Parkinson disease
Reading File
Finding Sources
Searching PubMed
"Parkinson disease"[MeSH Terms] AND treatment
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have all the content needed for a comprehensive answer. Let me compile it.
Parkinson Disease
Overview
Parkinson disease (PD) is the second most common age-related neurodegenerative disorder, exceeded only by Alzheimer disease. First described by English physician James Parkinson in 1817, it affects approximately 10.8 million people worldwide. Incidence rises sharply with age - about 1% of those over 60 and 4-5% over 85 are affected. The mean age of onset is ~60 years; lifetime risk is ~3% in men and ~2% in women. - Harrison's Principles of Internal Medicine 22E, p.3537
Pathology
Gross and Microscopic Changes
The hallmark pathological features are:
- Degeneration of dopaminergic neurons in the substantia nigra pars compacta (SNc), causing grossly visible pallor of the substantia nigra and locus coeruleus
- Reduced striatal dopamine - dopaminergic neurons project from the SN to the striatum to control motor activity
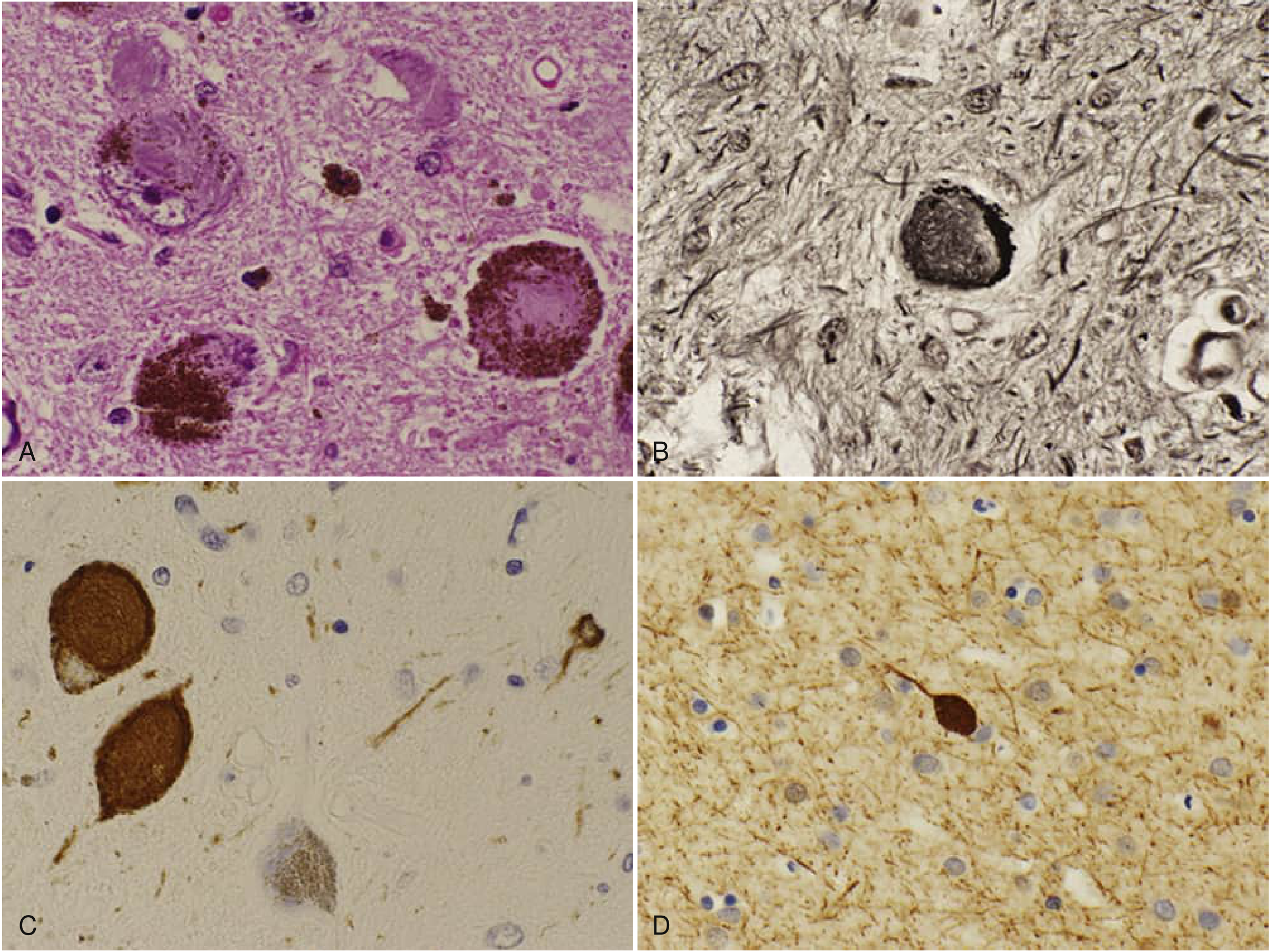
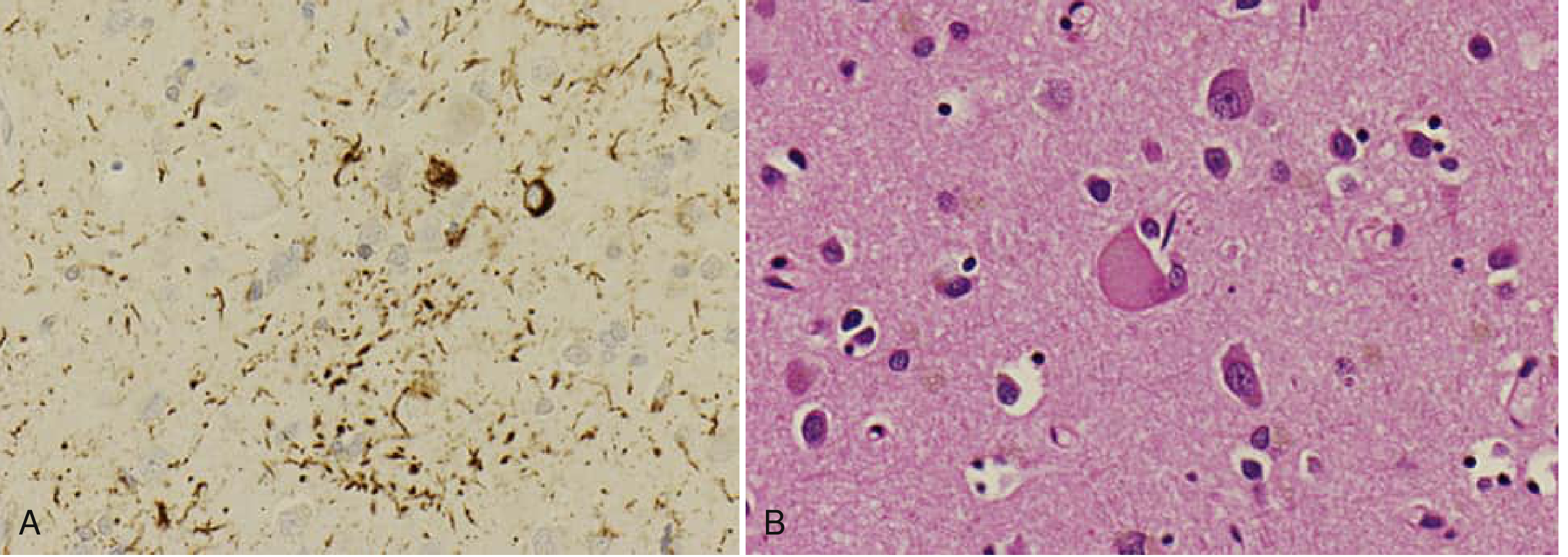
