensated; well-tolerated surgery
- Class B (7-9): Moderate risk
- Class C (≥10): Decompensated; surgery contraindicated; listed for transplant
MELD Score
- Formula: 3.78 × ln[Bilirubin] + 11.2 × ln[INR] + 9.57 × ln[Creatinine] + 6.43
- Now includes serum sodium (MELD-Na / MELD 3.0) for improved accuracy
- Used for organ allocation in liver transplant listing in the United States
- Higher score = higher short-term mortality
- Harrison's Principles, p. 814-821
7. COMPLICATIONS (The "Big 5")
7a. Ascites
- Most common complication; develops in ~60% within 10 years of compensated cirrhosis
- Pathogenesis: Na retention (RAAS activation) → extracellular fluid expansion → peritoneal accumulation
- Diagnosis: SAAG (Serum-Ascites Albumin Gradient)
- SAAG ≥1.1 g/dL = portal hypertension (cirrhosis, cardiac, Budd-Chiari)
- SAAG <1.1 = non-portal (TB, malignancy, pancreatitis)
| Grade | Management |
|---|---|
| Grade 1 (mild) | Sodium restriction (<2g/day), monitor |
| Grade 2 (moderate) | Spironolactone ± furosemide (100:40 ratio) |
| Grade 3 (tense) | Large-volume paracentesis (LVP) + albumin 8g/L drained |
| Refractory | Repeat LVP, TIPS (transjugular intrahepatic portosystemic shunt), transplant |
Key: Give albumin 8 g per litre when removing >5 L by paracentesis. ACE inhibitors and ARBs are contraindicated in decompensated cirrhosis with ascites.
- Rosen's Emergency Medicine, p. 2500-2506
7b. Spontaneous Bacterial Peritonitis (SBP)
- Acute infection of ascitic fluid WITHOUT a surgical source
- Common organisms: E. coli > Klebsiella > Streptococcus pneumoniae
- Diagnosis: Ascitic fluid PMN (neutrophil) count >250 cells/mm³
- Treatment: Cefotaxime 2 g IV q8h for 5 days + albumin 1.5 g/kg on day 1, 1 g/kg on day 3
- Prophylaxis: Norfloxacin or ciprofloxacin in high-risk patients
- Rosen's Emergency Medicine, p. 2524-2535
7c. Variceal Bleeding
- From gastroesophageal varices due to portal hypertension (portal pressure >12 mmHg)
- Mortality: 10-15% per episode of upper GI bleeding from varices
- Acute management:
- Resuscitate (platelets >50,000 for procedures)
- Vasoactive drugs: Octreotide/somatostatin (reduce splanchnic flow)
- Antibiotic prophylaxis: Ceftriaxone (reduces SBP risk post-bleed)
- Endoscopic band ligation (EBL) - treatment of choice
- Balloon tamponade (Sengstaken-Blakemore tube) - bridge only
- TIPS - for refractory bleeding
- Secondary prophylaxis: Non-selective beta-blockers (propranolol/nadolol) + EBL
- Coagulopathy note: Prefer cryoprecipitate (1 unit/10 kg) over FFP for active bleeding in liver disease
7d. Hepatic Encephalopathy (HE)
- Neuropsychiatric dysfunction from hyperammonemia + altered neurotransmission (GABA-BZ receptor upregulation)
- Pathogenesis: Reduced hepatocyte function + portosystemic shunting → ammonia bypasses liver → blood-brain barrier disruption
- Note: Ammonia levels do NOT directly correlate with severity
| Grade | Features |
|---|---|
| 0 (Minimal/Covert) | Subclinical; detected only on psychometric tests |
| 1 | Trivial lack of awareness, euphoria/anxiety, impaired attention |
| 2 | Lethargy, disorientation, inappropriate behavior, asterixis |
| 3 | Somnolence, confusion, asterixis, bizarre behavior |
| 4 | Coma |
- GI bleeding, hypokalemia, infection, dehydration, constipation, sedatives
- Correct precipitants
- Lactulose 30-60 g/day (acidifies colon, traps NH4+, promotes evacuation)
- Rifaximin 400 mg PO q8h (non-absorbed antibiotic, reduces ammonia production)
- Branched-chain amino acids (BCAA) as adjunct
- Liver transplant is the definitive cure
HE develops in 50-70% of cirrhotic patients; 1-year survival without transplant is ~42%, 3-year ~23%
- Sleisenger & Fordtran's, p. 1815
7e. Hepatorenal Syndrome (HRS)
- Functional renal failure (no intrinsic renal disease) due to severe renal vasoconstriction in advanced cirrhosis
- Diagnostic criteria: Rising creatinine in liver failure + oliguria (<400 mL/day) + urine Na <10 mEq/L + no improvement after 2 days of diuretic withdrawal and albumin loading
| Type | Feature |
|---|---|
| HRS-AKI (formerly Type 1) | Rapid doubling of creatinine in <2 weeks; poor prognosis |
| HRS-CKD (formerly Type 2) | Gradual decline; associated with refractory ascites |
- Bridge therapy: Vasoconstrictors + albumin
- Terlipressin (vasopressin analogue) - most evidence
- Norepinephrine - equivalent efficacy
- Octreotide + midodrine combination
- TIPS
- Extracorporeal albumin dialysis (MARS)
- Definitive: Liver transplantation (reverses HRS)
- Goldman-Cecil Medicine; Harrison's Principles, p. 2221-2224
8. OTHER COMPLICATIONS
| Complication | Key Point |
|---|---|
| Hepatocellular carcinoma (HCC) | 6-monthly US ± AFP screening in all cirrhotics |
| Hepatopulmonary syndrome | Intrapulmonary shunting → hypoxia; platypnoea-orthodeoxia |
| Portopulmonary hypertension | Pulmonary arterial HTN; rules out transplant if severe |
| Hepatic hydrothorax | Right-sided pleural effusion (portal hypertension); fluid from peritoneum via diaphragmatic defect |
| Coagulopathy | Low platelets (hypersplenism) + low clotting factors + low fibrinogen |
| Hypersplenism | Thrombocytopenia, leukopenia, anemia |
| Hyponatremia | Dilutional; water restriction + V2 receptor antagonists (tolvaptan) |
| Osteoporosis | Especially in PBC/PSC; calcium + vitamin D supplementation |
9. MANAGEMENT OVERVIEW
General Principles
- Treat the underlying cause (antivirals for HBV/HCV, abstinence for alcohol, immunosuppression for AIH)
- Alcohol: strict abstinence for all patients
- Vaccinations: Hep A, Hep B, pneumococcal, annual influenza
- Avoid hepatotoxic drugs and NSAIDs (worsen renal function in cirrhosis)
- Regular surveillance: 6-monthly liver ultrasound for HCC; upper endoscopy at diagnosis to assess varices
Liver Transplantation
- Indication: Child-Pugh class B (score ≥7) or MELD ≥15, or major complication (HCC within Milan criteria, HRS, refractory ascites)
- Child-Pugh class C - surgery is otherwise contraindicated
- HBV cirrhosis: Long-term TDF/TAF/entecavir → can achieve cirrhosis regression in 75% at 5 years
10. HIGH-YIELD EXAM MNEMONICS
- Alcohol
- Biliary disease (PBC, PSC)
- Chronics - Viral hepatitis C, Cryptogenic
- Drugs/metabolic (NAFLD, Wilson's, Hemochromatosis)
- Etc. - Autoimmune hepatitis, Budd-Chiari
- Bilirubin
- Encephalopathy
- Albumin
- PT/INR
- Tension ascites
- GI bleeding
- Infection (SBP)
- Bowel obstruction/constipation
- Alcohol binge
- Drugs (sedatives, opioids, diuretics)
- Sodium and electrolyte disturbance (hypokalemia)
Causes of hepatomegaly
Causes of Hepatomegaly
Exam tip: The liver can feel hard and irregular (cirrhosis), tender and smooth (acute hepatitis, hepatic congestion from RHF), or nodular with bruit (HCC). The texture and tenderness give you the diagnosis.
