If serum trop-I, and echo are normal but T-inversions in ECG
Reading File
Finding Sources
Finding Sources
Searching the Web
T wave inversion normal troponin normal echo differential diagnosis causes
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a thorough, well-illustrated answer. Here it is:
T-Inversions on ECG with Normal Trop-I and Normal Echo
This combination - abnormal ECG but negative biomarkers and preserved wall motion - is a classic diagnostic dilemma. It narrows your differential significantly but does not rule out serious disease.
Why the Echo is Normal (and Why That's Dangerous)
Wall motion abnormalities on echo appear only with ongoing ischemia or completed necrosis. If the ischemic episode has resolved by the time the echo was done, the myocardium may look completely normal even in high-grade CAD. This is the key trap of Wellens syndrome (see below).
The Differential Diagnosis
Organized by urgency:
1. Wellens Syndrome (DO NOT MISS - HIGH PRIORITY)
The most dangerous cause of this exact triad.
- Biphasic or deeply symmetric inverted T waves in V2-V4
- Occurs in the pain-free window - troponin may still be normal or mildly elevated
- Echo is normal because ischemia is not ongoing at the time of study
- Represents critical proximal LAD stenosis (>80%)
- Type A (25%): Biphasic T waves (positive-then-negative) in V2-V3
- Type B (75%): Deep, symmetric T-wave inversions in V2-V3
From the Washington Manual: "Biphasic or deeply inverted T waves (>5 mm) with QT prolongation in leads V2 to V4 in the setting of stuttering chest pain within the past 24 hours suggests a critical lesion in the LAD artery distribution (Wellens syndrome)."
These patients must NOT undergo stress testing - it can precipitate massive anterior MI. They need urgent coronary angiography.
ECG patterns of ACS-related T-wave inversions:
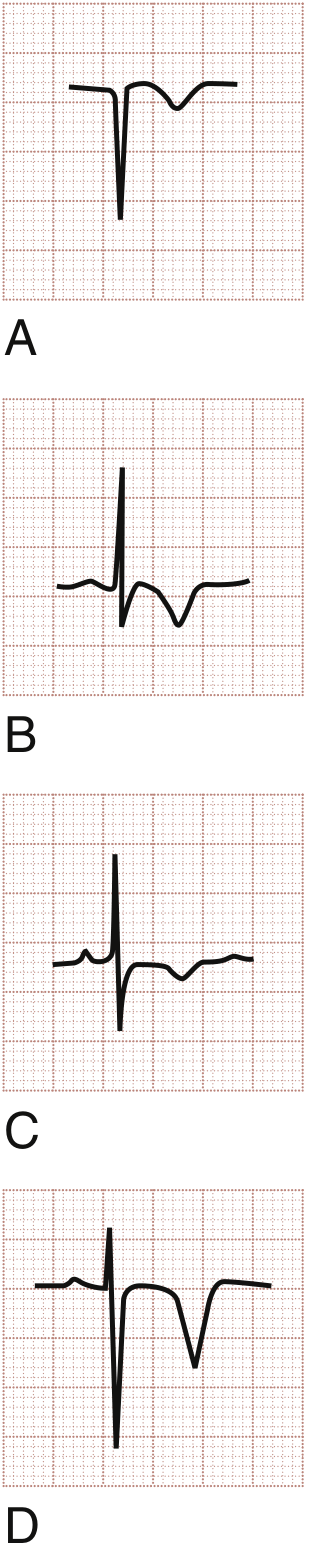
Wellens syndrome ECG patterns:
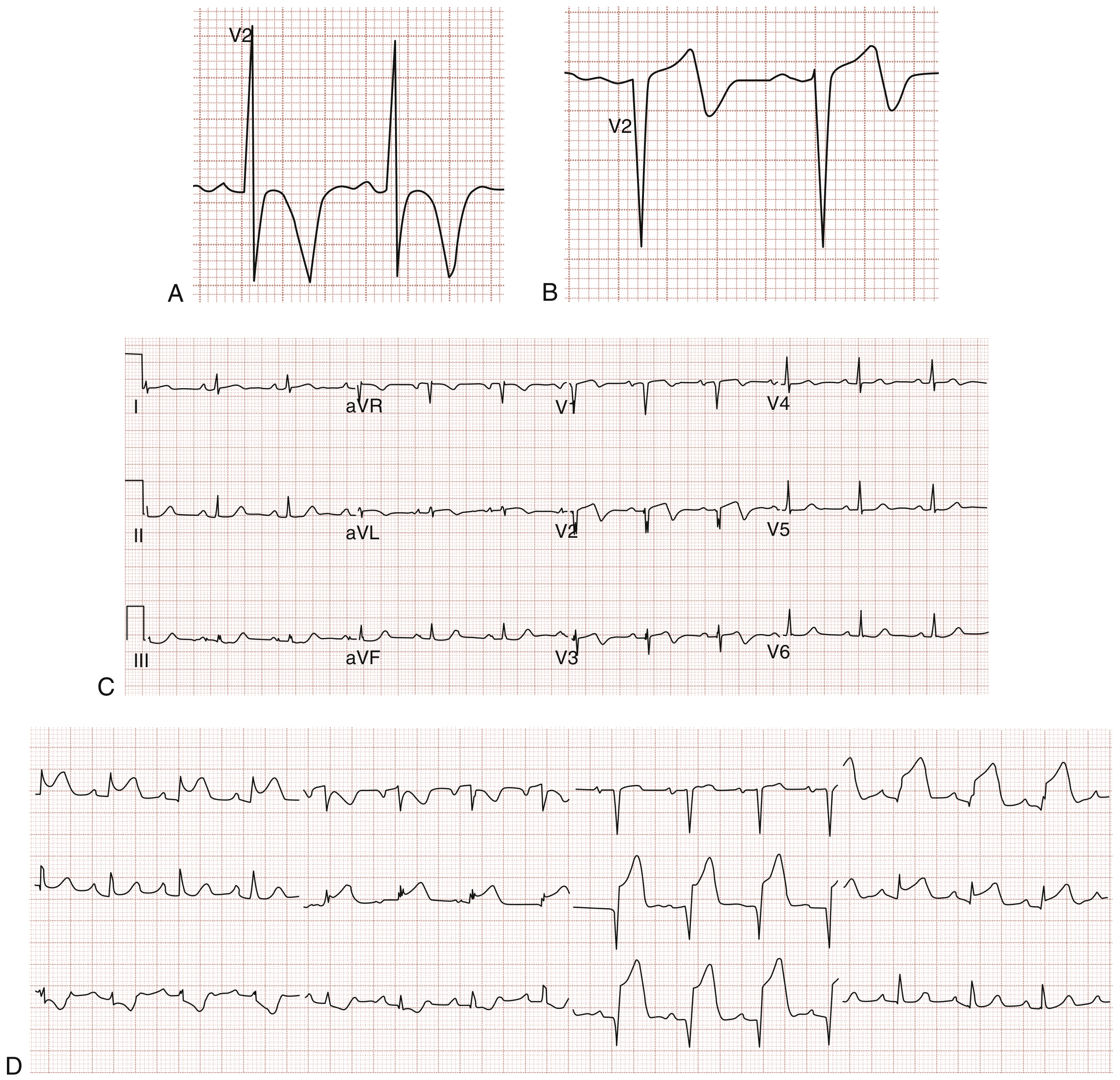
(Images from Rosen's Emergency Medicine)
2. Pulmonary Embolism
- T-wave inversions in V1-V4 (right heart strain pattern), often with T inversions in III and aVF as well