- Lewy bodies - intraneuronal, eosinophilic, round-to-elongated cytoplasmic inclusions composed of fine filaments of α-synuclein, neurofilaments, and ubiquitin. Neurons containing Lewy bodies are surrounded by gliosis
- Lewy neurites - dystrophic axonal processes also containing aggregated α-synuclein
- Robbins & Kumar Basic Pathology, p.854
Neuronal degeneration with Lewy pathology is not limited to dopamine neurons - it also affects:
- Cholinergic neurons of the nucleus basalis of Meynert
- Norepinephrine neurons of the locus coeruleus
- Serotonin neurons of the raphe nuclei
- Neurons of the olfactory system, spinal cord, and peripheral autonomic nervous system
- Harrison's, p.3537
Pathogenesis
The central mechanism involves α-synuclein aggregation and toxicity. The diagram below illustrates the key pathway:
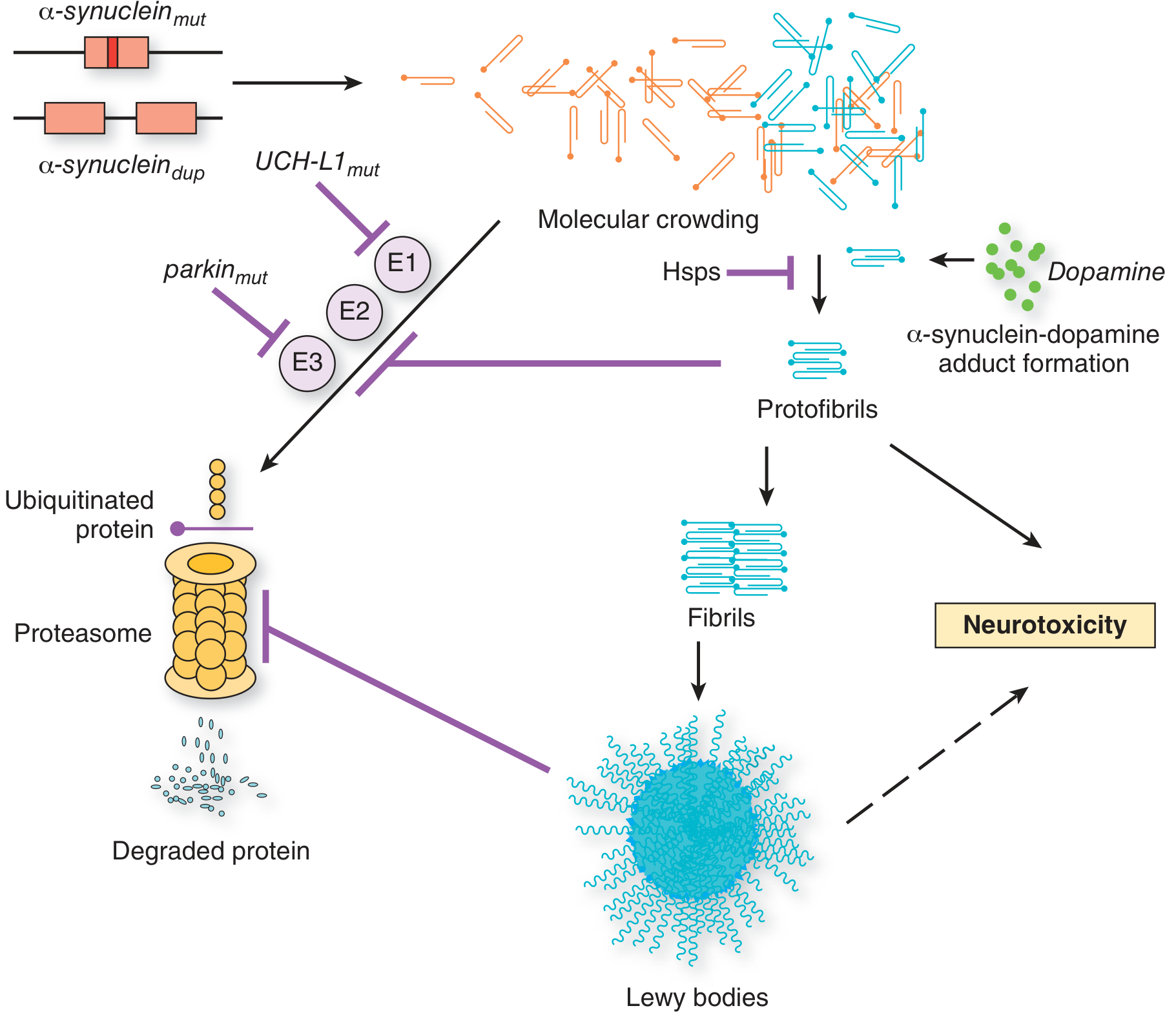
Mutations or duplications of the α-synuclein gene, or mutations in UCH-L1/parkin that impair ubiquitin-proteasome degradation, lead to α-synuclein aggregation → protofibrils → fibrils → Lewy bodies → neurotoxicity. Dopamine itself can form adducts with α-synuclein, accelerating aggregation. - Adams and Victor's Principles of Neurology, 12th Ed.