- Goldman-Cecil Medicine, p. 1543-1544
Classification by Mechanism
1. INFLAMMATORY / INFECTIVE
| Cause | Notes |
|---|---|
| Acute viral hepatitis (A, B, C, D, E) | Tender, smooth, enlarged; "starry sky" on USS |
| Chronic viral hepatitis (B, C) | Coarsened echotexture on USS |
| Alcoholic hepatitis | Tender hepatomegaly; AST:ALT >2:1 |
| Infectious mononucleosis (EBV) | Young patients; splenomegaly + pharyngitis |
| Cytomegalovirus (CMV) | Especially in immunocompromised |
| Amoebic liver abscess | Tender, smooth; right lobe most affected |
| Pyogenic liver abscess | Marked tenderness; swinging fever |
| Hydatid disease (Echinococcus) | Cystic lesion; travel history |
| Malaria (Plasmodium) | Tropical; + splenomegaly |
| Schistosomiasis | Tropical; portal fibrosis, pipestem fibrosis |
| Leptospirosis | Weil's disease; jaundice + renal failure |
| Tuberculosis (miliary/hepatic) | Systemic infiltration; granulomas |
| Visceral leishmaniasis (Kala-azar) | Massive hepatosplenomegaly |
| Brucellosis | Animal contact; granulomatous hepatitis |
2. CONGESTIVE / VASCULAR
| Cause | Notes |
|---|---|
| Right heart failure (RHF) | Tender, pulsatile; elevated JVP; hepatojugular reflux |
| Constrictive pericarditis | Firm liver; Kussmaul sign; "nutmeg liver" on histology |
| Tricuspid regurgitation | Pulsatile hepatomegaly - characteristic finding |
| Budd-Chiari syndrome | Hepatic vein obstruction; ascites + tender hepatomegaly; caudate lobe hypertrophy |
| Inferior vena cava obstruction | Venous congestion |
| Sinusoidal obstruction syndrome (SOS) | Post-bone marrow transplant; tender hepatomegaly + jaundice + fluid retention |
Pulsatile hepatomegaly = tricuspid regurgitation until proven otherwise.
3. INFILTRATIVE
| Cause | Notes |
|---|---|
| Fatty liver (NAFLD/NASH) | Most common; diffuse increased echogenicity on USS |
| Alcoholic fatty liver | Reversible; large, smooth, tender liver |
| Amyloidosis | Firm, non-tender; "waxy" consistency |
| Sarcoidosis | Granulomas; + lymphadenopathy, lung involvement |
| Haemochromatosis | Iron overload; "bronze diabetes"; hepatomegaly + cirrhosis |
| Wilson's disease | Copper deposition; K-F rings; young patients |
| Glycogen storage diseases (GSD I - Von Gierke's) | Enlarged hepatocytes with pale cytoplasm; presents in infancy with hypoglycemia |
| Gaucher's disease | Lipid storage; glucocerebrosidase deficiency |
| Niemann-Pick disease | Sphingomyelin storage |
| α-1 antitrypsin deficiency | PAS+ inclusions in hepatocytes |
4. NEOPLASTIC / SPACE-OCCUPYING
| Cause | Notes |
|---|---|
| Hepatocellular carcinoma (HCC) | Arterial bruit; ↑ AFP; background cirrhosis |
| Metastatic carcinoma | Most common malignant cause; hard, nodular, knobbly; from colorectal, breast, lung, stomach, pancreas |
| Cholangiocarcinoma | Jaundice + hepatomegaly |
| Hepatic lymphoma | Primary or secondary; homogeneous enlargement |
| Hepatic haemangioma | Benign; most common benign liver tumour; no bruit |
| Hepatic adenoma | OCP use; risk of rupture |
| Focal nodular hyperplasia (FNH) | Central stellate scar on CT/MRI |
| Hepatic cysts | Simple cysts - incidental; polycystic liver disease |
| Leukaemia / lymphoma | Infiltration of liver; + lymphadenopathy, splenomegaly |
5. CHOLESTATIC / BILIARY
| Cause | Notes |
|---|---|
| Biliary tract obstruction (extrahepatic) | Dilated ducts on USS; ↑ ALP, bilirubin; pruritus |
| Primary biliary cholangitis (PBC) | Middle-aged women; anti-mitochondrial antibodies (AMA) |
| Primary sclerosing cholangitis (PSC) | Associated with IBD; MRCP: "beading" of bile ducts |
6. CIRRHOSIS
- Early/active cirrhosis → enlarged liver
- End-stage cirrhosis → shrunken, fibrosed liver (right lobe atrophies, caudate/left lobe hypertrophy)
- Nodular surface on ultrasound
Clinical Approach: Texture of the Liver (Exam Favourite)
| Texture | Likely Cause |
|---|---|
| Soft, tender, smooth | Acute hepatitis, RHF/congestion, abscess |
| Smooth, non-tender | Fatty liver, early cirrhosis, leukaemia |
| Firm, irregular, nodular | Cirrhosis, metastases |
| Hard, rock-hard nodular | Metastatic malignancy |
| Pulsatile | Tricuspid regurgitation |
Diagnostic Approach - Algorithm
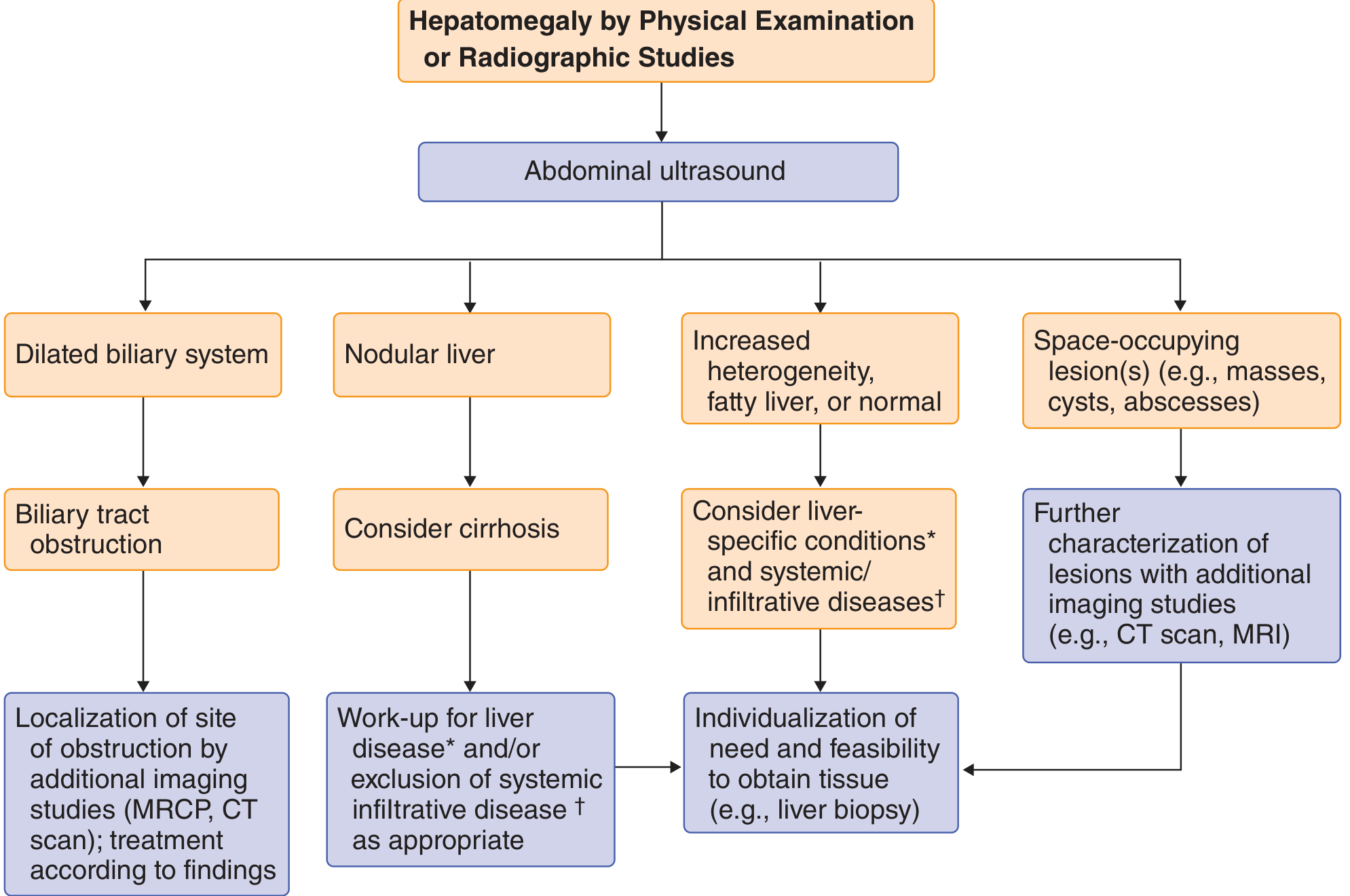
- Ultrasound abdomen - first-line
- Dilated biliary system → biliary obstruction → MRCP/CT
