Give me case of pcos for practical examination
Reading File
Finding Sources
Searching the Web
PCOS polycystic ovary syndrome practical examination case presentation clinical features
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed to construct a comprehensive practical examination case. Here it is:
PCOS — Practical Examination Case
CASE PRESENTATION
Patient: Miss S.K., 24-year-old unmarried female
Chief Complaints:
- Irregular menstrual cycles for 3 years
- Excessive facial and body hair for 2 years
- Weight gain for 2 years
- Multiple acne lesions on face and back
HISTORY OF PRESENT ILLNESS
A 24-year-old woman presents with oligomenorrhea (cycles every 35–90 days, lasting 2–3 days), excessive hair growth on the upper lip, chin, chest, and abdomen, and progressive weight gain of 12 kg over 2 years. She also reports acne unresponsive to topical treatment. Menarche was at age 13; her cycles were irregular from the start. She has no galactorrhea, no heat/cold intolerance, no symptoms of Cushing's syndrome. She is not on any medications.
Past History: No major illnesses. No surgeries.
Family History: Mother has type 2 diabetes; sister has irregular periods.
Personal/Social: Not sexually active. No tobacco, alcohol, or drug use.
EXAMINATION FINDINGS
General
- Obese female, BMI 32 kg/m²
- Acanthosis nigricans at the nape of neck and axillae (marker of insulin resistance)
Vitals
- BP: 128/82 mmHg | PR: 82/min | RR: 16/min | Temp: 37°C
Dermatological (Androgen Excess Signs)
- Ferriman-Gallwey hirsutism score: 14 (≥8 = clinically significant hirsutism)
- Comedonal and inflammatory acne on face and upper back
- Moderate androgenic alopecia (bitemporal thinning)
- Acanthosis nigricans in skin folds
Abdominal
- Central obesity; waist circumference 92 cm
- No palpable abdominal/pelvic mass
Gynaecological
- Uterus normal sized; bilateral ovaries slightly enlarged (palpable per abdominally)
INVESTIGATIONS
| Investigation | Result | Significance |
|---|---|---|
| Serum total testosterone | 72 ng/dL (elevated; normal <50) | Hyperandrogenemia |
| LH : FSH ratio | 2.8 : 1 (>2:1) | Classic PCOS pattern |
| Serum LH | 14.2 IU/L (elevated) | Inappropriately elevated |
| Serum FSH | 5.1 IU/L (low-normal) | Relatively suppressed |
| Fasting insulin | 28 µIU/mL (elevated) | Hyperinsulinemia |
| Fasting glucose | 98 mg/dL | Impaired fasting glucose trend |
| HOMA-IR | 6.8 (>2.5 = IR) | Insulin resistance |
| HbA1c | 5.7% | Pre-diabetes range |
| Prolactin | 14 ng/mL (normal) | Excludes hyperprolactinemia |
| TSH | 2.1 mIU/L (normal) | Excludes thyroid disorder |
| DHEA-S | Mildly elevated | Adrenal androgen contribution |
| 17-OH Progesterone | 1.2 ng/mL (normal) | Excludes non-classical CAH |
| Lipid profile | TG 180 mg/dL, HDL 38 mg/dL | Dyslipidemia |
Pelvic Ultrasound (Transvaginal)
- Both ovaries enlarged: Right ovary 12 cm³, Left ovary 13 cm³ (normal <10 cm³)
- ≥12 follicles (2–9 mm diameter) per ovary arranged in a "string of pearls" periphery
- Increased stromal echogenicity and volume
- Uterine endometrium: 8 mm (proliferative)
DIAGNOSIS
Working Diagnosis: Polycystic Ovary Syndrome (PCOS)
Applying the Rotterdam Criteria (2003) — diagnosis requires 2 of 3:
| Criterion | Present? |
|---|---|
| 1. Oligo/anovulation (oligomenorrhea) | ✅ Yes |
| 2. Clinical/biochemical hyperandrogenism | ✅ Yes (hirsutism + elevated testosterone) |
| 3. Polycystic ovaries on ultrasound | ✅ Yes |
All three criteria are fulfilled. Other causes excluded (TSH normal, prolactin normal, 17-OHP normal, no features of Cushing's).