Key molecular mechanisms include:
- Impaired autophagy and lysosomal degradation - several PD-associated genes (Parkin, others) play roles in endosomal trafficking and mitochondrial function
- Mitochondrial dysfunction - PINK1 (PTEN-induced putative kinase 1) is a mitochondrial gene mutated in early-onset PD
- Oxidative stress - the DJ-1 protein plays a role in cellular response to oxidative stress
Genetics
Most PD is sporadic, but 5-15% of cases involve pathogenic gene mutations. Key genetic loci include:
| Notation | Gene (Protein) | Inheritance | Age of Onset | Lewy Bodies | Notes |
|---|---|---|---|---|---|
| Park1/Park4 | SCNA (α-synuclein) | AD | 30-40 years | + | A53T, A30P mutations promote α-synuclein oligomerization |
| Park2 | PARK2 (Parkin) | AR | 20-40 years | - | 50% of early-onset inherited PD; 20% of "sporadic" early-onset cases |
| Park5 | UCHL-1 (ubiquitin esterase) | AD/SNP | 50s | + | Mutations decrease ubiquitin monomer recycling |
| Park6 | PINK1 | AR | Variable | - | Mitochondrial gene |
| Park7 | DJ-1 | AR | 30s | ? | Slow progression; oxidative stress response |
| Park8 | LRRK2 | AD | Late | ± | Most common autosomal dominant PD; common in Ashkenazi Jews |
GBA1 (glucocerebrosidase) variants are the single most common genetic risk factor for PD (up to 15% of cases). Heterozygosity for Gaucher-causing mutations in GBA1 confers risk.
- Adams and Victor's Principles of Neurology, 12th Ed., p.1091
Clinical Features
Cardinal Motor Features (TRAP)
- Tremor - rest ("pill-rolling") tremor; presenting symptom in up to 70% of patients; typically asymmetric and virtually pathognomonic. Differentiated from essential tremor (which is action-type and symmetric)
- Rigidity - increased tone with "cogwheel" ratchety quality on passive limb movement
- Akinesia/Bradykinesia - slowness of movement; patients describe it as limb "weakness" though strength testing is normal
- Postural instability - late finding; contributes to falls and aspiration pneumonia
Other Motor Features
- Micrographia (small handwriting)
- Masked facies (hypomimia) - reduced facial expression
- Shuffling, narrow-based gait
- Hypophonia (soft voice)
- Drooling
- Dysphagia (subjective in 35%, objective evidence in up to 82%)
- Freezing of gait
Non-Motor Features (often underappreciated)
| Category | Examples |
|---|---|
| Autonomic | Orthostatic hypotension, GI disturbances (constipation), genitourinary disturbances |
| Sensory | Anosmia (often prodromal), pain |
| Mood | Depression, anxiety, apathy |
| Sleep | Fragmented sleep, REM sleep behavior disorder (RBD) |
| Cognitive | Mild cognitive impairment → dementia (Parkinson disease dementia / Lewy body dementia spectrum) |
"The disease usually progresses over 10 to 15 years, eventually producing severe motor slowing to the point of near immobility. Death often results from aspiration pneumonia or trauma from falls." - Robbins & Kumar Basic Pathology, p.854
- Harrison's Principles of Internal Medicine 22E, p.3537
Differential Diagnosis - Parkinsonism-Plus Syndromes
Up to 20% of patients initially diagnosed with PD have an alternative diagnosis. Features that suggest a parkinsonism-plus syndrome and warrant further evaluation:
- Hallucinations (early)
- Paralysis of upward gaze (progressive supranuclear palsy, PSP)
- Early dementia (dementia with Lewy bodies)
- Early postural instability
- Early autonomic dysfunction (multiple system atrophy, MSA)
- Failure to respond to levodopa
Key alternative diagnoses: PSP, dementia with Lewy bodies, multiple system atrophy, vascular parkinsonism, drug-induced parkinsonism (dopamine antagonists)
- Textbook of Family Medicine 9e, p.1249
Diagnosis
Diagnosis is primarily clinical, based on cardinal features. Investigations include:
-
DaT-SPECT (dopamine transporter scan) - shows reduced striatal uptake, most pronounced in the posterior putamen, typically asymmetric. Useful when there is diagnostic uncertainty (e.g., vs. essential tremor)
-
FDG-PET - increased avidity in striatum (abnormal finding in both PD and Lewy body disease)
-
α-Synuclein seeding amplification assay (SAA) - applied to CSF or skin; very high sensitivity and specificity to distinguish PD from other parkinsonisms; currently primarily a research tool, but blood-based versions are in development
-
MRI/Transcranial sonography - may detect increased iron in the SNc in prodromal PD
-
Genetic testing - not routine; consider in early onset (<40 years), strong family history, or specific ethnic backgrounds
-
Harrison's Principles of Internal Medicine 22E, p.3537-3538
Treatment
Pharmacological
| Drug Class | Agents | Dose | Benefit | Key Side Effects |
|---|---|---|---|---|
| L-DOPA | Carbidopa/levodopa | 25/100 mg TID up to 50/250 mg q3h | Best motor benefit; reduces tremor and bradykinesia | Nausea, dyskinesias, orthostatic hypotension, hallucinations |
| Dopamine agonists | Ropinirole (9-24 mg/d), Pramipexole (0.75-3 mg/d) | Start low, titrate | Moderate motor benefit; reduce L-DOPA fluctuations | Orthostatic hypotension, sudden-onset sleep, impulse control disorders |
| MAO-B inhibitors | Rasagiline (1 mg/d), Selegiline (5 mg BID) | - | Reduce "off" time; possible neuroprotection | Hypertensive crisis with tyramine-rich foods |
| COMT inhibitors | Entacapone (200 mg with L-DOPA) | - | Prolongs L-DOPA effect | Urine discoloration, diarrhea, increased dyskinesias |
| Glutamate antagonist | Amantadine (100 mg BID-TID) | - | Smooths motor fluctuations; reduces L-DOPA dyskinesias | Leg edema, CHF, confusion, insomnia |
| Anticholinergics | Benztropine, Trihexyphenidyl | Start 0.5 mg/d | Tremor reduction | Dry mouth, urinary retention, confusion, psychosis |
Adams and Victor's Principles of Neurology, 12th Ed., p.1093
L-DOPA Complications Over Time
As the disease advances, L-DOPA develops two major problems:
- Wearing-off / end-dose failure - the duration of each dose's benefit shortens ("on-off" fluctuations)
- L-DOPA-induced dyskinesias - choreoathetosis, dystonia, head wagging, grimacing, blepharospasm - due to denervation hypersensitivity of striatal dopamine receptors
These can be managed by adding dopamine agonists, COMT inhibitors, amantadine, or moving to device-aided therapy.