- Nodular liver → consider cirrhosis → liver-specific workup
- Increased heterogenicity / fatty liver → liver-specific conditions (hepatitis, NAFLD, NASH, autoimmune, metabolic) ± systemic/infiltrative diseases (amyloid, lymphoma, sarcoidosis, TB)
- Space-occupying lesions (masses, cysts, abscesses) → CT/MRI for characterisation
- Blood tests: LFTs, viral hepatitis serology, AFP, autoimmune markers, ferritin, ceruloplasmin
- Liver biopsy - if diagnosis unclear after imaging
High-Yield Exam Mnemonics
- Infections (hepatitis, abscess, malaria, amoeba)
- Neoplasia (HCC, mets, lymphoma)
- Vascular (RHF, Budd-Chiari, TR)
- Infiltrative (fatty liver, amyloid, sarcoid, GSD)
- Toxic/alcohol
- Endocrine/metabolic (DM, haemochromatosis, Wilson's)
- Drugs
- Malignancy (primary + secondary)
- Ducts (biliary obstruction)
- Storage diseases (Gaucher, Niemann-Pick)
Causes of hepatomegaly
Causes of Hepatomegaly - Quick Reference
By Mechanism (6 Groups)
| Category | Key Examples |
|---|---|
| 1. Inflammatory / Infective | Viral hepatitis (A-E), amoebic/pyogenic abscess, malaria, EBV, TB, kala-azar, schistosomiasis |
| 2. Congestive / Vascular | Right heart failure, tricuspid regurgitation (pulsatile!), Budd-Chiari syndrome, constrictive pericarditis |
| 3. Infiltrative | NAFLD/fatty liver, amyloidosis, sarcoidosis, haemochromatosis, Wilson's, glycogen storage diseases |
| 4. Neoplastic | HCC, metastases (most common malignant cause), lymphoma, haemangioma, hepatic adenoma |
| 5. Cholestatic / Biliary | Biliary obstruction, PBC, PSC |
| 6. Cirrhosis | Early/active cirrhosis (enlarged) - late cirrhosis gives a shrunken liver |
Texture Clue (Exam Favourite)
| Feel | Think |
|---|---|
| Soft, smooth, tender | Acute hepatitis, RHF, abscess |
| Smooth, non-tender | Fatty liver, leukaemia, amyloid |
| Firm, nodular | Cirrhosis, metastases |
| Rock-hard nodular | Metastatic malignancy |
| Pulsatile | Tricuspid regurgitation |
Mnemonic - "INVITED MDs"
Diagnostic Approach
- Ultrasound first - guides everything
- Dilated ducts → biliary obstruction → MRCP/CT
- Nodular → cirrhosis workup
- Fatty/heterogeneous → hepatitis panel, metabolic screen
- Mass/cyst/abscess → CT/MRI for characterisation
- Labs: LFTs, viral serology, AFP, AMA, ANA, ferritin, ceruloplasmin
- Liver biopsy if diagnosis remains unclear
Splenomegaly
Splenomegaly - Comprehensive Review
Functions of the Spleen (Context for Causes)
- Work hypertrophy - increased filtering/phagocytic demand (infection, haemolysis)
- Congestion - impaired venous drainage (portal hypertension, cardiac failure)
- Infiltration - abnormal cells/deposits (malignancy, storage diseases)
- Immunological hyperactivity - antigen stimulation (autoimmune, infection)
Classification of Causes
1. INFECTIVE / INFLAMMATORY
| Sub-category | Examples |
|---|---|
| Viral | Infectious mononucleosis (EBV) - most common viral cause; CMV; HIV; viral hepatitis |
| Bacterial | Infective endocarditis, typhoid fever, brucellosis, syphilis, TB, rickettsial (Rocky Mountain spotted fever), leptospirosis |
| Parasitic | Malaria (nearly always causes splenomegaly), kala-azar (visceral leishmaniasis) - causes massive splenomegaly, schistosomiasis, trypanosomiasis, toxoplasmosis, echinococcosis |
| Fungal | Histoplasmosis, disseminated cryptococcosis |
| Splenic abscess | From endocarditis emboli, typhoid, osteomyelitis, pancreatic necrosis |
Geography and travel history are key clues - malaria and kala-azar dominate in the tropics.
- Goldman-Cecil Medicine, p. 1435
2. CONGESTIVE / VASCULAR
| Cause | Notes |
|---|---|
| Cirrhosis of the liver | Main cause of massive congestive splenomegaly; portal hypertension |
| Portal vein thrombosis | Direct compression/obstruction of portal flow |
| Splenic vein thrombosis | Left-sided (sinistral) portal hypertension |
| Right heart failure | Systemic venous congestion; moderately enlarged spleen (rarely >500g) |
| Constrictive pericarditis | Venous backpressure |
| Tricuspid valve disease / cor pulmonale | Right-sided congestion |
| Budd-Chiari syndrome | Hepatic vein obstruction → portal hypertension |
| Schistosomiasis | "Pipestem" hepatic fibrosis → portal hypertension |
Cirrhosis is the most common cause of congestive splenomegaly. A palpable spleen tip in chronic liver disease implies portal hypertension.