- Classic S1Q3T3 pattern (not always present)
- Troponin may be mildly elevated with massive PE, but can be normal in submassive/small PE
- Echo may show RV strain/dilation but can be normal in smaller emboli
- Consider if there is tachycardia, low SpO2, pleuritic chest pain, or risk factors (immobility, malignancy, prior DVT)
- Next step: D-dimer + CT pulmonary angiography
3. Pericarditis (Resolving Phase)
- During pericarditis, the evolution is: diffuse ST elevation -> ST normalization -> diffuse T-wave inversions -> normalization
- T inversions in this stage are typically diffuse (multiple leads), not regional
- Troponin can be mildly elevated if there is myopericarditis but may be normal in pure pericarditis
- Echo may show small pericardial effusion, but can be normal
4. Myocarditis
- Can cause regional or diffuse T inversions
- Troponin is often elevated, but early or mild myocarditis may have a normal initial troponin
- Echo may be normal early; repeat in 24-48 hours may show new wall motion abnormality or reduced EF
- Usually has a viral prodrome (fever, myalgia, upper respiratory illness)
5. Subarachnoid Hemorrhage / CNS Catastrophe
- Classic pattern: Deeply inverted T waves with a very wide, prolonged QT interval, sometimes called "cerebral T waves"
- Can mimic ACS on ECG perfectly
- Troponin is frequently elevated due to catecholamine surge (neurogenic myocardial injury), but can be normal
- Echo can show transient wall motion abnormality (stress cardiomyopathy) but may be normal
- Key clue: severe headache ("thunderclap"), altered consciousness, focal neurological deficit
- Next step: Non-contrast CT head + LP if CT negative
6. Takotsubo (Stress) Cardiomyopathy - Resolving Phase
- Deep T inversions typically appear after the acute phase, as the apical ballooning resolves
- At that stage, echo may have normalized wall motion while T inversions persist on ECG
- Troponin may already have peaked and returned near-normal
- Triggered by physical or emotional stress
7. ARVC (Arrhythmogenic Right Ventricular Cardiomyopathy)
- T inversions in V1-V3 (right precordial leads) - a classic finding