DIFFERENTIAL DIAGNOSIS
- Non-classical Congenital Adrenal Hyperplasia (CAH) — excluded by normal 17-OH progesterone
- Hyperprolactinemia — excluded by normal prolactin
- Hypothyroidism — excluded by normal TSH
- Cushing's Syndrome — no striae, no proximal myopathy, no moon face
- Androgen-secreting ovarian/adrenal tumour — testosterone not markedly elevated (>200 ng/dL would raise suspicion); onset gradual
PATHOPHYSIOLOGY (Viva Points)
Genetic predisposition + Obesity
↓
Insulin Resistance → Compensatory Hyperinsulinemia
↓
↑ LH pulsatility from hypothalamus
↓
Theca cells → ↑ Androgen production (testosterone, androstenedione)
↓
Excess androgens → Inhibit follicular maturation → Follicular arrest
↓
Multiple small antral follicles (≤9 mm) → Polycystic appearance
↓
Anovulation → No corpus luteum → No progesterone
↓
Oligomenorrhea / Amenorrhea + Unopposed estrogen → Endometrial hyperplasia risk
"A dysregulation of enzymes involved in androgen biosynthesis results in excessive androgen production, which is considered a central feature of PCOS." — Robbins Basic Pathology
MANAGEMENT
1. Lifestyle Modification (First-Line)
- Caloric restriction (500 kcal/day deficit) + regular aerobic exercise
- Even 5% weight loss improves menstrual regularity, insulin sensitivity, and fertility outcomes
- Target BMI <25 kg/m²
2. Medical Management
If pregnancy NOT desired:
| Drug | Dose | Purpose |
|---|---|---|
| Combined OCP (ethinylestradiol + levonorgestrel/drospirenone) | 1 tablet daily cyclically | Cycle regulation, anti-androgenic, endometrial protection |
| Metformin | 1500–2000 mg/day in divided doses | Insulin sensitiser; reduces androgens; may restore ovulation in 60–70% |
| Spironolactone | 50–100 mg/day | Anti-androgen for hirsutism (add to OCP) |
If pregnancy desired:
| Drug | Dose | Purpose |
|---|---|---|
| Letrozole (preferred) | 5 mg on days 3–7 of cycle | Aromatase inhibitor; ovulation induction (superior to clomiphene in PCOS) |
| Clomiphene citrate | 50 mg on days 3–7 | SERM; ovulation induction (alternative) |
| Metformin | Adjunct | Improves ovulation induction response |
"Letrozole is the preferred therapy; 75–80% of women conceive with such therapy." — Goldman-Cecil Medicine
3. Monitoring and Complications Screening
Per the diagnostic flowchart above:
- Endometrial protection: Progesterone-induced bleed ≥4×/year if not on OCPs; ultrasound/biopsy if risk factors
- Metabolic syndrome: Annual fasting glucose, HbA1c, lipid profile
- Hypertension: Regular BP monitoring
- Obstructive sleep apnoea: Screen with Epworth Sleepiness Scale (obesity + PCOS)