- Robbins & Cotran Pathologic Basis of Disease
3. HAEMATOLOGICAL
Haemolytic Anaemias
| Cause | Notes |
|---|---|
| Hereditary spherocytosis | Autosomal dominant; spleen destroys spherocytes |
| Autoimmune haemolytic anaemia (AIHA) | Antibody-coated RBCs phagocytosed by splenic macrophages |
| Haemoglobinopathies | Sickle cell (early - later autosplenectomy), thalassaemia major |
| G6PD deficiency | Episodic haemolysis |
Myeloproliferative Neoplasms (causes massive splenomegaly)
| Cause | Notes |
|---|---|
| Primary myelofibrosis | Massive splenomegaly from extramedullary haematopoiesis; leukoerythroblastic blood film |
| Chronic myeloid leukaemia (CML) | Hallmark is massive splenomegaly; Philadelphia chromosome |
| Polycythaemia vera | Splenomegaly from extramedullary haematopoiesis |
| Essential thrombocythaemia | Moderate splenomegaly |
Lymphoproliferative Disorders
| Cause | Notes |
|---|---|
| Lymphoma (Hodgkin & Non-Hodgkin) | ± lymphadenopathy |
| Hairy cell leukaemia | Isolated splenomegaly WITHOUT lymphadenopathy - characteristic |
| Chronic lymphocytic leukaemia (CLL) | + lymphadenopathy |
| Acute leukaemias | Variable |
4. AUTOIMMUNE / IMMUNE-MEDIATED
| Cause | Notes |
|---|---|
| Rheumatoid arthritis | Mild-moderate; Felty syndrome = RA + splenomegaly + neutropenia |
| SLE | Autoimmune activation |
| ITP | Spleen seldom palpable despite destroying platelets |
| Drug reaction | Phenytoin, antibiotics (serum sickness) |
5. INFILTRATIVE / STORAGE DISEASES
| Cause | Notes |
|---|---|
| Gaucher's disease | Most common storage disease; glucocerebrosidase deficiency; bone crises |
| Niemann-Pick disease | Sphingomyelinase deficiency |
| Amyloidosis | Firm, non-tender splenomegaly |
| Sarcoidosis | Granulomatous infiltration; + hilar lymphadenopathy |
| Haemochromatosis | Iron deposition (usually secondary to cirrhosis) |
| Extramedullary haematopoiesis | Bone marrow failure/fibrosis |
6. OTHER
| Cause | Notes |
|---|---|
| Thyrotoxicosis | Mild, uncommon |
| Haemophagocytic lymphohistiocytosis (HLH) | Severe systemic inflammatory syndrome; fever + cytopenias + splenomegaly |
| Splenic cysts/pseudocysts | Benign; incidental |
| Metastatic malignancy | Rare; melanoma is the most likely solid tumour to metastasise to spleen |
MASSIVE Splenomegaly - Causes to Know (High-Yield)
| Mnemonic: "MMCH KG" |
|---|
| Myelofibrosis (primary) |
| Malaria (chronic) |
| CML (chronic myeloid leukaemia) |
| Hairy cell leukaemia |
| Kala-azar (visceral leishmaniasis) |
| Gaucher's disease |
Hypersplenism
- Splenomegaly
- One or more peripheral cytopenias (anaemia, leukopenia, thrombocytopenia)
- Normal or hypercellular bone marrow (compensating)
- Improvement after splenectomy
- 90% of peripheral platelets
- 65% of granulocytes
- 30% of red blood cells
When hypersplenism is the sole driver of cytopenias, splenectomy is often curative.
- Frameworks for Internal Medicine, p. 336
Clinical Assessment
Symptoms
- Usually asymptomatic (incidental finding on imaging)
- Left upper quadrant dragging discomfort / pain radiating to left shoulder (infarct)
- Early satiety (gastric compression)
- Cytopenias: fatigue, bleeding, infections
- Rarely: catastrophic splenic rupture (can be first sign with EBV!)
Examination Technique
- Position patient in right lateral decubitus with knees flexed
- Begin palpation from the right iliac fossa (to avoid missing massive spleen)
- Spleen descends on deep inspiration toward right iliac fossa
- Notch on medial border is pathognomonic
- Record in cm below left costal margin in midclavicular line
Key Differentiating Features of Spleen vs. Kidney
| Feature | Spleen | Kidney |
|---|---|---|
| Moves with respiration | Yes - downward & medially | Minimally |
| Ballottable | No | Yes |
| Can get above it | No | Sometimes |
| Notch on medial border | Yes | No |
| Band of colonic resonance | No (dull to percussion) | Yes |
Diagnostic Approach
- History: Age, travel history (tropical), drug history, family history
- Examination: Size of spleen, lymphadenopathy, hepatomegaly, jaundice, fever
- FBC + blood film: Cytopenias, abnormal cells, parasites (malaria film)
- LFTs, viral serology: EBV (Monospot/Paul-Bunnell), hepatitis screen
- Ultrasound: Confirms size, portal vein Doppler (portal HTN), lesions
- CT abdomen: Better anatomical detail, lymphadenopathy
- Bone marrow biopsy: If haematological malignancy suspected
- Splenic biopsy: Rarely needed; risk of haemorrhage
Complications of Splenomegaly
| Complication | Notes |
|---|---|
| Hypersplenism | Pancytopenia from sequestration |
| Splenic infarct | Pain; sickle cell, endocarditis, myeloproliferative |
| Splenic rupture | Spontaneous or traumatic; EBV classic cause |
| Splenic abscess | From septic emboli or haematogenous spread |
Causes of hepatosplenomegaly.
Causes of Hepatosplenomegaly
A palpable spleen tip in chronic liver disease implies portal hypertension. Fever + hepatosplenomegaly suggests systemic infection (EBV, malaria, visceral leishmaniasis), granulomatous disease (TB, histoplasmosis), or lymphoma.
- Goldman-Cecil Medicine, p. 2941
Classification by Cause
1. INFECTIVE (Most Common Group)
| Cause | Key Features |
|---|---|
| Infectious mononucleosis (EBV) | Classic triad: pharyngitis + lymphadenopathy + hepatosplenomegaly; young adults; Monospot +ve; rash with amoxicillin |
| CMV | Heterophil-negative mono syndrome; immunocompromised |
| Malaria | Nearly always causes hepatosplenomegaly; travel history; Plasmodium vivax most commonly; periodic fever |
| Visceral leishmaniasis (Kala-azar) | Massive hepatosplenomegaly; months of fever, weight loss, anaemia; sub-Saharan Africa, Indian subcontinent |
| Typhoid fever | Salmonella typhi; rose spots; relative bradycardia |
| Brucellosis | Animal contact; undulant fever; lymphadenopathy; malodorous perspiration; hallmark feature |
| Tuberculosis (miliary) | Systemic dissemination; granulomas in both organs |
| Schistosomiasis | Portal fibrosis ("pipestem" fibrosis) → portal HTN; tropical |
| Syphilis (secondary) | Spirochaetaemia; rash including palms & soles |
| Leptospirosis | Animal urine exposure; Weil's disease: jaundice + renal failure + hepatosplenomegaly |
| Infective endocarditis | Septic emboli; immunological activation |
| Histoplasmosis | Fungal; immunocompromised; bird/bat droppings |