- Look for epsilon waves, RBBB morphology, ventricular ectopy with LBBB pattern
- Echo may look normal early in disease; cardiac MRI (with late gadolinium enhancement) is the diagnostic test
- Usually presents in young adults with palpitations or syncope
8. Secondary T-Wave Changes (Structural/Electrical)
- LVH: T-wave inversions in lateral leads (I, aVL, V5-V6) - "strain pattern" - with increased QRS voltage
- RBBB: T inversions in V1-V3 as expected discordant change
- WPW: "Pseudo-infarction" T changes
9. Benign / Non-Urgent Causes
- Persistent juvenile T-wave pattern: Shallow, asymmetric T inversions in V1-V3 in young adults (especially women) - diagnosis of exclusion
- Digitalis effect: Sagging ST with T flattening/inversion at therapeutic levels
- Hyperventilation: Can transiently invert T waves
- Post-tachycardia cardiac memory: T inversions persisting after resolution of tachycardia (rate-related)
- Normal variant: Isolated T inversion in lead III or aVL alone is often normal
Practical Approach
| Step | Action |
|---|---|
| 1 | Identify the lead distribution of the T inversions (anterior V1-V4? lateral? inferior? diffuse?) |
| 2 | Correlate with symptoms - is the patient pain-free? Any history of chest pain in the last 24 hours? |
| 3 | Serial troponins - a single negative troponin does not rule out demand ischemia; repeat at 3-6 hours |
| 4 | If anterior T inversions + recent stuttering chest pain + pain-free now: treat as Wellens until proven otherwise - urgent cardiology review, NO stress test |
| 5 | If tachycardia + hypoxia + risk factors: CT-PA to rule out PE |
| 6 | If thunderclap headache: CT head immediately |
| 7 | If persistent uncertainty after serial troponins: cardiac MRI (catches myocarditis, ARVC, Takotsubo residua that echo misses) |
Bottom line: Normal troponin and normal echo do not make T-inversions benign. Wellens syndrome and PE are the most time-critical diagnoses to exclude. The lead distribution and clinical context are the key to narrowing this differential. - Rosen's Emergency Medicine; Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.