- Mood disorders: Screen for depression/anxiety (common in PCOS)
4. Surgical (Last Resort)
- Laparoscopic ovarian drilling (LOD): Multiple ovarian punctures by diathermy/laser; achieves unifollicular ovulation; reserved for medical treatment failure; risk of adhesions
DIAGNOSTIC FLOWCHART
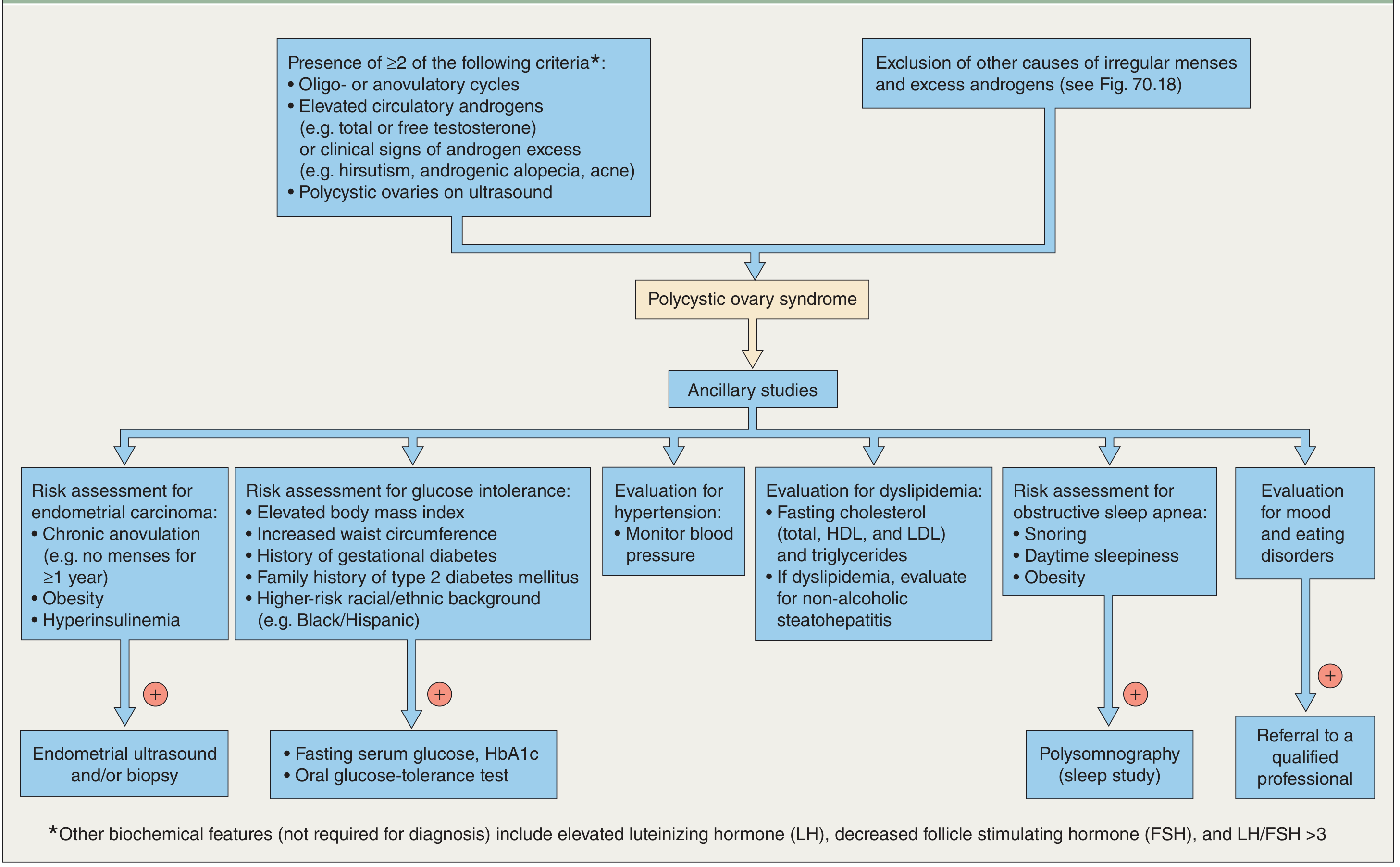
Dermatology 5e — Evaluation and ancillary studies after PCOS diagnosis
LONG-TERM COMPLICATIONS (Important for Viva)
| System | Complication |
|---|---|
| Metabolic | Type 2 DM (>50% by age 40), metabolic syndrome |
| Cardiovascular | Dyslipidaemia, hypertension, increased CVD risk |
| Oncological | Endometrial hyperplasia/carcinoma (unopposed oestrogen) |
| Reproductive | Infertility, increased miscarriage rate, gestational diabetes |
| Dermatological | Hirsutism, acne, androgenic alopecia |
| Psychological | Depression, anxiety, eating disorders |
VIVA VOCE QUESTIONS
Q1. What are the Rotterdam criteria?
Any 2 of 3: (i) oligo/anovulation, (ii) clinical or biochemical hyperandrogenism, (iii) polycystic ovaries on USG — after excluding other causes.
Q2. What is the LH:FSH ratio in PCOS?
Typically >2:1 (often 3:1), due to increased LH pulsatility. However, it is not required for diagnosis.
Q3. Why does PCOS cause anovulation?
Excess LH stimulates theca cells → excess androgens → inhibit follicular maturation → arrest at antral stage → no dominant follicle → no LH surge → anovulation.
Q4. Why is unopposed oestrogen dangerous in PCOS?
Chronic anovulation → no corpus luteum → no progesterone → unopposed oestrogen → endometrial proliferation → risk of endometrial hyperplasia and carcinoma.
Q5. What is acanthosis nigricans and its significance here?
Velvety hyperpigmented skin in flexural areas (neck, axillae, groin); marker of insulin resistance. Seen in ~50% of PCOS patients.
Q6. Histology of polycystic ovary?
Ovaries twice normal size, thickened fibrotic capsule, multiple subcortical follicular cysts (0.5–1.5 cm), hyperplastic luteinized theca interna, absent corpora lutea (due to anovulation). — Robbins Basic Pathology
Q7. Why is letrozole preferred over clomiphene for ovulation induction in PCOS?
Letrozole (aromatase inhibitor) has shorter half-life (48 hrs vs 2 weeks for clomiphene), reduces peripheral oestrogen feedback, and has better live birth rates in PCOS with fewer multiple pregnancies.
Sources: Goldman-Cecil Medicine (International Ed.), Robbins & Kumar Basic Pathology, Berek & Novak's Gynecology, Textbook of Family Medicine 9e, Dermatology 5e
This is a shared conversation. Sign in to Orris to start your own chat.