| Toxoplasmosis | Intracellular parasite; immunocompromised |
| Trypanosomiasis | African sleeping sickness; tsetse fly |
| HIV | Often due to co-infection (hepatitis C, CMV, MAC) |
| Viral hepatitis (A, B, C, E) | Active hepatitis with systemic immune activation |
2. PORTAL HYPERTENSION / CONGESTIVE
| Cause | Key Features |
|---|---|
| Cirrhosis of the liver | Most common overall cause; portal HTN → splenomegaly; early cirrhosis enlarges liver; late = shrunken liver |
| Schistosomiasis | Pipestem fibrosis → portal hypertension; both organs enlarged |
| Right heart failure | Congestive hepatomegaly + passive splenic congestion |
| Constrictive pericarditis | Elevated JVP; Kussmaul sign |
| Budd-Chiari syndrome | Hepatic vein thrombosis; caudate lobe hypertrophy; + ascites |
| Portal / splenic vein thrombosis | Localised portal hypertension |
3. HAEMATOLOGICAL MALIGNANCIES
| Cause | Key Features |
|---|---|
| Lymphoma (Hodgkin & NHL) | Hepatosplenomegaly ± generalised lymphadenopathy; B symptoms (fever, night sweats, weight loss) |
| Leukaemia (CML, CLL, ALL, AML) | CML: massive hepatosplenomegaly; Philadelphia chromosome (t9;22) |
| Primary myelofibrosis | Massive splenomegaly (extramedullary haematopoiesis); leukoerythroblastic film; teardrop cells |
| Polycythaemia vera | Plethora; pruritis after bath; elevated Hb/Hct |
4. INFILTRATIVE / STORAGE DISEASES
| Cause | Key Features |
|---|---|
| Gaucher's disease | Most common lysosomal storage disorder; glucocerebrosidase deficiency; marked hepatosplenomegaly + bone crises; "wrinkled tissue paper" macrophages |
| Niemann-Pick disease | Sphingomyelinase deficiency; Type A: severe neonatal form with hepatosplenomegaly by 3 months |
| Amyloidosis | Firm, smooth, non-tender; AL or AA types; Congo red staining |
| Sarcoidosis | Non-caseating granulomas in liver + spleen; hilar lymphadenopathy; elevated ACE |
| Haemochromatosis | Iron overload; hepatomegaly + cirrhosis; spleen enlarged secondary to portal HTN |
| Glycogen storage diseases (von Gierke - GSD I) | Infants; hypoglycaemia + massive hepatomegaly; splenomegaly present |
| Hurler syndrome (MPS I) | Mucopolysaccharidosis; children; coarse facies + organomegaly |
5. AUTOIMMUNE / INFLAMMATORY
| Cause | Key Features |
|---|---|
| Systemic lupus erythematosus (SLE) | Multi-system; ANA +ve; lupus hepatitis |
| Rheumatoid arthritis / Felty syndrome | RA + splenomegaly + neutropenia; hepatomegaly from Felty's or co-pathology |
| Still's disease (SJIA) | Fever + rash + lymphadenopathy + hepatosplenomegaly; serositis; very high ferritin; macrophage activation syndrome |
| Haemophagocytic lymphohistiocytosis (HLH) | Cytokine storm; fever + hepatosplenomegaly + cytopenias + very high ferritin (>10,000); triggered by EBV or malignancy |
6. MISCELLANEOUS
| Cause | Key Features |
|---|---|
| Thyrotoxicosis | Mild; warm, tender goitre |
| Chronic myeloid conditions (extramedullary haematopoiesis) | Bone marrow failure states |
| Wilson's disease | Copper overload; K-F rings; young patient |
| α-1 antitrypsin deficiency | Liver disease (PAS+ inclusions) + emphysema |
Exam Summary Table: Key Distinguishing Features
| Cause | Key Associated Feature |
|---|---|
| EBV | Young, pharyngitis, posterior cervical lymphadenopathy, rash with amoxicillin |
| Malaria | Travel, cyclical fever, anaemia, thrombocytopenia |
| Kala-azar | Tropical, months of fever, massive splenomegaly > hepatomegaly, anaemia, hypergammaglobulinaemia |
| Cirrhosis | Spider naevi, caput medusae, ascites, jaundice |
| CML | Massive splenomegaly, Philadelphia chromosome, basophilia |
| Lymphoma | B symptoms, lymphadenopathy, elevated LDH |
| Gaucher's | Bone pain/crises, Ashkenazi Jewish heritage, no neurological symptoms (type 1) |
| Sarcoidosis | Bilateral hilar lymphadenopathy on CXR, elevated ACE, erythema nodosum |
| Brucellosis | Animal contact, undulant fever, malodorous sweating |
| HLH | Very high ferritin >10,000, cytopenias, triggered by EBV or haematological malignancy |
| Still's disease | Quotidian salmon-coloured rash, arthritis, serositis, high ferritin |
Mnemonic: "I CLAIM SHE"
- I - Infections (EBV, malaria, kala-azar, typhoid, TB, brucellosis)
- C - Cirrhosis / portal hypertension
- L - Leukaemia & lymphoma
- A - Amyloid / Autoimmune (SLE, RA, Still's, HLH)
- I - Infiltrative (sarcoidosis, Gaucher's, Niemann-Pick)
- M - Myeloproliferative disorders (CML, myelofibrosis, PV)
- S - Storage diseases (glycogen, mucopolysaccharidoses)
- H - Heart failure (right-sided congestive)
- E - Endocrine/metabolic (haemochromatosis, Wilson's, thyrotoxicosis)
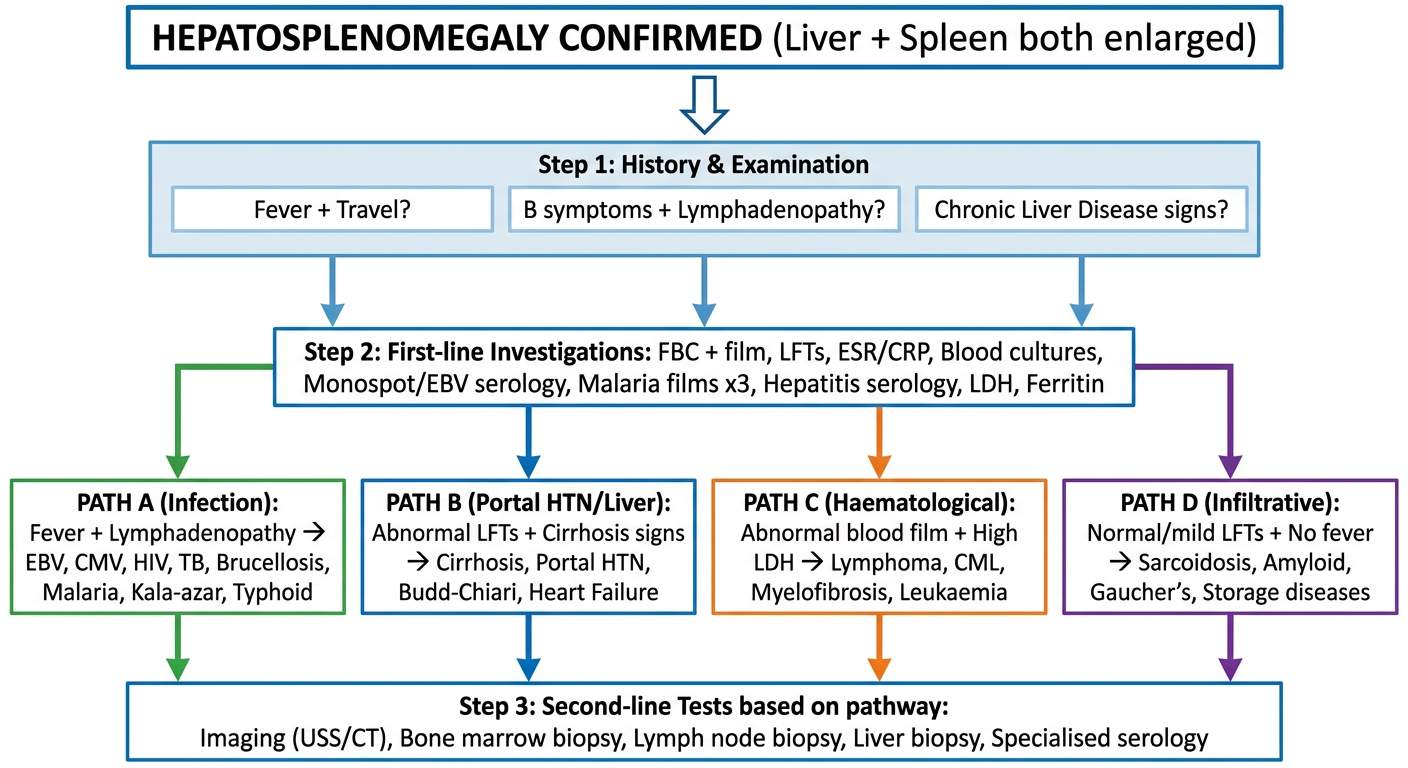
Create a diagnostic flowchart or comparison table for hepatosplenomegaly workup
A detailed medical diagnostic flowchart for hepatosplenomegaly workup. The flowchart starts at the top with "HEPATOSPLENOMEGALY CONFIRMED (Liver + Spleen both enlarged)" in a bold header box. It branches into two main paths: "Step 1: History & Examination" and flows down through investigations. The chart has these sequential steps: 1. Top box: "HEPATOSPLENOMEGALY" 2. Second level: Three parallel boxes for key history clues: "Fever + Travel?" | "B symptoms + Lymphadenopathy?" | "Chronic Liver Disease signs?" 3. Each of those branches to initial investigations box: "Step 2: First-line Investigations: FBC + film, LFTs, ESR/CRP, Blood cultures, Monospot/EBV serology, Malaria films x3, Hepatitis serology, LDH, Ferritin" 4. Results branch into 4 diagnostic pathways: - PATH A (Infection): "Fever + Lymphadenopathy → EBV, CMV, HIV, TB, Brucellosis, Malaria, Kala-azar, Typhoid" in green - PATH B (Portal HTN/Liver): "Abnormal LFTs + Cirrhosis signs → Cirrhosis, Portal HTN, Budd-Chiari, Heart Failure" in blue - PATH C (Haematological): "Abnormal blood film + High LDH → Lymphoma, CML, Myelofibrosis, Leukaemia" in orange - PATH D (Infiltrative): "Normal/mild LFTs + No fever → Sarcoidosis, Amyloid, Gaucher's, Storage diseases" in purple 5. Final box at bottom: "Step 3: Second-line Tests based on pathway: Imaging (USS/CT), Bone marrow biopsy, Lymph node biopsy, Liver biopsy, Specialised serology" Clean professional medical illustration, white background, color-coded pathways, clear arrows, sans-serif font, suitable for medical students and clinical exam preparation.