Surgical / Device-Aided Therapy
- Deep Brain Stimulation (DBS) - electrodes implanted in the globus pallidus or subthalamic nucleus to modulate basal ganglia circuitry. Allows significant reduction in L-DOPA dose in selected patients. Does not slow disease progression
- Levodopa-carbidopa intestinal gel (LCIG) - continuous duodenal infusion for advanced disease
Neuroprotection
No agent has conclusively shown slowing of neurodegeneration. MAO-B inhibitors (rasagiline - ADAGIO trial) showed mixed results. Vitamin E supplementation has shown negative results. This remains an active area of research. - Adams and Victor's Principles of Neurology, 12th Ed., p.1095
Recent Research (2025-2026)
Recent PubMed evidence highlights two emerging areas:
- GBA1 genetics: A 2025 systematic review (PMID: 39927608) provides updated classification of GBA1 variants and their genotype-phenotype relationships in PD, reinforcing GBA1 as the most important genetic risk factor
- Gut microbiome: A 2025 meta-analysis using machine learning (PMID: 40335465) identified consistent gut microbiome alterations in PD, supporting the gut-brain axis hypothesis in PD pathogenesis - particularly relevant given the early involvement of the enteric nervous system in Braak staging
Summary
| Feature | Detail |
|---|---|
| Epidemiology | 2nd most common neurodegenerative disease; age >60; M > F |
| Core pathology | Loss of SNc dopaminergic neurons; Lewy bodies (α-synuclein) |
| Cardinal features | Resting tremor, rigidity, bradykinesia, postural instability (TRAP) |
| Key non-motor | Anosmia, REM sleep disorder, depression, autonomic dysfunction, dementia |
| First-line treatment | Carbidopa/levodopa; dopamine agonists in younger patients |
| Surgery | DBS of STN or GPi for refractory motor fluctuations |
| Prognosis | Progressive over 10-15 years; death from aspiration pneumonia or falls |
Complete physiotherapy intervention
Finding Sources
Searching PubMed
"Parkinson disease"[MeSH Terms] AND "physical therapy"[MeSH Terms]
Searching the Web
physiotherapy intervention Parkinson disease guidelines 2024 2025 exercise gait balance
Finding Sources
Finding Sources
Searching PubMed
"Parkinson disease" AND "exercise" AND rehabilitation
Reading File
Reading File
Reading Article
PMID: 38588457
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC9046970
Reading Article
PMID: 37641007
I now have comprehensive evidence from the APTA guideline, Cochrane review, and textbooks. Let me compile the full physiotherapy intervention guide.
Physiotherapy Intervention in Parkinson Disease
Why Physiotherapy Matters
Parkinson disease causes progressive deterioration of motor function - bradykinesia, rigidity, postural instability, and gait impairment - that directly threaten independence and quality of life. Pharmacotherapy addresses dopamine deficits but does not target functional decline. Physiotherapy fills this gap by targeting the motor, balance, gait, and functional impairments that drugs cannot fully correct.
"Patients with PD can reduce their symptoms and improve their function with focused physical and occupational rehabilitation therapies to maintain range of motion, flexibility, proximal strength, mobility, freezing, safety, and fitness."
- Bradley and Daroff's Neurology in Clinical Practice
Goals of Physiotherapy in PD
| Domain | Goal |
|---|---|
| Motor symptoms | Reduce bradykinesia and rigidity; improve UPDRS motor scores |
| Gait | Improve stride length, cadence, gait speed, step symmetry |
| Balance | Reduce postural instability and falls |
| Functional mobility | Improve transfers, bed mobility, sit-to-stand |
| Freezing of gait (FOG) | Reduce frequency and severity of freezing episodes |
| Non-motor | Reduce depression, fatigue, and improve quality of life |
| Safety | Prevent falls; educate on assistive devices |
APTA Clinical Practice Guideline Recommendations (2022)
The APTA Clinical Practice Guideline provides the most comprehensive evidence-based framework. Recommendations are graded by evidence quality and strength:
| Intervention | Evidence Quality | Strength | Recommendation |
|---|---|---|---|
| Aerobic exercise | High | Strong (◆◆◆◆) | Should be implemented to reduce motor severity and improve fitness, gait, balance, and QoL |
| Resistance training | High | Strong (◆◆◆◆) | Should be implemented to reduce motor severity and improve strength, balance, gait, and QoL |
| Balance training | High | Strong (◆◆◆◆) | Should be implemented to reduce postural control impairments and improve balance, gait, mobility, and QoL |
| Gait training | High | Strong (◆◆◆◆) | Should be implemented to reduce motor severity and improve stride length, gait speed, mobility, and balance |
| External cueing | High | Strong (◆◆◆◆) | Should be implemented to reduce motor severity and FOG, improve gait outcomes |
| Task-specific training | High | Strong (◆◆◆◆) | Should be implemented to improve task-specific impairments and functional outcomes |
| Community-based exercise | High | Strong (◆◆◆◆) | Should be recommended to improve nonmotor symptoms, functional outcomes, and QoL |
| Behavior-change approach | High | Strong (◆◆◆◆) | Should be used to improve exercise adherence and physical activity levels |
| Integrated care | High | Strong (◆◆◆◆) | Should be used (multidisciplinary team approach) |
| Telerehabilitation | Moderate | Moderate (◆◆◆◇) | Should be considered as an alternative or supplement |
| Flexibility exercises | Low | Weak (◆◆◇◇) | May be implemented to improve ROM |
Specific Physiotherapy Interventions
1. Gait Training
Gait impairment in PD includes shortened stride length, reduced cadence, shuffling, and festination. Gait training is the most studied PT intervention.
Treadmill Training
- Body-weight support treadmill training (BWS-TT) is among the most effective interventions for balance and gait outcomes
- Improves stride length, cadence, gait speed, and functional mobility
- The treadmill itself acts as a form of external cueing, providing rhythmic sensory input
- Network meta-analysis (PMID: 37641007) found BWS-TT had the highest p-score for overall balance improvement
Overground Gait Training
- Practised with or without cueing
- Focuses on stride length amplification, heel-strike pattern, arm swing, and turning
Lee Silverman Voice Treatment (LSVT) BIG
- A specialised physiotherapy programme targeting amplitude of movement
- Patients are trained to make large, exaggerated movements to overcome hypokinesia
- Intensive: 16 sessions over 4 weeks; shown to improve gait speed, stride length, and motor UPDRS scores
2. External Cueing
This is one of the highest-impact interventions in PD physiotherapy, targeting bradykinesia and FOG.
Auditory Cueing (Rhythmic Auditory Stimulation - RAS)
- Metronome beats, music, or verbal prompts at a set cadence
- Patients are trained to synchronise steps to the rhythmic beat
- Immediately improves stride length and gait velocity
- Effective for FOG when used with balance training: RAS-supported balance training was superior to educational control in improving FOG frequency
- Delivered 2-5 times/week for 3-8 weeks; treadmill training with RAS outperforms overground gait training with RAS for FOG
Visual Cueing
- Transverse lines on the floor, laser lines from walking aids (e.g., U-Step walker with laser), or stripes on the ground
- Patients step over lines to trigger a normal step cycle and bypass the basal ganglia motor program deficit
- Highly effective for FOG
Combination Cueing
- Auditory + visual cueing together: greater improvements in gait speed, turning ability, and distance walked (6-Minute Walk Test)
3. Balance Training
PD causes postural instability due to impaired righting reflexes, flexed posture, and dopaminergic loss in circuits governing postural control.