Hepatosplenomegaly Workup - Comparison Table
Step 1: History Clues That Guide the Diagnosis
| Clue | Think |
|---|---|
| Fever + travel to tropics | Malaria, kala-azar, schistosomiasis, typhoid |
| Fever + pharyngitis + young patient | EBV (infectious mononucleosis) |
| Fever + months of weight loss | TB, lymphoma, kala-azar, HIV |
| B symptoms + lymphadenopathy | Lymphoma (Hodgkin / NHL) |
| Jaundice + spider naevi + ascites | Cirrhosis with portal hypertension |
| Animal/farm contact + undulant fever | Brucellosis |
| Bone pain + Ashkenazi Jewish | Gaucher's disease |
| Child + coarse facies + developmental delay | Mucopolysaccharidosis (Hurler) |
| Arthritis + quotidian rash + very high ferritin | Still's disease / HLH |
| Rash on palms and soles | Secondary syphilis |
Step 2: First-Line Investigations (Order in ALL patients)
| Test | What it detects |
|---|---|
| FBC + blood film | Anaemia, cytopenias, blast cells, malaria parasites, atypical lymphocytes (EBV) |
| LFTs (AST/ALT/ALP/bilirubin/albumin) | Hepatocellular vs cholestatic pattern; synthetic function |
| ESR / CRP | Non-specific inflammation |
| Monospot (Paul-Bunnell) + EBV serology | Infectious mononucleosis |
| Malaria thick & thin films x3 | If any travel history |
| Hepatitis A/B/C/E serology | Viral hepatitis |
| LDH | Haemolysis, lymphoma, leukaemia |
| Ferritin | Very high (>10,000) in HLH; elevated in haemochromatosis, inflammation |
| Blood cultures x3 | Bacterial sepsis, brucellosis, typhoid, endocarditis |
| Abdominal ultrasound + Doppler | Confirms organomegaly; portal vein flow; ascites; masses; lymph nodes |
Step 3: Pathway-Based Second-Line Tests
| Pathway | Pattern | Second-Line Tests | Likely Diagnoses |
|---|---|---|---|
| A - Infective | Fever + elevated WBC/CRP + lymphadenopathy | EBV VCA IgM/IgG; CMV PCR; HIV viral load; Blood cultures; Brucella serology; Widal test; Leishmania rK39 antigen; Splenic aspirate for Leishmania | EBV, CMV, HIV, typhoid, brucellosis, kala-azar, malaria, TB |
| B - Portal HTN / Liver | Abnormal LFTs + cirrhosis signs + ascites | Hepatitis serology; INR/PT; Albumin; Liver USS with Doppler; CT abdomen; Liver biopsy; SAAG on ascitic fluid | Cirrhosis, Budd-Chiari, cardiac failure, schistosomiasis |
| C - Haematological | Abnormal blood film + high LDH + lymphadenopathy | CT chest/abdomen/pelvis; Bone marrow biopsy; Lymph node biopsy; BCR-ABL (CML); JAK2 mutation (PV/MF); Flow cytometry | CML, lymphoma, myelofibrosis, leukaemia, hairy cell leukaemia |
| D - Infiltrative / Storage | No/mild fever, minimal LFT derangement, no lymphadenopathy | Serum ACE (sarcoidosis); β-glucocerebrosidase (Gaucher's); Serum protein electrophoresis + Congo red biopsy (amyloid); Ceruloplasmin (Wilson's); Ferritin + HFE gene (haemochromatosis) | Gaucher's, sarcoidosis, amyloid, haemochromatosis, Wilson's |
| E - Autoimmune/Inflammatory | Young patient + arthritis + very high ferritin + rash | ANA, anti-dsDNA (SLE); RF, anti-CCP (RA/Felty); Ferritin >10,000 + triglycerides + fibrinogen (HLH); Bone marrow biopsy (haemophagocytosis) | SLE, Still's disease, HLH, Felty syndrome |
Quick Pattern Recognition (Exam Shortcuts)
| Pattern | Diagnosis |
|---|---|
| Fever + pharyngitis + posterior cervical LN + hepatosplenomegaly + atypical lymphocytes | EBV mononucleosis |
| Months of fever + massive hepatosplenomegaly + anaemia + weight loss (tropics) | Kala-azar |
| Massive splenomegaly > hepatomegaly + basophilia + Philadelphia chromosome | CML |
| B symptoms + mediastinal widening on CXR + hepatosplenomegaly | Hodgkin lymphoma |
| Child + bone crises + hepatosplenomegaly + no neurological features | Gaucher's disease (Type 1) |
| Ferritin >10,000 + cytopenias + fever + hepatosplenomegaly | HLH |
| Ascites + caput medusae + spider naevi + hepatosplenomegaly | Cirrhosis / Portal HTN |
| Bilateral hilar lymphadenopathy + hepatosplenomegaly + elevated ACE | Sarcoidosis |
| Quotidian salmon rash + arthritis + hepatosplenomegaly + serositis | Still's disease |
History I should ask for an per abdomen case
History for a Per Abdomen Case
1. PRESENTING COMPLAINT (PC)
- Abdominal pain / swelling / distension
- Jaundice
- Vomiting / nausea
- Change in bowel habits
- Loss of weight / appetite
- Bleeding (haematemesis, malena, rectal bleeding)
2. HISTORY OF PRESENTING COMPLAINT (HPC)
For Abdominal Pain - Use "SOCRATES"
| Letter | Question |
|---|---|
| S - Site | "Where exactly is the pain?" (point with one finger) |
| O - Onset | "Did it come on suddenly or gradually?" |
| C - Character | "Is it sharp, dull, crampy, burning, colicky?" |
| R - Radiation | "Does it spread anywhere? Back? Shoulder tip? Groin?" |
| A - Associated symptoms | (see below) |
| T - Timing | "Is it constant or does it come and go?" |
| E - Exacerbating/relieving factors | "What makes it better or worse? Food? Posture? Movement?" |
| S - Severity | "On a scale of 1-10, how bad is the pain?" |
For Abdominal Swelling / Distension
- Onset: sudden or gradual?
- Which part of the abdomen?
- Any pain associated with it?
- Any change in urine output or colour?
- Ankle swelling (ascites from cardiac/liver/nephrotic)?
For Jaundice
- Duration and progression
- Dark urine / pale stools / pruritus (obstructive jaundice triad)
- Fever and rigors (Charcot's triad → cholangitis)?