Core components:
- Static balance exercises: single-leg standing, tandem stance, weight-shifting
- Dynamic balance exercises: stepping over obstacles, direction changes, perturbation training
- Reactive balance training: catching oneself after unexpected perturbations - most closely mimics real-world fall prevention
- Dual-task training: walking while performing a cognitive task (counting backwards, carrying a tray) - addresses the PD-specific vulnerability to cognitive-motor dual tasking
- Sensory orientation training: training with reduced visual or somatosensory input to improve vestibular reliance (foam surfaces, eyes closed)
Postural correction:
- Anterior trunk flexion ("camptocormia") is addressed with postural extension exercises, manual correction, and taping
- Mirror feedback, wall support exercises, and proprioceptive training improve body awareness
4. Aerobic Exercise
Strong evidence that aerobic training improves not just fitness but also motor symptoms, cognition, and mood in PD.
Forms:
- Walking, cycling (including stationary bike), swimming, Nordic walking
- High-intensity interval training (HIIT) is emerging as particularly effective
- Minimum: 150 minutes/week moderate intensity, as per general exercise guidelines
Benefits (2024 Cochrane review, PMID: 38588457 - 154 RCTs, 7,837 participants):
- Endurance/aerobic training: small to moderate beneficial effect on motor severity (UPDRS-M MD -5.76)
- Improved cardiovascular fitness, reduced fatigue, improved mood and depression
5. Resistance/Strength Training
Progressive resistance training addresses muscle weakness, which compounds bradykinesia in PD.
Focus areas:
- Lower limb extensor strength (quadriceps, hip abductors, calf) for gait and fall prevention
- Core stability for trunk control and posture
- Upper limb for ADL function
Evidence: High-quality evidence shows resistance training reduces motor severity and improves gait and balance. Results on the UPDRS-M are comparable to aerobic training.
6. Dance and Mind-Body Therapies
Dance (Tango, Ballroom, Zumba)
- The 2024 Cochrane network meta-analysis found dance had the greatest effect on motor severity of all exercise types (UPDRS-M MD -10.18, 95% CI -14.87 to -5.36 - a moderate effect; moderate confidence)
- Combines aerobic exercise, rhythmic cueing, balance challenge, and social engagement
- Tango is the most studied: improves balance, gait, and fear of falling
- "Several of our patients have taken up dancing and report that their balance in daily circumstances is improved." - Adams and Victor's Principles of Neurology, 12th Ed.
Tai Chi
- Shown to improve balance and significantly reduce falls in PD in RCTs
- Effects maintained at 3-month follow-up
- "Tai chi has been found to improve balance and reduce falls as measured by objective criteria (Li et al., 2012)" - Adams and Victor's Principles of Neurology
- Recommended by most Parkinson's associations
- Most studied martial art for PD; supervised groups preferred
Yoga
- Improves flexibility, balance, and reduces anxiety
- Supported by expert opinion; low-quality evidence formally
Pilates
- Network meta-analysis (PMID: 37641007) found Pilates was among the best interventions for proactive balance (p-score 0.95)
Aquatic Exercise
- Water provides resistance without fall risk; buoyancy reduces fear
- Aquatic exercise was best for static steady-state balance (sSSB, p-score 0.85) in the 2023 NMA
7. Task-Specific and Functional Training
Training must mirror real-world functional tasks to transfer to daily life:
Key tasks practised:
- Sit-to-stand from varying chair heights (including low chairs, toilet)
- Bed mobility: rolling, getting in/out of bed
- Floor transfers: getting up from the floor after a fall
- Turning: 90° and 180° turns in small spaces; one of the highest-risk activities for FOG and falls
- Reaching: overhead and forward reaching tasks
- Stair climbing: step-by-step strategy with handrail
- Dual-task functional training: carrying items while walking, talking while ambulating
Twice-weekly practice of whole-body functional movements (sitting, kneeling, standing, throwing) over 3 months improved mobility speed in moderately disabled PD patients. - Bradley and Daroff's Neurology
8. Stretching and Flexibility
PD produces rigidity and a characteristic flexed posture (stooped, arms adducted, elbows and knees flexed). Flexibility work counteracts this.
Targets:
- Hip flexors, chest/pectoral muscles (counteracting forward stoop)
- Cervical spine and thoracic extension
- Hamstrings and calf muscles
- Shoulder rotators
Methods: passive stretching, active-assisted stretching, yoga-based stretching, PNF (proprioceptive neuromuscular facilitation)
Evidence quality is low (APTA: ◆◆◇◇), but clinical benefit is widely observed and forms part of most comprehensive programmes.
9. Speech and Respiratory Physiotherapy
- Speech therapy / LSVT LOUD: addresses hypophonia (soft voice), monotone speech, dysarthria; intensive amplitude-based approach
- Respiratory physiotherapy: diaphragmatic breathing, expiratory muscle strength training - improves breath support for speech, reduces aspiration risk
- Swallowing therapy (SLP): critical given 35-82% prevalence of dysphagia in PD
10. Falls Prevention and Assistive Devices
Physiotherapists assess and address fall risk comprehensively:
Assessment of fall causes:
- Postural instability
- Orthostatic hypotension
- Medication timing (falls in "off" periods)
- Environmental hazards
- Footwear
Assistive devices:
- Standard quad cane: useful for mild instability
- Nordic/trekking poles: bilateral support; improve trunk extension
- 4-wheeled walker (rollator): preferred over front-wheeled walker (FWW increases falls in PD)
- U-Step walker: has built-in laser line or metronome for cueing; designed specifically for PD
- Wheeled mobility: when ambulation becomes unsafe
Home modification: remove trip hazards, add grab bars, improve lighting, non-slip mats
11. Pelvic Floor Physiotherapy
Often overlooked but important given autonomic dysfunction:
- Urinary urgency/incontinence affects up to 40% of PD patients
- Pelvic floor muscle training (PFMT): Kegel exercises, biofeedback
- Transcutaneous tibial nerve stimulation (TTNS) and percutaneous tibial nerve stimulation (PTNS): neuromodulatory approaches for bladder symptoms
12. Telerehabilitation
- APTA guideline: moderate quality, moderate recommendation
- Video-based physiotherapy sessions are feasible and effective, particularly for homebound patients
- Falls when travelling to clinic is a risk for late-stage PD
- Home exercise apps (e.g., Parkinson's UK apps, Beats Medical, PD Warrior) supplement supervised sessions
Exercise Dosing Principles
| Parameter | Recommendation |
|---|---|
| Frequency | 3-5 sessions/week |
| Duration | 45-60 min/session |
| Intensity | Moderate to vigorous (RPE 12-16/20) |
| Type | Multi-modal: combine aerobic + balance + strength + task-specific |
| Progression | Progressive overload; increase repetitions and difficulty over weeks |
| Timing | During medication "on" periods for optimal motor control |
| Monitoring | Use UPDRS motor scale, Berg Balance Scale, TUG, 6MWT, PDQ-39 |
Without an ongoing formal exercise programme, gains are lost within 6 months. - Bradley and Daroff's Neurology in Clinical Practice
Outcome Measures Used by Physiotherapists
| Measure | What It Assesses |
|---|---|
| UPDRS-III (motor) | Overall motor severity |
| Berg Balance Scale (BBS) | Static and dynamic balance |
| Timed Up and Go (TUG) | Functional mobility |
| 10-Metre Walk Test (10MWT) | Gait speed |
| 6-Minute Walk Test (6MWT) | Functional endurance |
| FOG Questionnaire (FOG-Q) | Freezing of gait severity |
| PDQ-39 | Quality of life (PD-specific) |
| Falls diary | Fall frequency |
| Mini-BESTest | Balance evaluation |
Disease Stage Considerations
| Stage (Hoehn & Yahr) | PT Focus |
|---|---|
| H&Y 1-2 (mild, unilateral) | Aerobic conditioning, strength, flexibility, education; prevent deconditioning |
| H&Y 2-3 (bilateral, postural changes) | Balance training, gait training, cueing strategies, fall prevention, task training |
| H&Y 3-4 (moderate-severe) | Intensive gait/balance, assistive devices, transfer training, caregiver education |
| H&Y 5 (wheelchair/bed-bound) | Passive range of motion, positioning, pressure care, caregiver training, comfort |
Key Evidence Summary
| Study | Finding |
|---|---|
| Cochrane NMA 2024 (PMID: 38588457) | Dance and gait/balance/functional training had the greatest effect on motor severity (UPDRS-M); 154 RCTs, 7,837 participants |
| NMA on balance 2023 (PMID: 37641007) | BWS treadmill training best for overall balance (BBS); Pilates best for proactive balance; aquatic exercise best for static balance; 199 studies, 9,523 patients |
| Home exercise meta-analysis 2023 (PMID: 38114897) | Home-based exercise significantly improves motor symptoms and QoL |
| APTA CPG 2022 | 10 strong recommendations covering all major intervention types |
Multidisciplinary Integration
Physiotherapy in PD works best as part of an integrated team:
- Neurologist: medication optimisation (exercise is most effective in "on" periods)
- Occupational therapist: ADL adaptations, fine motor training, home assessment
- Speech-language pathologist: dysphagia, voice, communication
- Physiotherapist: all motor, gait, balance, and exercise interventions above
- Psychologist/social worker: depression, anxiety, caregiver burden
- Pelvic floor PT: urinary symptoms
"Our position has been that any activity that keeps the patient moving and committed is of great value." - Adams and Victor's Principles of Neurology, 12th Ed.
Types of Parkinson
Finding Sources
Finding Sources
Searching the Web
types of Parkinson disease classification idiopathic atypical secondary parkinsonism 2024
Finding Sources
Finding Sources
Searching PubMed
"atypical parkinsonism"[MeSH Terms] AND diagnosis
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from all sources. Let me compile the full, detailed answer on types of Parkinson disease.
Types of Parkinson Disease (Parkinsonism)
"Parkinsonism" is a clinical syndrome defined by bradykinesia + at least one of: rigidity, rest tremor, or postural instability. It has many causes. The full classification is shown below.
Master Classification
PARKINSONISM
├── 1. PRIMARY (Neurodegenerative)
│ ├── A. Idiopathic Parkinson Disease (classic / sporadic PD)
│ ├── B. Genetic / Familial PD
│ └── C. Atypical Parkinsonism ("Parkinsonism-Plus")
│ ├── Multiple System Atrophy (MSA)
│ ├── Progressive Supranuclear Palsy (PSP)
│ ├── Corticobasal Degeneration (CBD)
│ └── Dementia with Lewy Bodies (DLB)
└── 2. SECONDARY (Acquired / Symptomatic)
├── Drug-induced parkinsonism
├── Vascular parkinsonism
├── Toxic parkinsonism (MPTP, CO, manganese)
├── Infectious (post-encephalitic)
├── Metabolic (Wilson's disease, hypothyroidism)
├── Structural (NPH, tumour, trauma)
└── Other heredodegenerative disorders
PART 1 - PRIMARY PARKINSONISM
A. Idiopathic Parkinson Disease (IPD)
The most common cause of parkinsonism (~75-80% of all cases).
| Feature | Detail |
|---|---|
| Other names | Sporadic PD, Parkinson's disease |
| Prevalence | ~1% of population >60 years |
| Pathology | Loss of dopaminergic neurons in substantia nigra pars compacta; Lewy bodies (α-synuclein inclusions) |
| Core features | TRAP: rest tremor (pill-rolling), rigidity (cogwheel), akinesia/bradykinesia, postural instability |
| Onset | Typically asymmetric |
| Tremor | Characteristic 4-6 Hz resting tremor (pill-rolling); present in 70% at onset |
| Response to L-DOPA | Excellent (hallmark feature; failure to respond questions the diagnosis) |
| Progression | Slow: 10-15 years to severe disability |
| Non-motor features | Anosmia, REM sleep behaviour disorder (RBD), depression, autonomic dysfunction, dementia (late) |
"Almost all PD patients experience improvement [with levodopa], and failure to respond to an adequate trial of levodopa should cause the diagnosis to be questioned." - Harrison's Principles of Internal Medicine 22E
B. Genetic / Familial Parkinson Disease
About 5-15% of PD is monogenic. Key genes:
| Gene | Inheritance | Age of Onset | Special Features |
|---|---|---|---|
| SNCA (α-synuclein) - PARK1/4 | Autosomal dominant | 30-40 years | A53T, A30P mutations; Lewy bodies present |
| PARK2 (Parkin) | Autosomal recessive | 20-40 years | Most common early-onset PD; no Lewy bodies; slow progression |
| LRRK2 (leucine-rich repeat kinase 2) - PARK8 | Autosomal dominant | Late onset | Most common AD cause; common in Ashkenazi Jews; variable pathology |
| PINK1 - PARK6 | Autosomal recessive | Variable | Mitochondrial gene |
| DJ-1 - PARK7 | Autosomal recessive | 30s | Oxidative stress response; slow progression |
| GBA1 (glucocerebrosidase) | Risk factor | Late | Most common genetic risk factor overall (~15% PD); Gaucher disease gene |
- Adams and Victor's Principles of Neurology, 12th Ed.