- Contact with jaundiced persons (hepatitis)
- Blood transfusions / IV drug use (hepatitis B/C)
- Alcohol history
- Recent travel
3. ASSOCIATED SYMPTOMS - Ask Specifically
Gastrointestinal
| Symptom | Why it matters |
|---|---|
| Nausea / vomiting | Content? Blood (haematemesis)? |
| Dysphagia | Oesophageal pathology |
| Heartburn / regurgitation | GORD |
| Anorexia / weight loss | Malignancy, chronic liver disease |
| Bowel habits | Constipation vs diarrhoea |
| Blood in stool | Frank red (lower GI) vs melaena (upper GI) |
| Mucus in stool | IBD, colorectal carcinoma |
| Pale/clay stools | Biliary obstruction |
| Dark urine | Haemolysis, hepatitis, biliary obstruction |
| Abdominal distension | Ascites, obstruction, gas |
| Tenesmus | Rectal pathology |
Systemic
| Symptom | Why it matters |
|---|---|
| Fever / chills / rigors | Infection, cholangitis, abscess, malaria |
| Night sweats | TB, lymphoma |
| Fatigue / weakness | Anaemia, CLD, malignancy |
| Pruritus (itching) | Obstructive jaundice, cholestasis, PBC |
| Easy bruising / bleeding | Coagulopathy (liver disease) |
| Peripheral oedema | Hypoalbuminaemia, cardiac failure |
| Shortness of breath | Massive ascites, hepatic hydrothorax, anaemia |
| Joint pains | Haemochromatosis, IBD, SLE |
| Skin rash | SLE, Still's disease, secondary syphilis |
4. PAST MEDICAL HISTORY (PMH)
- Previous episodes of similar complaints
- Known liver disease / hepatitis (B, C)
- Known gallstones / biliary disease
- Diabetes mellitus (NAFLD)
- Hypertension / cardiac disease (congestive hepatomegaly)
- Malignancy (any prior cancer → metastases)
- Previous abdominal surgery
- Blood transfusions
- Autoimmune diseases (SLE, rheumatoid arthritis, IBD)
- Haematological conditions (thalassaemia, sickle cell)
5. DRUG HISTORY (DH)
| Category | Examples |
|---|---|
| Hepatotoxic drugs | Methotrexate, isoniazid, paracetamol (overdose), amiodarone, statins, rifampicin |
| Drugs causing splenomegaly | Phenytoin |
| Anticoagulants | Warfarin, heparin (bleeding risk) |
| OCP | Risk of hepatic adenoma, Budd-Chiari |
| NSAIDs | GI bleeding, renal impairment in liver disease |
| Alcohol | Quantify - units per week (safe limit: ♂ <14 units/week, ♀ <14 units/week) |
| Herbal / traditional medicines | Often hepatotoxic |
6. FAMILY HISTORY (FH)
- Liver disease / jaundice in family
- Haematological disorders (thalassaemia, sickle cell, hereditary spherocytosis)
- Storage diseases (Gaucher's, Wilson's disease - autosomal recessive)
- Haemochromatosis (HFE gene mutation)
- Malignancy (colorectal cancer, HCC)
- Polycystic kidney/liver disease
7. SOCIAL HISTORY (SH)
Alcohol
- How much? How often? For how long?
- Type of alcohol
- CAGE questionnaire: Cut down? Annoyed? Guilty? Eye-opener?
Smoking
- Pack years (risk of pancreatitis, malignancy)
Occupation
- Farmer / abattoir (brucellosis, leptospirosis)
- Healthcare worker (hepatitis B/C risk)
- Chemical / solvent exposure (hepatotoxins)
Travel History
- Travel to tropics → malaria, kala-azar, typhoid, schistosomiasis, hepatitis A/E
- Where? When? Prophylaxis taken?
Sexual History
- Unprotected intercourse → hepatitis B/C, HIV, syphilis
IV Drug Use / Tattoos / Piercings
- Hepatitis B, C, HIV risk
Diet
- Raw shellfish → hepatitis A, E
- Animal contact → brucellosis, leptospirosis
Living Conditions
- Overcrowding → TB, typhoid, hepatitis A
8. REVIEW OF SYSTEMS (ROS)
- Cardiorespiratory: cough, breathlessness, chest pain (right heart failure causing hepatomegaly)
- Urological: decreased urine output (hepatorenal syndrome, nephrotic)
- Neurological: confusion, flapping tremor/asterixis (hepatic encephalopathy)
- Musculoskeletal: arthralgia, bone pain (Gaucher's, haemochromatosis)
- Endocrine: thyroid symptoms (thyrotoxicosis → mild hepatosplenomegaly)
OSCE Memory Aid: "ABCDE Symptoms" for Abdominal History
| Letter | Symptom group |
|---|---|
| A | Appetite/Anorexia/Abdominal pain |
| B | Bowel habit change / Bleeding (haematemesis, melaena, PR bleed) |
| C | Colour change (jaundice, dark urine, pale stools) |
| D | Distension / Dysphagia / Dark urine |
| E | Energy loss / constitutional (fever, weight loss, night sweats) |
Clinical Correlation: History Clues → Likely Diagnosis
| History Clue | Think |
|---|---|
| Alcohol excess + jaundice + RUQ pain | Alcoholic hepatitis / cirrhosis |
| IV drug use + jaundice + fever | Hepatitis B/C, endocarditis |
| Travel to tropics + fever + anaemia | Malaria, kala-azar, typhoid |
| Young patient + pharyngitis + hepatosplenomegaly | EBV mononucleosis |
| OCP use + Budd-Chiari features | Hepatic vein thrombosis |
| Pale stools + dark urine + pruritus + fever + RUQ pain | Cholangitis (Charcot's triad) |
| Weight loss + B symptoms + lymphadenopathy | Lymphoma / TB |
| Family history + bronze skin + DM + arthropathy | Haemochromatosis |
| Child + bone pain + Ashkenazi Jewish | Gaucher's disease |
| Arthritis + butterfly rash | SLE hepatitis |
I need it like symptoms and what all it rules out and what all negative history I should ask to rule out what
Per Abdomen History - Symptom-Based with Rule In / Rule Out Logic
PRESENTING COMPLAINT: Hepatosplenomegaly / Abdominal Mass / Jaundice
A. FEVER
If PRESENT → Suggests:
- Infection: malaria, kala-azar, typhoid, EBV, brucellosis, TB, leptospirosis
- Lymphoma (B symptoms)
- Still's disease / HLH
- SBP (in ascites patient)
- Cholangitis
Negative History to Ask (to rule out specific causes):
| Question | Rules Out if Negative |
|---|---|
| "Did you travel to any tropical country recently?" | Malaria, kala-azar, typhoid, schistosomiasis |
| "Did you have sore throat along with the fever?" | EBV (infectious mononucleosis) |
| "Was the fever coming and going in cycles / every 48-72 hrs?" | Malaria (tertian/quartan pattern) |
| "Did you have rigors (violent shivering) with the fever?" | Malaria, cholangitis, sepsis |
| "Did you have months of low-grade fever with weight loss?" | TB, lymphoma, kala-azar |
| "Any contact with animals / farm / unpasteurised milk?" | Brucellosis, leptospirosis |
| "Any night sweats along with the fever?" | TB, lymphoma |
| "Any skin rash with the fever?" | Still's disease, typhoid (rose spots), syphilis |
| "Any abdominal pain with the fever?" | Cholangitis, liver abscess, SBP |
B. JAUNDICE
If PRESENT → Suggests:
- Hepatitis (viral, alcoholic, drug-induced)
- Biliary obstruction (gallstones, cholangiocarcinoma, head of pancreas CA)
- Haemolysis
- Cirrhosis (late)
Negative History to Ask:
| Question | Rules Out if Negative |
|---|---|
| "Did you notice pale / clay-coloured stools?" | Obstructive (surgical) jaundice - rules out biliary obstruction if absent |
| "Did your urine turn dark (tea-coloured)?" | Obstructive jaundice, hepatitis |
| "Did you have itching (pruritus) all over?" | Obstructive jaundice / cholestasis (PBC) - suggests if present |
| "Any fever and pain in the right side with jaundice?" | Charcot's triad → cholangitis (fever + jaundice + RUQ pain) |
| "Did other family members or contacts develop jaundice around the same time?" | Hepatitis A/E (faeco-oral, epidemic) |
| "Any recent blood transfusion or injection / shared needles?" | Hepatitis B, C, HIV |
| "Do you drink alcohol regularly? How much?" | Alcoholic hepatitis / cirrhosis |
| "Have you taken any new medications or herbal medicines?" | Drug-induced jaundice |