C. Atypical Parkinsonism ("Parkinsonism-Plus Syndromes")
These neurodegenerative conditions share parkinsonism with PD but have additional features and key differences:
- Symptoms tend to be more symmetric
- More rapid progression
- Paucity or absence of resting tremor
- Early postural instability (falls in first year)
- Poor or absent L-DOPA response
- Neuroanatomy Through Clinical Cases, 3rd Ed.
C1. Progressive Supranuclear Palsy (PSP)
Also known as Steele-Richardson-Olszewski syndrome
| Feature | Detail |
|---|---|
| Prevalence | ~5-6.4 per 100,000; most common atypical parkinsonism |
| Pathology | 4-repeat tau accumulation (FTLD-tau); globose neurofibrillary tangles; affects midbrain-diencephalic junction |
| Hallmark sign | Supranuclear vertical gaze palsy - especially downward gaze (patient cannot look down; retained on doll's-head maneuver) |
| Gait | Stiff, unstable, hyperextended neck; "gunslinger gait"; spectacular falls backward in first year |
| Posture | Axial rigidity (neck and trunk > limbs); contrasts with PD which has flexed posture |
| Cognition | Frontal-executive dysfunction, apathy, disinhibition, pseudobulbar affect |
| Neuropsychiatry | Prominent apathy, bradyphrenia, personality change mimicking bvFTD |
| MRI sign | "Hummingbird sign" - midbrain atrophy on sagittal MRI; small midbrain-to-pons ratio |
| L-DOPA response | Minimal to absent |
| Disease duration | ~5-7 years; death usually from aspiration pneumonia |
| PSP variants | PSP-Richardson syndrome (classic), PSP-parkinsonism (L-DOPA responsive), PSP-PAGF (pure akinesia with gait freezing), PSP-CBS, PSP-PNFA |
"PSP-RS begins with falls and executive dysfunction... a stiff, unstable posture with hyperextension of the neck and a slow, jerky, toppling gait are characteristic." - Harrison's Principles of Internal Medicine 22E
C2. Multiple System Atrophy (MSA)
Formerly known as Shy-Drager syndrome, striatonigral degeneration, olivopontocerebellar atrophy (OPCA)
| Feature | Detail |
|---|---|
| Prevalence | ~4.4 per 100,000 |
| Mean onset | ~54 years; mean survival ~5.7 years |
| Pathology | α-Synuclein inclusions (glial cytoplasmic inclusions, GCIs) in oligodendrocytes; degeneration of striatum, substantia nigra, cerebellum, pons, intermediolateral cell column of spinal cord |
| Core triad | Parkinsonism + Autonomic failure + Cerebellar ataxia (not all three required) |
| L-DOPA response | Poor (some initial response in MSA-P) |
| Cognitive impairment | Rare at diagnosis (dementia is a red flag against MSA) |
Two subtypes:
| MSA-P (parkinsonian) | MSA-C (cerebellar) | |
|---|---|---|
| Former name | Striatonigral degeneration | Olivopontocerebellar atrophy (OPCA) |
| Dominant feature | L-DOPA-poor parkinsonism | Cerebellar ataxia |
| Frequency (Europe) | 58% of MSA cases | 42% of MSA cases |
| Frequency (Japan) | Less common | 84% of MSA cases |
| MRI | Putaminal T2 abnormality; posterolateral putaminal hypointensity | "Hot cross bun sign" - cruciform T2 hyperintensity in pons; middle cerebellar peduncle atrophy |
Autonomic features (prominent in both subtypes):
- Orthostatic hypotension (>30 mmHg systolic drop on standing)
- Urogenital dysfunction - urinary incontinence, erectile dysfunction (often the first symptom in men)
- GI dysmotility
- Anhidrosis (central pattern on thermoregulatory sweat testing)
- REM sleep behaviour disorder (RBD)
- Stridor (from vocal cord paralysis - a dangerous, characteristic feature)
"Patients with MSA have loss of dopaminergic neurons of the substantia nigra pars compacta. However, there is also loss of striatal neurons projecting to the globus pallidus - therefore, even if dopaminergic transmission is enhanced pharmacologically, there will still be decreased inhibition of the basal ganglia output nuclei." - Neuroanatomy Through Clinical Cases, 3rd Ed.
C3. Corticobasal Degeneration (CBD) / Corticobasal Syndrome (CBS)
| Feature | Detail |
|---|---|
| Mean age of onset | ~64 years; disease duration ~6.6 years |
| Pathology | 4-repeat tau accumulation (same class as PSP); atrophy of superior frontal gyrus; thinning of corpus callosum; "balloon neurons" (achromatic neuronal inclusions); tau-positive astrocytic plaques |
| Hallmark | Asymmetric apraxia and rigidity (one limb far worse than the other) |
| Alien limb phenomenon | Patient's hand moves involuntarily, as if with a mind of its own - a near-pathognomonic feature |
| Other cortical signs | Cortical sensory loss, myoclonus (stimulus-sensitive), mirror movements |
| Motor features | Bradykinesia, dystonia of the affected limb, the hand may form a characteristic fist |
| Cognition | Executive dysfunction, visuospatial deficits; can present as bvFTD |
| MRI | Asymmetric frontoparietal atrophy contralateral to the affected limb |
| FDG-PET | Focal asymmetric hypometabolism in posterior frontal and anterior parietal regions |
| L-DOPA response | Poor |
Important distinction: The term CBS (corticobasal syndrome) = clinical syndrome; CBD = pathological entity. CBD accounts for only ~50% of CBS cases - other causes include PSP, AD, and CJD. - Bradley and Daroff's Neurology in Clinical Practice
C4. Dementia with Lewy Bodies (DLB)
| Feature | Detail |
|---|---|
| Prevalence | Second most common cause of dementia in the elderly (after Alzheimer) |
| Pathology | Widespread Lewy bodies (α-synuclein) in cerebral cortex (contrasts PD where they are predominantly brainstem); Lewy bodies also in intermediolateral cell column → autonomic failure |
| Relationship to PD | DLB and Parkinson disease dementia (PDD) are ends of a continuous spectrum ("Lewy body disease spectrum"). Convention: if dementia precedes or occurs within 1 year of motor symptoms = DLB; if motor symptoms precede dementia by >1 year = PDD |
| Core clinical features | Progressive cognitive decline + parkinsonism + the DLB triad: |
DLB diagnostic triad:
- Fluctuating cognition - dramatic fluctuations in alertness and attention (minutes to hours)
- Recurrent vivid visual hallucinations (well-formed, typically people or animals)
- Parkinsonism - usually mild, often no tremor or only slight tremor
Supportive features: REM sleep behaviour disorder (RBD), severe neuroleptic sensitivity (can cause neuroleptic malignant syndrome), reduced dopamine transporter on DaT-SPECT
| Feature | DLB | PD Dementia |
|---|---|---|
| Timing of dementia | Before or concurrent with parkinsonism | >1 year after motor symptoms |
| Tremor | Usually absent or mild | Present in most |
| L-DOPA response | Variable, often causes hallucinations | Usually good initially |
| Neuroleptic sensitivity | Extreme (can be fatal) | Moderate |
Warning: DLB patients are extremely sensitive to neuroleptics - even atypical antipsychotics can dramatically worsen parkinsonism or trigger neuroleptic malignant syndrome. - Adams and Victor's Principles of Neurology, 12th Ed.