| "Any episode of sudden worsening of anaemia with dark urine?" | Haemolytic jaundice (G6PD, thalassaemia crisis) |
C. ABDOMINAL PAIN
If PRESENT → Use SOCRATES; then ask:
| Question | Rules Out if Negative |
|---|---|
| "Is the pain in the right upper quadrant?" | Liver pathology, cholecystitis, hepatitis |
| "Does the pain radiate to your right shoulder tip?" | Diaphragmatic irritation (hepatic abscess, perforated viscus) |
| "Does the pain radiate to your back?" | Pancreatitis, carcinoma head of pancreas, aortic aneurysm |
| "Is the pain colicky - coming and going in waves?" | Biliary colic, ureteric colic, intestinal obstruction |
| "Does eating make it worse?" | Peptic ulcer (worse with food = gastric; better with food = duodenal); mesenteric angina (chronic ischaemia) |
| "Is the pain relieved by opening your bowels?" | Irritable bowel syndrome, bowel pathology |
| "Is the pain worse when you breathe in?" | Peritonism, hepatic/splenic pathology |
D. ABDOMINAL SWELLING / DISTENSION
If PRESENT → Think: Ascites, organomegaly, mass, gas, obesity, pregnancy
| Question | Rules Out if Negative |
|---|---|
| "Has the swelling been increasing gradually over weeks/months?" | Cirrhosis / malignant ascites / slowly growing mass |
| "Did the swelling come on suddenly?" | Acute obstruction, haemoperitoneum, acute liver failure |
| "Is it associated with swelling of both legs / ankle swelling?" | Hypoalbuminaemia (cirrhosis, nephrotic), cardiac failure → rules out these if no leg swelling |
| "Any breathlessness due to the swelling?" | Massive ascites pushing up diaphragm, hepatic hydrothorax |
| "Do you pass less urine than usual?" | Hepatorenal syndrome, nephrotic syndrome, cardiac failure |
| "Any history of heart disease?" | Cardiac ascites / congestive hepatomegaly - rules out if no cardiac history |
| "Is the swelling in a specific region only or all over the abdomen?" | Localised = organomegaly/mass; diffuse = ascites/gas |
E. WEIGHT LOSS / ANOREXIA
If PRESENT → Suggests:
- Malignancy (HCC, lymphoma, metastases, pancreatic CA)
- Chronic infections (TB, kala-azar, HIV)
- Cirrhosis / chronic liver disease
- Chronic inflammatory conditions
| Question | Rules Out if Negative |
|---|---|
| "How much weight have you lost and over how long?" | Rapid severe loss → malignancy; gradual → CLD, TB |
| "Is your appetite completely lost or reduced?" | Complete anorexia suggests malignancy or severe liver disease |
| "Any early satiety (feeling full very quickly)?" | Massive splenomegaly compressing stomach; gastric cancer |
| "Any night sweats along with weight loss?" | TB, lymphoma - rules out if absent |
| "Any chronic cough or breathlessness along with weight loss?" | TB (pulmonary), lymphoma with mediastinal involvement |
| "Any change in bowel habits along with weight loss?" | Colorectal malignancy with liver metastases |
F. BLEEDING
If PRESENT → Suggests: Portal hypertension (varices), coagulopathy, malignancy
| Question | Rules Out if Negative |
|---|---|
| "Did you vomit blood (haematemesis)? What colour?" | Bright red = active variceal/arterial bleed; coffee-ground = slower upper GI bleed |
| "Did you pass black tarry stools (melaena)?" | Upper GI bleed (varices, peptic ulcer) - rules out upper GI source if absent |
| "Did you pass fresh red blood in stools?" | Lower GI bleed, anorectal pathology |
| "Do you bruise easily or bleed from minor cuts for a long time?" | Coagulopathy of liver disease, thrombocytopenia (hypersplenism) |
| "Any bleeding from gums or nose?" | Coagulopathy, leukaemia, thrombocytopenia |
G. BOWEL HABIT CHANGES
| Question | Rules Out if Negative |
|---|---|
| "Have you noticed any change in your bowel habit?" | Colorectal cancer (alternating constipation/diarrhoea), IBD |
| "Any mucus or blood mixed in the stools?" | Colorectal CA, IBD, amoebic colitis |
| "Any pale / greasy stools that are hard to flush?" | Steatorrhoea → malabsorption, cholestasis, pancreatic insufficiency |
| "Any diarrhoea?" | Infective cause, IBD, colorectal CA, carcinoid |
| "Any constipation?" | Colorectal CA, hypothyroidism |
H. ALCOHOL HISTORY (Always ask in EVERY abdominal case)
| Question | Significance |
|---|---|
| "Do you drink alcohol?" | Opens the question |
| "How much per week? What type?" | Quantify in units |
| "For how many years have you been drinking?" | Duration determines damage |
| "Have you ever tried to cut down?" (CAGE) | Dependence assessment |
- Alcoholic hepatitis, alcoholic cirrhosis, alcoholic pancreatitis
I. DRUG / MEDICATION HISTORY
| Question | Rules Out if Negative |
|---|---|
| "Do you take any regular medications?" | Drug-induced hepatitis, drug-induced cholestasis |
| "Any herbal or traditional medicines?" | Hepatotoxic herbals (very common, often missed) |
| "Any painkillers (paracetamol, ibuprofen)?" | Paracetamol overdose, NSAID-induced GI bleed |
| "Have you used any injections / IV drugs?" | Hepatitis B, C, HIV - rules out if never injected |
| "Any long-term medications like methotrexate, isoniazid, amiodarone?" | Specific drug-induced liver disease |
| "OCP use?" (in women) | Hepatic adenoma, Budd-Chiari syndrome |
J. SOCIAL / EXPOSURE HISTORY
| Question | Rules Out if Negative |
|---|---|
| "Any contact with a jaundiced person recently?" | Hepatitis A / E (faeco-oral) - rules out epidemic hepatitis |
| "Did you eat raw shellfish or food from unhygienic sources?" | Hepatitis A / E |
| "Any unprotected sexual contact?" | Hepatitis B, C, HIV, syphilis |
| "Any recent tattooing or body piercing?" | Hepatitis B, C |
| "Do you work with animals or on a farm?" | Brucellosis, leptospirosis, hydatid cyst |
| "Have you worked in a mine / construction / in water?" | Leptospirosis (water exposure), schistosomiasis |
| "Any family member with similar illness?" | Hereditary haemochromatosis, Wilson's, thalassaemia, Gilbert's |
K. FAMILY HISTORY
| Question | Rules Out if Negative |
|---|---|
| "Any family member with liver disease or jaundice?" | Hereditary causes (haemochromatosis, Wilson's, Gilbert's) |
| "Any family member with blood disorders?" | Thalassaemia, sickle cell, hereditary spherocytosis |
| "Any family member with similar abdominal swelling?" | Polycystic liver/kidney disease, familial malignancy |
| "Any family member with cancer?" | Familial colorectal CA, HCC in HBV-infected families |
SUMMARY CARD: Positive vs Negative History at a Glance
| Symptom Present | Rules In | Negative History Needed | Rules Out |
|---|---|---|---|
| Cyclical fever + travel | Malaria | No travel → | Malaria less likely |
| Pharyngitis + HSM | EBV | No sore throat → | Mononucleosis less likely |
| Pale stools + dark urine + itch | Obstructive jaundice | Stools normal coloured → | Biliary obstruction less likely |
| Night sweats + weight loss | TB / Lymphoma | No night sweats → | TB/lymphoma less likely |
| Alcohol history | Alcoholic liver disease | No alcohol → | Alcoholic CLD excluded |
| IV drug use / tattoos | Hepatitis B/C | Never → | Blood-borne hepatitis less likely |
| Easy bruising | Coagulopathy / CLD | No bruising → | Severe coagulopathy less likely |
| Haematemesis | Varices / upper GI bleed | No → | Variceal bleed less likely |
| Animal contact | Brucellosis / leptospirosis | No animal contact → | Zoonosis less likely |
| Family liver disease | Hereditary (HH, Wilson's) | No family history → | Hereditary cause less likely |