PART 2 - SECONDARY (ACQUIRED) PARKINSONISM
D. Drug-Induced Parkinsonism (DIP)
The second most common cause of parkinsonism overall (accounting for ~20% of parkinsonism-plus presentations).
| Feature | Detail |
|---|---|
| Mechanism | Blockade or depletion of dopamine in nigrostriatal pathway |
| Key causative drugs | Antipsychotics (haloperidol, risperidone), antiemetics (metoclopramide, prochlorperazine), reserpine, tetrabenazine, valproate, cinnarizine/flunarizine |
| Clinical features | Symmetric parkinsonism (distinguishes from IPD); may include bradykinesia, rigidity, tremor |
| Risk factors | Increasing age, higher drug dose, prior history of parkinsonism, underlying basal ganglia damage |
| Key distinguishing feature | Reversible on drug withdrawal (weeks to months) - this is why it must be identified |
| L-DOPA response | Poor (dopamine receptors are blocked, not neurons lost) |
"Drug-induced parkinsonism accounted for 20% of cases of parkinsonism-plus conditions in a population-based study." - Textbook of Family Medicine 9e
E. Vascular Parkinsonism (VP)
| Feature | Detail |
|---|---|
| Cause | Cerebrovascular disease - lacunar infarcts or white matter changes affecting basal ganglia circuits |
| Subtypes | Acute/subacute (after a stroke affecting striatum - hemiparkinsonism); Insidious-onset (most common - progressive with white matter disease) |
| Distinguishing features | Predominantly lower body parkinsonism (shuffling gait, falls) with relative sparing of upper limbs; no rest tremor; early gait disorder; pyramidal signs; evidence of cerebrovascular disease on MRI |
| L-DOPA response | Variable and often limited |
F. Toxic Parkinsonism
| Toxin | Source | Mechanism |
|---|---|---|
| MPTP (1-methyl-4-phenyl-1,2,5,6-tetrahydropyridine) | Illicit heroin synthesis by-product | Converted to MPP+ in CNS → selective dopaminergic neurotoxin; typically no Lewy bodies |
| Carbon monoxide | CO poisoning | Basal ganglia damage (globus pallidus necrosis) |
| Manganese | Mining, welding | Affects basal ganglia; "manganism" |
| Pesticides/herbicides | Agricultural exposure | Epidemiologically linked to increased PD risk |
"MPTP is transported into the CNS, where it is oxidized to form MPP+, a mitochondrial toxin that is selectively taken up by, and damages, dopamine neurons, but typically without the formation of Lewy bodies." - Harrison's 22E
G. Post-Encephalitic Parkinsonism
- Von Economo's encephalitis lethargica (1918 influenza pandemic era) caused a characteristic post-infectious parkinsonism with oculogyric crises
- Patients could develop parkinsonism decades after acute encephalitis
- Now largely historical but remains in differential diagnosis; recent interest given reports of new-onset PD following SARS-CoV-2 infection
H. Metabolic / Heredodegenerative Causes
| Condition | Key Features |
|---|---|
| Wilson's disease | Autosomal recessive copper metabolism disorder; onset before age 40; Kayser-Fleischer rings; liver disease; wing-beating tremor; treatable with copper chelation |
| Hypothyroidism | Slowness mimicking bradykinesia; reversible with thyroid replacement |
| Normal pressure hydrocephalus (NPH) | Triad: gait apraxia + urinary incontinence + dementia; parkinsonism-like lower body gait; responds to CSF shunting |
| Juvenile Huntington's disease | Rigidity-dominant variant (Westphal variant); chorea may be absent initially |
| Chronic traumatic encephalopathy (CTE) | "Dementia pugilistica" in boxers; tau pathology; parkinsonism component |
| Machado-Joseph disease (SCA-3) | Autosomal dominant spinocerebellar ataxia with parkinsonism component |
Comparative Summary Table
| Feature | IPD | PSP | MSA | DLB | CBD | Drug-induced |
|---|---|---|---|---|---|---|
| Tremor | Rest (pill-rolling) | Rare | Rare | Rare/absent | Action/myoclonus | Variable |
| Symmetry | Asymmetric | Symmetric (axial) | Symmetric | Symmetric | Asymmetric | Symmetric |
| L-DOPA response | Excellent | None | Poor | Variable | Poor | None |
| Dementia | Late | Frontal-subcortical | Rare | Early/prominent | Frontal | No |
| Hallucinations | Late (with L-DOPA) | Rare | Rare | Early/prominent | Rare | No |
| Eye movements | Normal early | Vertical gaze palsy | Mild abnormality | Normal early | Saccadic abnormalities | Normal |
| Autonomic failure | Mild-moderate | Mild | Prominent | Moderate | Mild | Mild |
| Key sign | Rest tremor | Backward falls, downgaze palsy | Hot cross bun, stridor | Visual hallucinations + fluctuating cognition | Alien limb + apraxia | Symmetric, drug history |
| MRI sign | Usually normal | Hummingbird sign | Hot cross bun / putaminal rim | Normal/medial temporal atrophy | Asymmetric parietal atrophy | Normal |
| Progression | 10-15 years | 5-7 years | ~6 years | Variable | ~6.6 years | Reversible |
| Pathology | α-Synuclein (Lewy bodies) | 4R-Tau (tangles) | α-Synuclein (GCIs) | α-Synuclein (cortical Lewy bodies) | 4R-Tau (astrocytic plaques) | No specific pathology |
Key Clinical Red Flags Against Idiopathic PD
The following features suggest an alternative diagnosis (atypical or secondary parkinsonism):
-
Symmetric onset
-
Failure to respond to an adequate L-DOPA trial
-
Early falls (within 1st year)
-
Early dementia or visual hallucinations preceding motor symptoms
-
Vertical gaze palsy (→ PSP)
-
Prominent early autonomic failure (→ MSA)
-
Prominent cerebellar signs (→ MSA-C)
-
Alien limb or cortical sensory loss (→ CBD)
-
Neuroleptic drug exposure (→ drug-induced)
-
Liver disease or age <40 (→ Wilson's disease)
-
Harrison's Principles of Internal Medicine 22E, p.3544; Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.